
Abstract
PURPOSE Federally qualified health centers provide care to medically underserved populations, the same individuals often underrepresented in the electoral process. These centers are unique venues to access patients for voter registration services.
METHODS We undertook a clinician-led, nonpartisan voter registration drive within 2 university-affiliated federally qualified health centers in the Bronx, New York. Patients were approached by voter registration volunteers in clinic waiting areas during a 12-week period.
RESULTS Volunteers directly engaged with 304 patients. Of the 128 patients who were eligible and not currently registered, 114 (89%) registered to vote through this project. This number corresponded to 38% of all patients engaged. Sixty-five percent of new registrants were aged younger than 40 years.
CONCLUSIONS This project was successful in registering clinic patients to vote. Clinics are not only health centers, but also powerful vehicles for bringing a voice to civically disenfranchised communities.
- voter registration
- civic engagement
- primary care
- family practice
- social participation
- vulnerable populations
INTRODUCTION
In the United States, voting is a fundamental right of citizenship and represents the power to influence societal conditions that affect health conditions. Despite this opportunity, only 42.5% (93 million) of the American electorate voted in the 2012 presidential election.1 Low voter turnout is even more of a challenge in local elections. In 2009, just 18.4% of voters cast a ballot in the New York City mayoral election, the lowest turnout since 1969.2 This phenomenon may lead to skewed health policy outcomes that favor more civically active citizens.2,3
The demographic composition of a community can predict low voter turnout. Whites vote at a rate 10% higher than blacks and 50% higher than Latinos and Asians nationally.3 Low household income, young age, and residential mobility are also major predictors.2,4–6 The Bronx community is particularly vulnerable. It is the poorest urban county in the United States, with 29% of its residents living at or below the poverty level.7 Additionally, Bronx residents experience high rates of residential mobility.8 Twelve percent of residents change addresses within 1 year of moving to a new address.9 In many ways, social disparities mirror health disparities in that inequitable distribution of health resources and disproportionate adverse health outcomes affect these same groups.10
The magnitude of voter disparity is especially great among individuals who are likely to receive care at federally qualified health centers (FQHCs). These patients are most often Medicaid eligible, uninsured, and low income. Offering voter services in this setting allows increased access to potential voters, facilitates civic participation, and enables patients to get involved to improve community health. Additionally, the National Voter Registration Act of 1993 empowers FQHCs to provide voter services. Under the law, offices that provide public assistance, including Medicaid services, are considered voter registration agencies.11
The National Association of Community Health Centers (NACHC), a nonprofit association of health centers, ran a successful national voter registration campaign in community health centers in 2008. Clinicians and health center staff registered more than 18,000 individuals in preparation for the 2008 presidential election, proving that community health centers can successfully conduct voter registration campaigns.12 Building on the NACHC Community Health Vote toolkit, we developed a nonpartisan, clinician-led voter registration initiative within 2 Bronx FQHCs in preparation for the 2012 presidential election.
METHODS
Settings
Voter registration was conducted at the Williamsbridge Family Practice and the Family Health Center, 2 FQHCs in the Bronx, New York. These sites serve as medical student, family medicine residency, and faculty practice sites for the Department of Family and Social Medicine at Montefiore Medical Center/Albert Einstein College of Medicine. A unique aspect of the department’s residency curriculum addresses social justice and health disparities.13 The clinics are managed in collaboration with the Bronx Community Health Network, a community advocacy and service organization.
The clinics are located in different communities in the Bronx, but the demographic makeup of the 2 communities is largely similar. Seventy-eight percent of Williamsbridge Family Practice and 79% of Family Health Center community residents self-identify as black or Latino, 33% and 35% are foreign-born, and 55% and 64% have at most a high school education, respectively. The Family Health Center community is somewhat more impoverished, with 33% of residents living at or below the poverty line, compared with 16% in the Williamsbridge Family Practice community.14,15
Procedures
Voter registration took place from August 1 to October 12, 2012. The project was implemented in 3 phases: administrative approval, volunteer recruitment and training, and voter registration. We obtained approval for this project after meeting with clinic and hospital leadership over several months. In these discussions, we highlighted the role of community health centers as federally supported locations to conduct voter registration. We also stressed the importance of using clinics to address disparities in civic participation, a powerful social determinant of health.
Clinic staff, nurses, physicians, Bronx Community Health Network community board members, and Bronx area college students were recruited as volunteers. Two Bronx area college students and 2 Department of Family and Social Medicine resident physicians spearheaded the effort. Volunteers attended a 2-hour training session conducted after-hours by the National League of Women Voters. The training covered voter registration rules and eligibility. Twenty volunteers were recruited in total: 13 provided basic information to potential voters, and 8 received an additional hour of training to answer patient questions and register them to vote. Of the 8 volunteers with special training, 2 were students, 2 were resident physicians, 2 were attending physicians, and 2 were clinic staff. Volunteer time varied from 3 to 8 hours weekly and volunteers staffed 50% of the clinic sessions.
We developed a 3-pronged strategy to efficiently register patients to vote as part of the regularly scheduled clinic visit: direct engagement with patients by volunteers, education about voting laws in New York, and voter registration. Patient-volunteer interactions took place at all areas of the patient flow: during waiting times in common areas, during appointment registration, when vital signs were taken, and before or after the physician encounter in the examination room. Voter registration took an average of 5 to 7 minutes to complete. It was conducted in a nonpartisan manner and patients were not instructed on candidates’ positions.
Patients were asked if they were interested in learning more about voting as part of a clinic-driven voter registration effort. If they expressed interest, they were referred to a specially trained volunteer who could answer questions regarding incarceration, citizenship, language and disability barriers, and changes in name or address as they pertain to voting. Volunteers then administered a 2-minute questionnaire to collect patient demographics and assessed voting eligibility using the New York City Board of Elections criteria (Supplemental Appendix 1). Patients were considered eligible if they would be 18 years or older at the time of the presidential election, were US citizens, and were not on parole for a felony conviction. Patients were asked their age and sex, if they had ever voted in the past, and if they had changed their name or address since the last election in which they voted. If patients were eligible and agreed to register, they were given a voter registration card to complete on site. All completed registration cards were mailed to the Board of Elections on behalf of the patient, or mailed by the patient. Patients were told to expect mail correspondence from the Board of Elections regarding their polling location, and voting day policies and procedures. Both eligible and ineligible patients were given written materials that included information for voters and political party platforms, and charged to spread the word about voting in their community (Supplemental Appendixes 2 and 3).
The primary outcomes of the intervention were voter engagement through patient-volunteer interactions and voter registration. Patients were considered to have engaged with volunteers if they agreed to speak with a volunteer about voter registration. They were considered to have registered to vote if they were eligible and either accepted a voter registration card with the intent to complete it or completed a card on site. Descriptive statistics of aggregate data were reported for this project.
The Committee on Clinical Investigation at Albert Einstein College of Medicine approved this project.
RESULTS
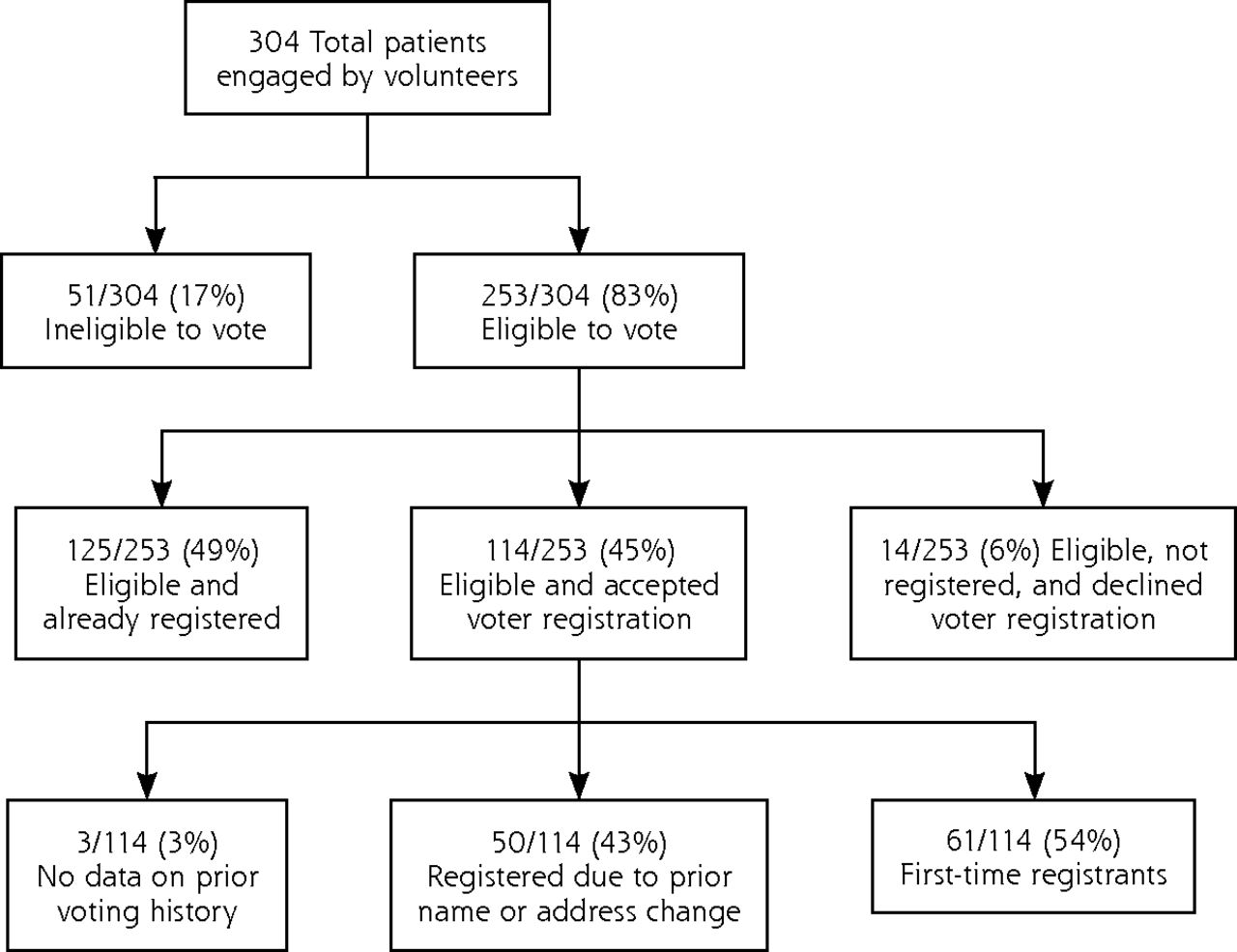
Demographic information for new registrants is shown in Table 1. Volunteers directly engaged with 304 patients (Figure 1). Of these individuals, 253 (83%) were eligible to vote, whereas the rest were ineligible. Of the 128 patients eligible to vote and not currently registered, 114 (89%) registered to vote through this project. Of the 114 patients, 61 (54%) were first-time registrants, 50 (43%) were re-registered because of prior name or address change, and 3 (3%) had no data on prior voting history. Thirty-eight percent of the total patients engaged were registered to vote. Sixty-five percent of registrants were aged younger than 40 years.

Schema and results of clinic-based voter registration.
Patients Registered in Clinic-Based Voter Registration Project (n = 114)
DISCUSSION
Our project was successful in registering 89% of the eligible voters through clinic-based voter registration. The fact that almost one-half of new voters were re-registrants because of changes in demographics highlights barriers in the current voter registration process. In communities with high levels of socioeconomic stress, easing access to voter services becomes increasingly important. In New York City, citizens can register to vote in person or by mail; however, lack of individual initiative, time constraints, work schedules, limited income, and transportation issues can make this process more difficult. Individuals who hold a valid New York State identification card can register online, but access to the Internet may be problematic in resource-poor settings.
This project is also an instructive example of how health care professionals can address broader social determinants of health through clinic interventions. Health is determined in part by access to care, which the Affordable Care Act seeks to address.16 It is also influenced by the environmental conditions in which people live, however. Community safety, quality education, access to jobs, and availability of green space may carry less importance than chronic disease in the clinical setting. But all too often, through neglect of these issues, clinicians miss opportunities to affect population-level change. Addressing social determinants is a necessary aspect of comprehensive care in that it considers patients an integral part of their communities. The National Committee for Quality Assurance recently expanded its patient-centered medical home definition to include an emphasis on care management of high-need populations, which includes addressing social determinants of health.17
Multiple factors contributed to the success of this project. Active patient engagement at several stages of the clinic visit not only increased access to voter services, but also eliminated the need for patient initiative to seek out these services. Additionally, it was critical to have at least 1 volunteer wholly dedicated to troubleshooting questions and actively registering patients to vote. This strategy reduced the additional time and energy cost to clinic staff in a setting where time is a precious commodity.
The small number of volunteers conducting voter registration was a major limitation of the study impact. A total of 4,500 patients visited our health centers during the study period and during clinic sessions when volunteers were on site to conduct voter registration. We engaged a small fraction (7%) of the total, potentially eligible patients because of limited volunteer capacity. With more volunteers, this intervention could have a much larger impact on civic engagement in medically underserved communities. Additionally, voter registration was conducted in English and Spanish only. The Family Health Center has a large Vietnamese and Cambodian community that was not adequately reached because of language barriers.
There were few unintended consequences of the study. Most patients expressed interested in voter registration; however, some patients experienced stress when asked about citizenship status. It was important to reassure them that the information collected was being used for research purposes only and would not be shared with the Immigration and Naturalization Service.
This project may serve as a clinic model for civic engagement and for other interventions that address social determinants of health. Its success has many implications for the future of health centers across the country. If health centers step up their role in community civic activism, they can act as powerful vehicles for bringing a voice to communities underrepresented in the electoral process.
Footnotes
-
Conflicts of interest: authors report none.
-
Supplementary materials: Available at http://www.annfammed.org/content/12/5/466/suppl/DC1/
- Received for publication September 18, 2013.
- Revision received May 16, 2014.
- Accepted for publication May 21, 2014.
- © 2014 Annals of Family Medicine, Inc.
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- US doctors and hospitals offer a new treatment: voter registration
- Supporting patients to shape social determinants of health through democratic engagement
- Aider les patients a faconner les determinants sociaux de la sante par un engagement democratique
- Addressing Health Disparities Through Voter Engagement
- In This Issue: Raise the Gaze