
Article Figures & Data
Figures
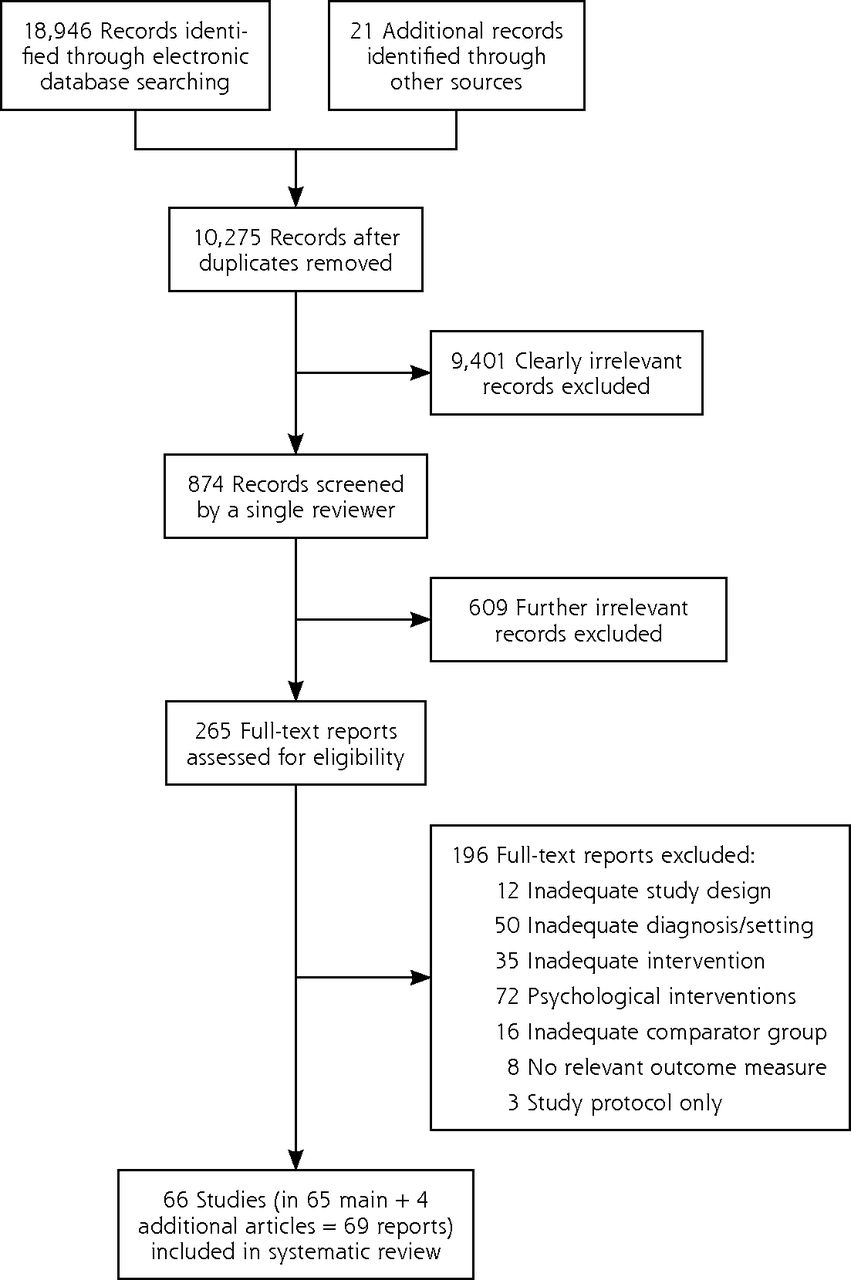
- Figure 1
Study selection process.
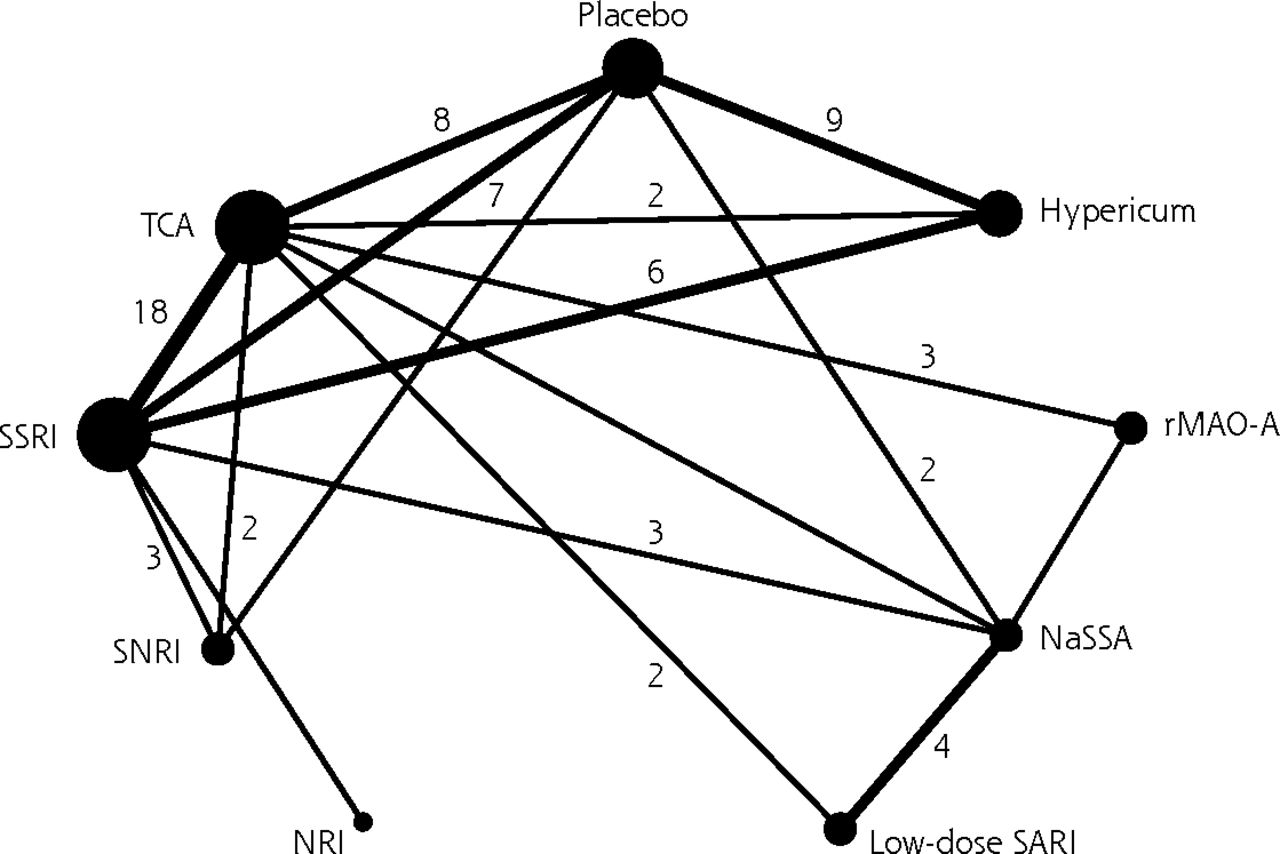
- Figure 2
Network for the main efficacy outcome response.
Figures indicate the number of direct comparisons (lines without figure indicate 1 comparison)
Hypericum = extract from Hypericum perforatum L.; NaSSA = noradrenergic and specific serotonergic antidepressive agent (mianserin, mirtazapine); NRI = noradrenaline reuptake inhibitor (reboxetine); rMAO-A = reversible inhibitor of monoaminoxidase A (moclobemide, minaprine); SARI = serotonin (5-HT2) antagonist and reuptake inhibitor (trazodone); SNRI = serotonin-noradrenaline reuptake inhibitor (venlafaxine); SSRI = selective serotonin reuptake inhibitor; TCA = tricyclic and tetracyclic antidepressant.


Tables
- Table 1
Overview of Antidepressant Medications Tested in the Included Trials and in the Meta-Analysis
Medication Class Trial Groups/Arms and Specific Medication Tested TCA, tricyclic and tetracyclic antidepressants 40 Separate groups in trials, after pooling of groups in studies with more than 1 TCA, 37 arms in analyses 14 Amitriptyline (1 pooling of 2 groups with different dosages, 1 pooled with dothiepin) 8 Imipramine (1 pooled with desipramine) 8 Dothiepin/dosulepin (1 pooled with amitriptyline) 3 Clomipramine 1 Amineptine 1 Desipramine (pooled with imipramine) 1 Doxepin 1 Lofepramine 1 Maprotiline 1 Tianeptine 1 Individualized TCA SSRI, selective serotonin reuptake inhibitors 38 Arms in total, 37 after pooling of 2 arms in a study with 2 SSRI 35 arms 12 Paroxetine 9 Fluoxetine 5 Sertraline 5 Citalopram (1 pooled with escitalopram) 2 Fluvoxamine 3 Escitalopram (1 pooled with citalopram) 1 Individualized SSRI SNRI, serotonin-noradrenaline reuptake inhibitor 6 Arms in total
6 VenlafaxineNRI, noradrenaline reuptake inhibitor 1 Arm in total
1 ReboxetineSARI, serotonin (5-HT2) antagonists and reuptake inhibitor 5 Arms in total
5 TrazodoneNaSSA, noradrenergic and specific serotonergic antidepressive agents 9 Arms in total
8 Mianserin (2 underdosing)
1 MirtazapinerMAO-A, reversible inhibitors of monoaminoxidase A 8 Arms in total, 6 in analyses
4 Moclobemide,
4 Minaprine (2 pooling of different dosages)Hypericum, extracts from Hypericum perforatum L. (St. John’s wort) 15 Arms in total, 14 after pooling of 2 arms testing different extracts in 1 study; 12 different extracts Characteristic Publication Year 1996 (1971, 2012) Number of patients Total 15,161 Median (minimum, maximum) 162 (21, 1,385) Diagnosis, No. (%) Major depression only 38 (58) Mixed/unclear 25 (38) Minor depression/dysthymia 3 (5) Classification of depression, No. (%) Diagnostic and Statistical Manual of Mental Disorders (Fourth Edition) 15 (23) Diagnostic and Statistical Manual of Mental Disorders (Third Edition) 24 (36) International Classification of Diseases, Tenth Revision 6 (9) International Classification of Diseases, Ninth Revision 4 (6) Research Diagnostic Criteria 4 (6) Not reported/other 13 (20) Restricted to patients >55 y, No. (%) 8 (12) Median length of treatment in weeks (minimum, maximum) 6 (4, 52) Overall risk of bias, No. (%) High (high risk in 1 or more items) 32 (49) Unclear (no item high risk, <3 low risk) 23 (35) Low (at least 3 low, no high risk) 11 (17) Data available for meta-analysis, No. (%) Response 59 (89) Remission 55 (83) Total number of patients dropping out 60 (91) Number of patients dropping out due to adverse effects 58 (88) Number of patients reporting adverse effects 40 (61) - Table 3
Results of Conventional and Network Meta-Analyses for the Main Efficacy Outcome Response
Medication TCA SSRI SNRI NRI Low-Dose SARI NaSSA rMAO-A Hypericum Placebo TCA OR (95% CI)a 0.95 (0.84–1.08) 0.83 (0.37–1.89) na 1.43 (0.60–3.42) 3.83 (1.67–8.75) 1.65 (1.16–2.34) 0.87 (0.54–1.41) 1.67 (1.24–2.25) No. of studies; I2, %; P valueb 18; 0; .45; 2; 55; 0.14 na 2; 79; .03 1 3; 0; .79; 2; 24; 0.25; 8; 25; .23; OR (95% CI)c 1.04 (0.88–1.21) 1.00 (0.71–1.40) 1.23 (0.73–2.14) 0.97 (0.65–1.47) 1.55 (1.11–2.18) 1.65 (1.10–2.45) 0.86 (0.67–1.10) 1.75 (1.42–2.15) SSRI OR (95% CI)a 1.05 (0.93–1.19) 0.92 (0.67–1.25) 1.18 (0.85–1.65) na 1.05 (0.54–2.03) na 0.88 (0.63–1.23) 1.57 (1.31–1.89) No. of studies; I2, %; P valueb 18; 0; .45 4; 64; .04 1 na 3; 60; .08 na 6; 46; .10 7; 0; .83 OR (95% CI)c 0.97 (0.82–1.13) 0.96 (0.71–1.29) 1.19 (0.71–2.04) 0.94 (0.63–1.43) 1.50 (1.06–2.11) 1.60 (1.03–2.54) 0.83 (0.66–1.04) 1.69 (1.40–2.04) SNRI OR (95% CI)a 1.20 (0.53–2.72) 1.09 (0.79–1.49) na na na na na 1.94 (0.96–3.93) No. of studies; I2, %; P valueb 2; 55; .14 4; 64; .04 na na na na na 1 OR (95% CI)c 1.00 (0.72–1.41) 1.03 (0.77–1.42) 1.23 (0.67–2.28) 0.97 (0.60–1.63) 1.55 (1.02–2.45) 1.65 (0.98–2,80) 0.86 (0.59–1.24) 1.75 (1.24–2.47) NRI OR (95% CI)a na 0.84 (0.61–1.18) na na na na na na No. of studies; I2, %; P valueb na 1 na na na na na na OR (95% CI)c 0.60 (0.41–0.91) 0.63 (0.41–0.87) 0.61 (0.36–1.02) 0.79 (0.41–1.57) 0.94 (0.58–1.54) 1.34 (0.66–2.70) 0.52 (0.32–0.84) 1.42 (0.81–2.49) Low-dose SARI OR (95% CI)a 0.70 (0.29–1.67) na na na 2.11 (1.37–3.25) na na na No. of studies; I2, %; P valueb 2; 79; .03 na na na 4; 0; .56 na na na OR (95% CI)c 1.03 (0.68–1.55) 1.06 (0.70–1.58) 1.03 (0.61–1.67) 1.26 (0.63–2.47) 1.60 (1.07–2.42) 1.70 (0.96–2.89) 0.89 (0.58–1.38) 1.80 (1.17–2.76) NaSSA OR (95% CI)a 0.26 (0.11–0.60) 0.95 (0.49–1.85) na na 0.47 (0.31–0.73) 1.07 (0.49–2.34) na 1.34 (0.85–2.10) No. of studies; I2, %; P valueb 1 3; 60; .08 na na 4; 0; .56 1 na 2; 0; .98 OR (95% CI)c 0.64 (0.46–0.93) 0.67 (0.47–0.95) 0.64 (0.41–0.98) 0.79 (0.42–1.45) 0.63 (0.41–0.93) 1.06 (0.65–1.72) 0.55 (0.37–0.82) 1.13 (0.78–1.62) rMAO-A OR (95% CI)a 0.61 (0.43–0.86) na na na na 0.93 (0.43–2.03) na na No. of studies; I2, %; P valueb 3; 0; .79 na na na na 1 na na OR (95% CI)c 0.61 (0.41–0.91) 0.63 (0.41–0.97) 0.61 (0.36–1.02) 0.74 (0.37–1.52) 0.59 (0.35–1.04) 0.94 (0.58–1.54) 0.52 (0.32–0.84) 1.06 (0.67–1.66) Hypericum OR (95% CI)a 1.15 (0.71–1.85) 1.14 (0.81–1.59) na na na na na 2.02 (1.41–2.88) No. of studies; I2, %; P valueb 2; 24; .25 6; 43; .12 na na na na na 9; 43; .08 OR (95% CI)c 1.16 (0.81–1.50) 1.20 (0.96–1.51) 1.16 (0.80–1.68) 1.43 (0.81–2.64) 1.13 (0.72–1.73) 1.80 (1.21. 2.67) 1.92 (1.20–3.16) 2.03 (1.63–2.53) -
CI = confidence interval; CI = credible interval; hypericum = extract from Hypericum perforatum L.; rMAO-A = reversible inhibitor of monoaminoxidase A (moclobemide, minaprine); na = not available; NaSSA = noradrenergic and specific serotonergic antidepressive agent (mianserin, mirtazapine); NRI = noradrenaline reuptake inhibitor (reboxetine); OR = odds ratio; SARI = serotonin (5-HT2) antagonist and reuptake inhibitor (trazodone); SNRI = serotonin-noradrenaline reuptake inhibitor (venlafaxine); SSRI = selective serotonin reuptake inhibitor; TCA = tricyclic and tetracyclic antidepressant.
Note: Odds ratios >1 indicate more study discontinuation in patients receiving the treatment given in the row heading.
-
↵a Conventional meta-analysis of within-study comparisons with pooled odds ratios.
-
↵b Studies with direct comparisons available, with I2 value and P value from the χ2 test for heterogeneity.
-
↵c From network meta-analysis.
-
- Table 4
Results of Conventional and Network Meta-Analyses for the Main Acceptability Outcome Study Discontinuation Because of Adverse Effects
Medication TCA SSRI SNRI NRI Low-Dose SARI NaSSA rMAO-A Hypericum Placebo TCA OR (95% CI)a 1.15 (0.85–1.55) 0.86 (0.46–1.62) na 1.18 (0.46–3.01) 0.51 (0.18–1.42) 2.57 (1.18–5.60) 2.33 (.92–5.93) 2.30(1.10–4.81) No. of studies; I2, %; P value1 14; 43; .05 2; 0; .80 na 2; 54; .14 1 5; 47; .11 2; 0; .89 7; 24; .25 OR (95% CI)c 1.12 (0.84–1.47) 0.89 (0.55–1.37) 0.44 (0.18–1.06) 1.86 (0.92–3.75) 0.64 (0.36–1.14) 2.63 (1.49–5.09) 2.37 (1.28–4.49) 2.47 (1.59–3.84) SSRI OR (95% CI)a 0.87 (0.64–1.17) 0.81 (0.58–1.13) 0.39 (0.28–0.55) na 0.78 (0.42–1.44) na 1.48 (0.77–2.85) 1.86 (1.16–2.98) No. of studies; I2, %; P value1 14; 43; .05 4; 38; .18 1 na 3; 31; .23 na 6; 0; .92 8; 0; .64 OR (95% CI)c 0.89 (0.68–1.19) 0.79 (0.55–1.19) 0.39 (0.16–0.90) 1.65 (0.85–3.45) 0.57 (0.33–0.96) 2.34 (1.24–4.84) 2.11 (1.18–4.14) 2.20(1.44–3.36) SNRI OR (95% CI)a 1.16 (0.62–2.20) 1.24 (0.89–1.74) na na na na na 2.96 (0.90–9.73) No. of studies; I2, %; P value1 2; 0; .80 4; 38; .18 na na na na na 1 OR (95% CI)c 1.12 (0.73–1.81) 1.26 (0.84–1.83) 0.50 (0.19–1.23) 2.08 (0.95–4.85) 0.72 (0.36–1.37) 2.95 (1.41–6.69) 2.66 (1.33–5.57) 2.77 (1.58–4.87) NRI OR (95% CI)a 2.53 (1.81–3.53) na na na na na na No. of studies; I2, %; P value1 1 na na na na na na OR (95% CI)c 2.25 (0.95–5.48) 2.54 (1.11–6.37) 2.01 (0.82–5.20) 4.19 (1.59–12.48) 1.45 (0.58–3.74) 5.94 (2.09–17.13) 5.35 (1.99–14.94) 5.58 (2.28–13.66) SARI OR (95% CI)a 0.84 (0.33–2.15) na na na 0.28 (0.10–0.79) na na na No. of studies; I2, %; P value1 2; 54; .14 na na na 3; 58; 0.09 na na na OR (95% CI)c 0.54 (0.26–1.08) 0.61 (0.29–1.17) 0.48 (0.21–1.05) 0.24 (0.08–0.63) 0.35 (0.16–0.64) 1.42 (0.58–3.55) 0.78 (0.31–1.83) 1.33 (0.61–2.89) NaSSA OR (95% CI)a 1.97 (0.71–5.51) 1.28 (0.69–2.36) na na 3.55 (1.27–9.90) na na 3.52 (1.40–8.84) No. of studies; I2, %; P value1 1 3; 31; .23 na na 3; 58; .09 na na 2; 0; .90 OR (95% CI)c 1.56 (0.88–2.76) 1.75 (1.04–3.02) 1.39(0.73, 2.76) 0.69 (0.27–1.71) 2.89 (1.56–6.18) 4.10(1.81–10.38) 3.69 (1.71–8.56) 3.85 (2.05–7.25) rMAO-A OR (95% CI)a 0.39 (0.18–0.85) na na na na na na na No. of studies; I2, %; P value1 5; 47; .11 na na na na na na na OR (95% CI)c 0.38 (0.20–0.67) 0.43 (0.21–0.81) 0.34 (0.15–0.71) 0.17 (0.06–0.48) 0.71 (0.28–1.73) 0.24 (0.10–0.55) 0.90 (0.35–2.04) 0.94 (0.43–2.05) Hypericum OR (95% CI)a 0.43 (0.17–1.09) 0.68 (0.35–1.30) na na na na na 0.79 (0.31–1.97) No. of studies; I2, %; P value1 2; 0; 0.89 6; 0; .92 na na na na na 5; 0; .48 OR (95% CI)c 0.42 (0.22–0.78) 0.47 (0.24–0.85) 0.38 (0.18–0.75) 0.19 (0.07–0.50) 0.78 (0.31–1.83) 0.27 (0.11–0.58) 1.11 (0.49–2.83) 1.04 (0.53–2.06) -
CI = confidence interval; CI = credible interval; hypericum = extract from Hypericum perforatum L.; rMAO-A = reversible inhibitor of monoaminoxidase A (moclobemide, minaprine); na = not available; NaSSA = noradrenergic and specific serotonergic antidepressive agent (mianserin, mirtazapine); NRI = noradrenaline reuptake inhibitor (reboxetine); OR = odds ratio; SARI = serotonin (5-HT2) antagonist and reuptake inhibitor (trazodone); SNRI = serotonin-noradrenaline reuptake inhibitor (venlafaxine); SSRI = selective serotonin reuptake inhibitor; TCA = tricyclic and tetracyclic antidepressant.
Note: Odds ratios >1 indicate more study discontinuation in patients receiving the treatment given in the row heading.
-
↵a Conventional meta-analysis of within-study comparisons with pooled odds ratios.
-
b Studies with direct comparisons available, with I2 value and P value from the χ2 test for heterogeneity.
-
↵c From network meta-analysis.
-
The Article in Brief
Efficacy and Acceptability of Pharmacological Treatments for Depressive Disorders in Primary Care: Systematic Review and Network Meta-Analysis
Klaus Linde , and colleagues
Background Most cases of depression are seen and managed in primary care, however, most research on depression treatment involves specialty settings. Antidepresssant drugs are an important element of depression treatment, but there is ongoing debate about whether their relatively small effects over placebo are clinically relevant. This study analyzes existing randomized trials of pharmacological treatments of depression in primary care to investigate whether antidepressants are more effective than placebo and whether there are differences in efficacy and acceptability between different types of depression medications.
What This Study Found Antidepressants have short-term effects over placebo in primary care. SSRI (selective serotonin reuptake inhibitors) and TCA (tetracyclic antidepressants) have a somewhat more solid evidence base than other substance classes (with SSRI having a slightly better acceptability profile). Other pharmaceuticals (Hypericum, MAO-A, SNRI, NRI, NaSSa, SARI) showed some positive results, but due to limitations of the currently available evidence, a clear recommendation on their place in clinical practice remains difficult.
Implications
- The authors call for future research prioritizing large, long-term trials and observational studies addressing clinically relevant questions, such as the best management of mild-to-moderate depression and comparison of pharmacological and psychological treatments under conditions of routine care and stepped-care strategies.
Supplemental Appendix
Files in this Data Supplement:
- Supplemental data: Appendix - PDF file, 25 pages + cover
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- The relationship between antihypertensive medications and mood disorders: analysis of linked healthcare data for 1.8 million patients
- Maternal Fluoxetine Exposure Alters Cortical Hemodynamic and Calcium Response of Offspring to Somatosensory Stimuli
- Depression in primary care: part 2--management
- Polygenic risk scores for major depressive disorder and neuroticism as predictors of antidepressant response: meta-analysis of three treatment cohorts
- Effectiveness of online interventions in preventing depression: a protocol for systematic review and meta-analysis of randomised controlled trials
- A systematic review of network meta-analyses for pharmacological treatment of common mental disorders
- Pharmacological and non-pharmacological treatments for major depressive disorder: review of systematic reviews
- Incentives and disincentives for treating of depression and anxiety in Ontario Family Health Teams: protocol for a grounded theory study
- Comparative efficacy and acceptability of first-generation and second-generation antidepressants in the acute treatment of major depression: protocol for a network meta-analysis
- In This Issue: Policy and Practice
- Treatment of Depression in Primary Care