
Article Figures & Data
Figures
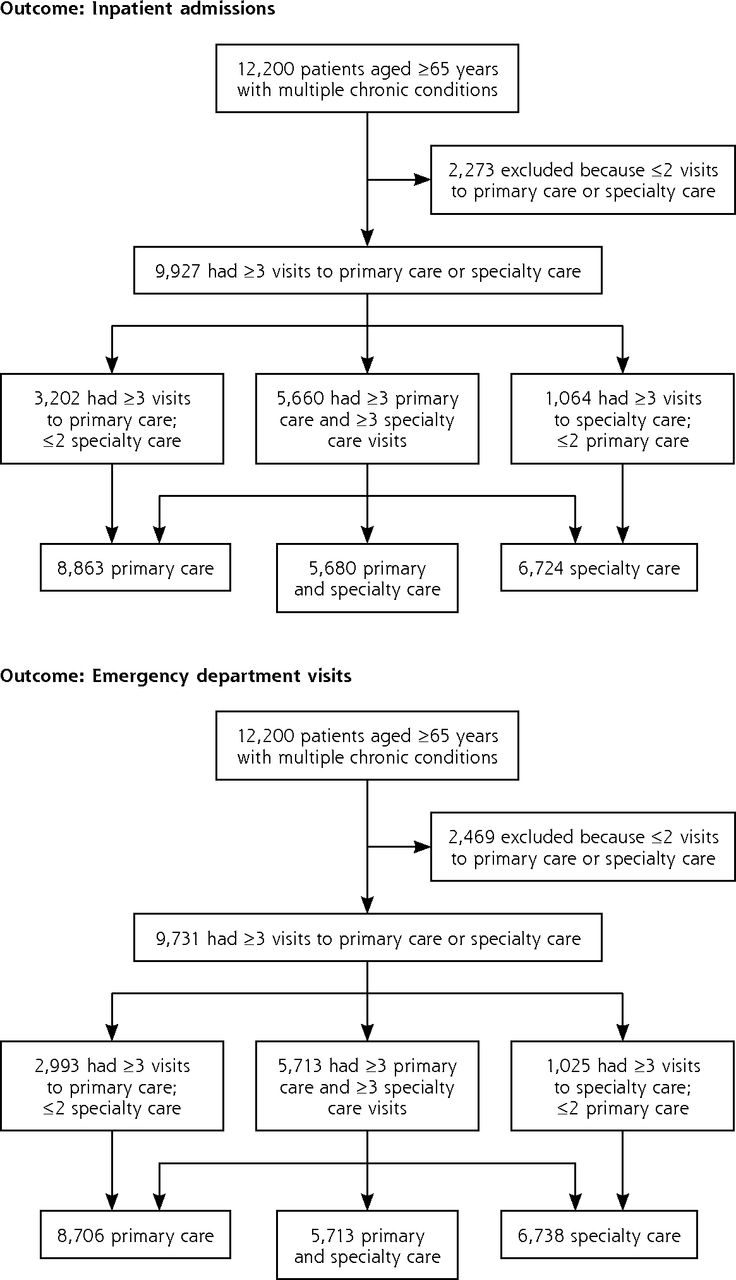
- Figure 1
Subcohorts used for analyses of each outcome.
Note: Numbers of visits refer to visits used to calculate Continuity of Care Index (between baseline and outcome).

Tables
Characteristic Inpatient Admissions Emergency Department Visits Primary Care a (n = 8,863) Mean (SD) Specialty Carea (n = 6,724) Mean (SD) Primary and Specialty Carea (n = 5,660) Mean (SD) Primary Carea (n = 8,706) Mean (SD) Specialty Carea (n = 6,738) Mean (SD) Primary and Specialty Carea (n = 5,713) Mean (SD) Age, y 76.0 (6.0) 75.8 (5.9) 76.0 (5.9) 75.9 (6.0) 75.8 (5.8) 76.0 (5.8) Morbidity burdenb 4.3 (2.4) 4.4 (2.5) 4.4 (2.5) 4.3 (2.5) 4.5 (2.5) 4.5 (2.5) Baseline visits, No. Primary care 3.8 (2.8) 3.8 (2.8) 4.0 (2.9) 3.7 (2.8) 3.7 (2.8) 3.9 (2.8) Specialty care 3.2 (3.6) 4.1 (3.9) 4.1 (4.0) 3.3 (3.7) 4.1 (4.0) 4.1 (4.0) COCIc Primary care 0.6 (0.3) – 0.6 (0.3) 0.6 (0.3) – 0.6 (0.3) Specialty care – 0.2 (0.2) 0.2 (0.2) – 0.2 (0.2) 0.2 (0.2) Percent Percent Percent Percent Percent Percent Female sex 56.4 55.0 55.4 55.6 54.2 54.2 Race/ethnicity White 78.8 80.8 81.0 79.1 81.1 81.2 Black 4.4 4.1 4.0 4.2 3.9 3.8 Hispanic 10.5 9.2 9.4 10.3 9.1 9.4 Other 1.8 1.7 1.6 1.8 1.7 1.7 Unknown 4.6 4.2 3.9 4.5 4.2 3.9 Low socioeconomic status 15.4 14.3 14.2 15.0 14.2 13.8 Baseline utilization Inpatient admissions 16.9 18.7 18.7 – – – Emergency department visits – – – 17.0 17.5 17.8 Experienced any outcomed 21.7 22.8 20.6 22.9 23.4 20.4 -
COCI = Continuity of Care Index.27
-
↵a Three visits required for subcohort entry.
-
↵b According to the Quan-adapted Elixhauser comorbidity index.28
-
↵c Last measured before outcome or censoring. Possible values range from 0 to 1 with higher scores indicating greater continuity.
-
↵d Hospital admission or emergency department visit.
-
- Table 2
Effect of Continuity of Care and Morbidity Burden on Adjusted Hazard Ratios of Inpatient Admissions
Predictive Variable Subcohorta Primary Care, HRb (95% CI) (n = 8,863) Specialty Care, HRb (95% CI) (n = 6,724) Primary and Specialty Care, HRb (95% CI) (n = 5,660) Primary care continuity (COCI) 0.97 (0.96–0.99)c – 0.99 (0.97–1.01) Specialty care continuity (COCI) – 0.95 (0.93–0.98)c 0.94 (0.92–0.97)c Morbidity burdend 1.12 (1.10–1.14)c 1.09 (1.06–1.11)c 1.09 (1.06–1.12)c -
COCI = Continuity of Care Index27; HR = hazard ratio.
-
↵a Three or more visits of any type required for subcohort membership.
-
↵b Adjusted for age, sex, race/ethnicity, socioeconomic status, and prior year primary care, specialty care, and baseline inpatient admissions. HR is for each 0.1-unit increase in COCI.
-
↵c Significant at P ≤.05.
-
↵d According to the Quan-adapted Elixhauser comorbidity index.28 HR is for 1-unit increase in morbidity score.
-
- Table 3
Effect of Continuity of Care and Morbidity Burden on Adjusted Hazard Ratios of Emergency Department Visits
Predictive Variables Subcohorta Primary Care, HR (95% CI)b (n = 8,706) Specialty Care, HR (95% CI)b (n = 6,738) Primary and Specialty Care, HR (95% CI)b (n = 5,713) Primary care continuity (COCI) 0.97 (0.96–0.98)c – 0.98 (0.96–1.00)c Specialty care continuity (COCI) – 0.98 (0.96–1.00)c 0.98 (0.95–1.00) Morbidity burdend 1.06 (1.04–1.08)c 1.05 (1.03–1.07)c 1.06 (1.03–1.08)c -
COCI = Continuity of Care Index27; HR = hazard ratio.
-
↵a Three or more visits of any type required for subcohort membership.
-
↵b Adjusted for age, sex, race/ethnicity, socioeconomic status, and prior year primary care, specialty care, and baseline emergency department visits. HR is for each 0.1-unit increase in COCI.
-
↵c Significant at P ≤.05.
-
↵d According to the Quan-adapted Elixhauser comorbidity index.28 HR is for 1-unit increase in morbidity score.
-
The Article in Brief
Effect of Continuity of Care on Hospital Utilization for Seniors With Multiple Medical Conditions in an Integrated Health Care System
Elizabeth A. Bayliss , and colleagues
Background Continuity of care refers to an ongoing health care relationship. Low continuity of care is associated with more inappropriate medication prescribing, higher cost of care, more avoidable hospitalizations, and greater use of emergency services. This study looks at whether interpersonal continuity (seeing the same clinician over time) is associated with rates of hospital admissions and emergency department use among seniors with multiple chronic medical conditions. The study takes place in an integrated system of health care delivery with high informational continuity (clinical information is available to all clinicians caring for a patient) through shared electronic records.
What This Study Found Greater primary care and specialty care continuity are each associated with lower inpatient admission and lower risk of emergency department visits. For patients with three or more primary care and three or more specialty care visits, specialty care continuity, but not primary care continuity, is associated with a decreased risk of hospital admissions; primary care continuity, but not specialty care continuity, is associated with a decreased risk of emergency department visits.
Implications
- Different subgroups of patients will benefit from continuity with primary and specialty care clinicians depending on their care needs.
- Interpersonal continuity may have a beneficial effect on utilization independent of the informational continuity provided by electronic medical records.
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- Continuity of care in general practice and secondary care: retrospective cohort study
- Improving personal continuity in general practice: a focus group study
- Health Care Utilization After a Visit to a Within-Group Family Physician vs a Walk-In Clinic Physician
- Optimising personal continuity for older patients in general practice: a cluster randomised stepped wedge pragmatic trial
- The Wall of Evidence for Continuity of Care: How Many More Bricks Do We Need?
- General practitioners ending their practice and impact on patients health, healthcare use and mortality: a protocol for national registry cohort studies in Norway, 2008 to 2021
- Optimising personal continuity: a survey of GPs and older patients views
- Optimising personal continuity: a survey of GPs and older patients views
- General practitioners ending their practice and impact on patients health, health care use and mortality. A protocol for national registry cohort studies in Norway, 2006 to 2021
- Towards a framework for patient-centred care coordination: a scoping review protocol
- Primary care physician involvement during hospitalisation: a qualitative analysis of perspectives from frequently hospitalised patients
- Analysis of multimorbidity networks associated with different factors in Northeast China: a cross-sectional analysis
- How does general practitioner discontinuity affect healthcare utilisation? An observational cohort study of 2.4 million Norwegians 2007-2017
- Retrospective cohort study to investigate the 10-year trajectories of disease patterns in patients with hypertension and/or diabetes mellitus on subsequent cardiovascular outcomes and health service utilisation: a study protocol
- Identifying patterns of health care utilisation among physical elder abuse victims using Medicare data and legally adjudicated cases: protocol for case-control study using data linkage and machine learning
- Association between continuity and access in primary care: a retrospective cohort study
- Physical Distancing With Social Connectedness
- Disparities in health outcomes among seniors without a family physician in the North West Local Health Integration Network: a retrospective cohort study
- Critical Care Nurses Reasons for Working or Not Working Overtime
- When Primary Care Providers (PCPs) Help Patients Choose Prostate Cancer Treatment
- Association between Continuity of Care and Health-Related Quality of Life
- Achieving Coordinated Care for Patients With Complex Cases of Cancer: A Multiteam System Approach
- Continuity of care in primary care and association with survival in older people: a 17-year prospective cohort study
- Impact of integrated health system changes, accelerated due to an earthquake, on emergency department attendances and acute admissions: a Bayesian change-point analysis
- In This Issue: Developing and Amplifying the Effectiveness of the Primary Care Workforce