


Abstract
Associations of multimorbidity and income with hospital admission were investigated in population samples from 3 widely differing health care systems: Scotland (n = 36,921), China (n = 162,464), and Hong Kong (n = 29,187). Multimorbidity increased odds of admissions in all 3 settings. In Scotland, poorer people were more likely to be admitted (adjusted odds ratio [aOR] = 1.62; 95% CI, 1.41–1.86 for the lowest income group vs the highest), whereas China showed the opposite (aOR = 0.58; 95% CI, 0.56–0.60). In Hong Kong, poorer people were more likely to be admitted to public hospitals (aOR = 1.68; 95% CI, 1.36–2.07), but less likely to be admitted to private ones (aOR = 0.18; 95% CI, 0.13–0.25). Strategies to improve equitable health care should consider the impact of socioeconomic deprivation on the use of health care resources, particularly among populations with prevalent multimorbidity.
- multimorbidity
- chronic disease
- hospital admission
- cross-country analysis
- population-based study
- socioeconomic factors
- health care system
INTRODUCTION
Multimorbidity, the coexistence of 2 or more chronic conditions within an individual, is increasingly common1,2 and leads to more hospital admissions, especially in patients having lower socioeconomic status.3 Most studies on multimorbidity have been conducted in developed countries in the West, however4; how admission rates are influenced by socioeconomic status under differently organized and funded health care systems in eastern or transitioning countries is unknown.
Scotland, a western country, has a well-established public health care system providing universal coverage. Work there has shown a clear link between low socioeconomic status, multimorbidity, and admission rates.3 China, the largest country in the world in transition, does not provide universal health coverage. Social medical insurance offers a limited benefits package, and most health care remains based on fee-for-service charges and patients’ private out-of-pocket payment.5 Hong Kong, however, has maintained a public health care sector, funded mainly by taxes and providing the majority of secondary care, while the sizeable private health care sector, funded on a fee-for-service basis underpinned by direct out-of-pocket expenditure, provides the majority of primary care. We thus aimed to examine the relationships of multimorbidity and income with hospital admission in representative samples from these 3 countries.
METHODS
We undertook a cross-sectional comparative study from large, representative population-based surveys using multistage stratified random sampling in Scotland,6 China,2 and Hong Kong.7 The study was approved by the Survey and Behavior Research Ethics Committee, The Chinese University of Hong Kong.
Data in Scotland came from 4 cycles of the Scottish Health Survey (SHeS) from 2008 to 2011, consisting of a representative sample (n = 36,921) of the population with response rates ranging from 67% to 81%.6 The study sample in China included 4.55% (n = 162,464) of the general resident population in 3 representative prefectures (with health care and population characteristics comparable to national average)2 in Guangdong province. The household replacement rate was 9.91%, and 14.46% of questionnaires were answered by householders on behalf of household members.2 Data in Hong Kong came from the 2011 Thematic Household Survey (THS), consisting of a representative sample of the land-based noninstitutionalized resident population (n = 29,187) with an estimated response rate of 75%.7
Surveys were conducted by academic institutions (in Scotland6 and China2) or a consultant company (in Hong Kong7). Information collected was largely based on self-report from open-ended questions on chronic conditions (clinically diagnosed or being treated) and admissions to hospitals at the secondary level or above in the prior 12 months. A total of 31 chronic conditions were commonly reported in all surveys, capturing International Classification of Diseases, 10th Edition (ICD-10) coding categories. We defined multimorbidity as having 2 or more chronic conditions from 14 categories (neoplasms, endocrine and metabolic, mental disorders, nervous system, eye complaints, ear complaints, circulatory system, respiratory system, digestive system, genitourinary system, skin tissue, musculoskeletal system, infectious diseases, and blood and related organs) and used equal weighting.8
We conducted binary logistic regression analysis with a backward stepwise algorithm to examine the impact of income on the associations between multimorbidity and hospital admission. Statistical analyses were performed using multistage sample design with sampling weights by SPSS Statistics 20.0 (IBM Corporation).
RESULTS
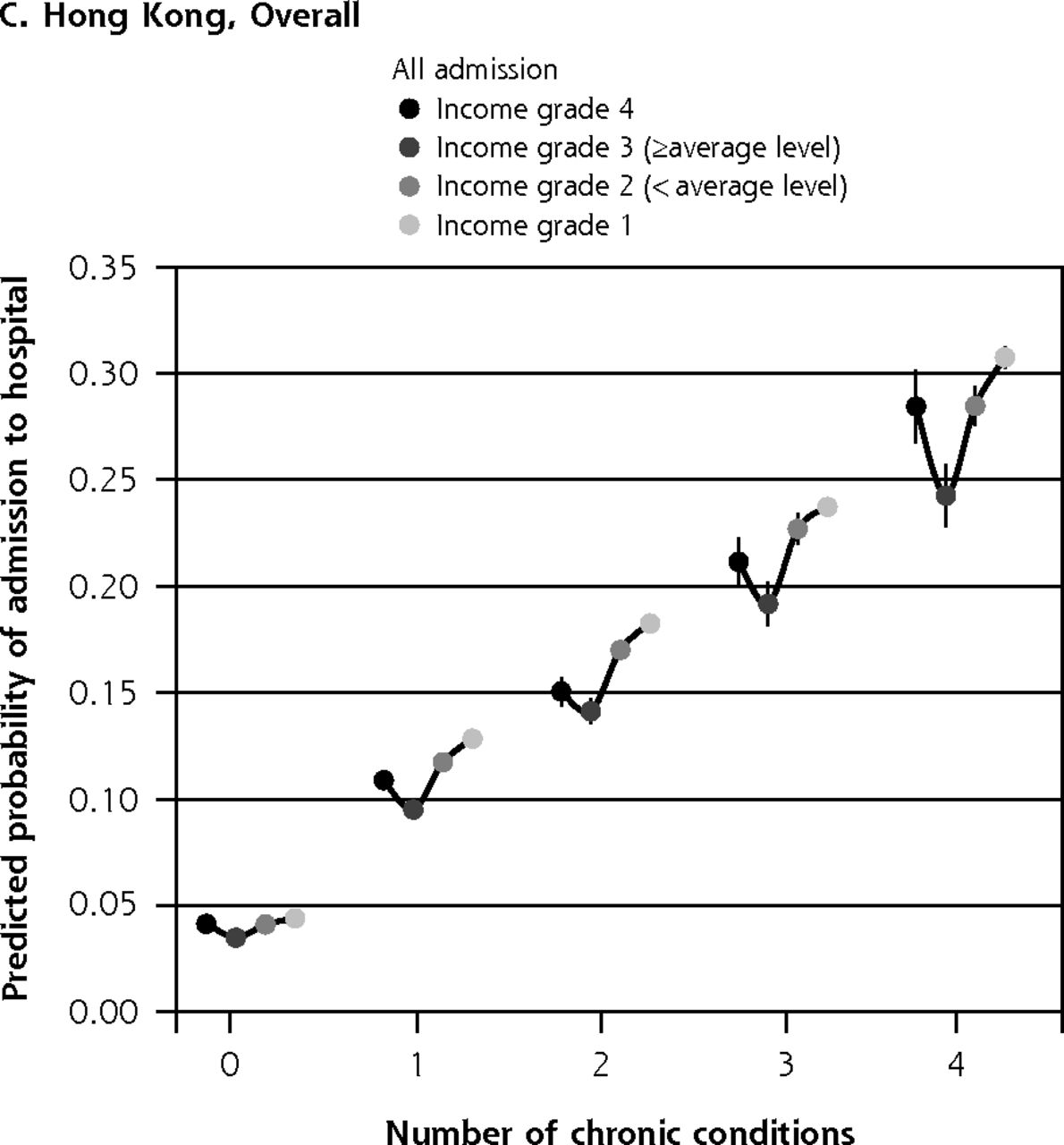
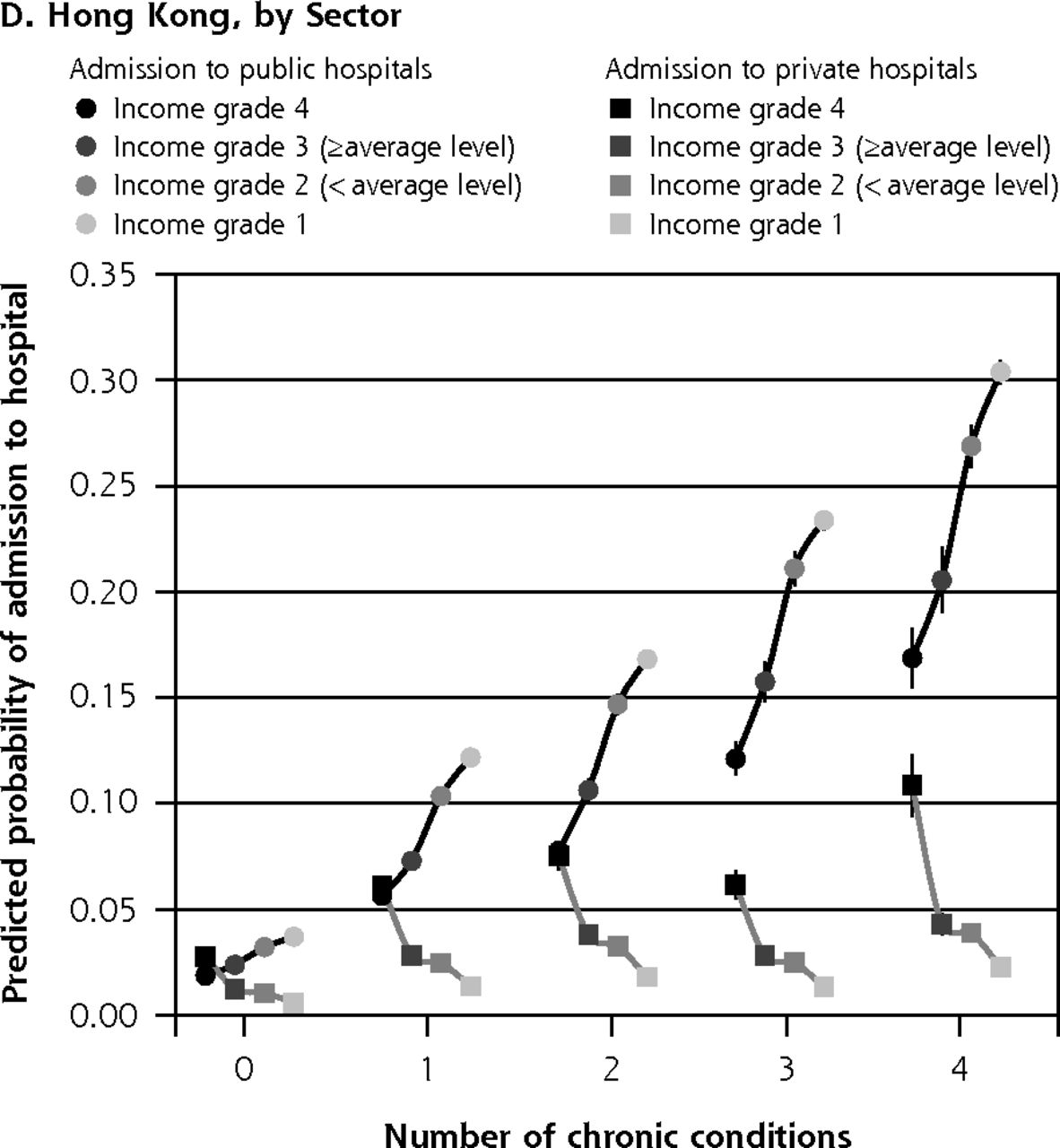
Independent factors positively associated with hospitalization across all 3 countries included female sex, older age, smoking, and multimorbidity (Table 1). The impact of income on hospitalization rate was greater among individuals with multimorbidity vs others, although patterns differed across settings. In Scotland, lower household income per head was associated with increased odds of hospitalization (adjusted odds ratio [aOR] = 1.62; 95% CI, 1.41–1.86 for the lowest income group vs the highest) (Figure 1A), whereas in China the opposite was found—those with lower incomes had reduced odds (aOR = 0.58; 95% CI, 0.56–0.60). Having social medical insurance conferred an increased likelihood of admissions in China among individuals with multimorbidity irrespective of income (Figure 1B). In Hong Kong, there was no clear overall pattern (P = .155) (Figure 1C); however, subanalysis by health care sector showed 2 distinct patterns, mirroring the 2 differing relationships found in Scotland and China. In Hong Kong, people in the lowest household income bracket had the highest odds of admission to hospitals in the public health care sector (aOR = 1.68; 95% CI, 1.36–2.07), but the lowest odds of admission to hospitals in the private health care sector (aOR = 0.18; 95% CI, 0.13–0.25) (Figure 1D).



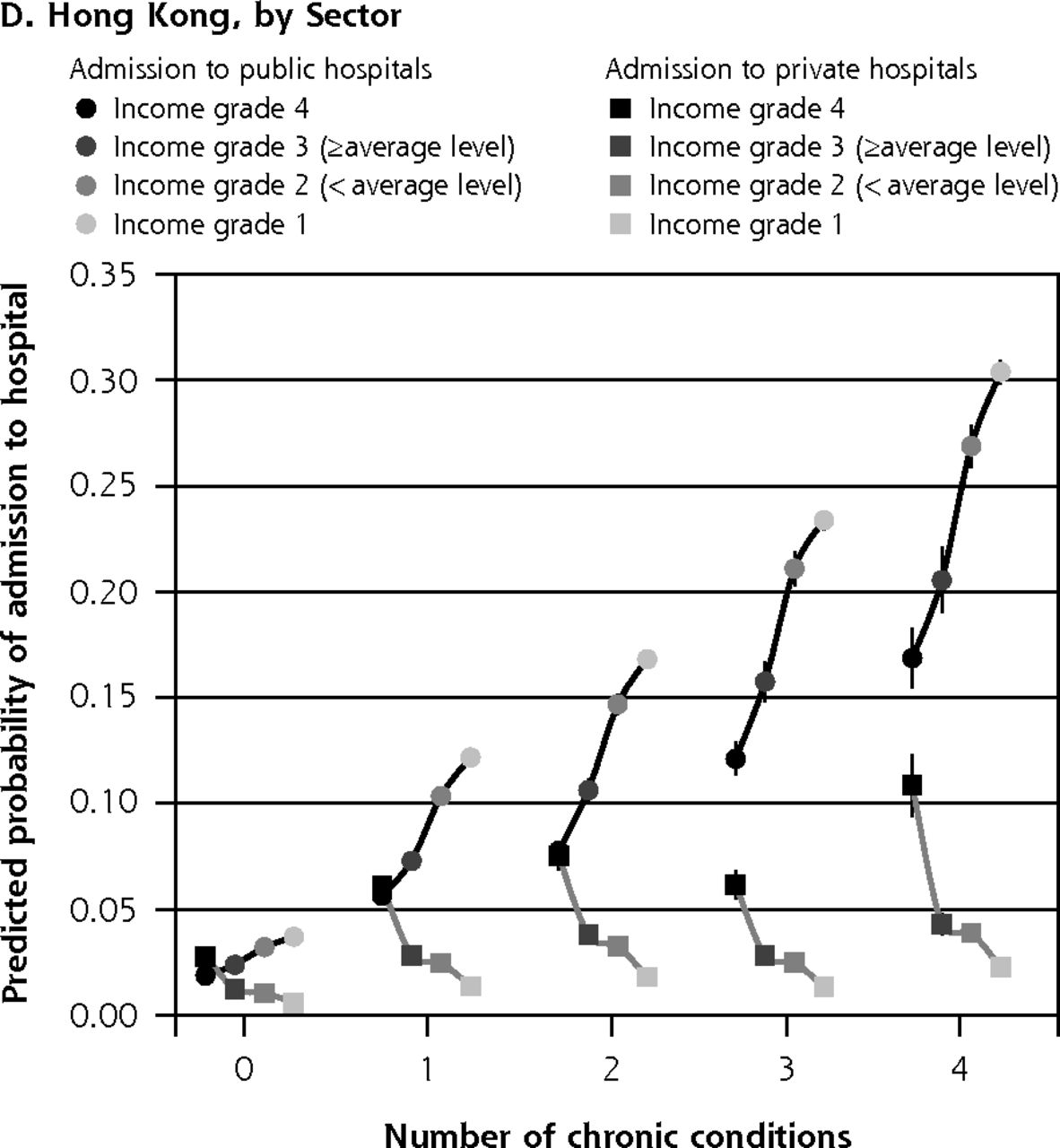
Predicted probability of hospital admission by income level among individuals aged ≥20 years in 3 differing health care systems.
Note: Error bars indicate 95% confidence interval.
Logistic Regression Models for Hospital Admissions in the Past 12 Months Among Patients Aged ≥20 Years
DISCUSSION
We have shown that multimorbidity increases the odds of hospital admissions in Scotland, China, and Hong Kong, in line with the international literature.3 The impact of income on this relationship varied across health care systems, however. In Scotland and in the public health care sector in Hong Kong, poorer individuals with multimorbidity were more likely to be admitted than richer counterparts with multimorbidity. This finding concurs with our previous research in Scotland using electronic health records.3 Within a national health care system with universal coverage, this association likely reflects unmet need due (at least in part) to the continuing problem of the “inverse care law.”9 In China, where universal coverage has not yet been established and primary care is still being developed,10 ability to pay is likely the main driver of admission, similar to the situation in the private health care sector in Hong Kong.
Inequitable access to care and the health literacy of the population could affect the disease diagnoses and possibly bias multimorbidity counts based on self-report data. In addition, the data did not allow determination of the reason for hospitalization. The study’s cross-sectional nature also means that causality can only be implied.
The challenges of health care disparities arising from multimorbidity are not limited to the 3 countries studied, but are of major relevance to many others currently aiming to make health care more equitable, including the United States. Strategies seeking to improve equitable health care will need to consider the impact of socioeconomic deprivation on the use of health care resources, particularly among populations with a high prevalence of multimorbidity.
Footnotes
-
* Authors contributed equally to this work.
-
Conflicts of interest: authors report none.
-
Funding support: We thank the Research Grants Council of Hong Kong and the Scottish Government, UK (Hong Kong-Scotland Partners in Post Doctoral Research, S-CUHK402/12), which supported H.H.X.W. with a postdoctoral research fellowship at the University of Glasgow, UK, to conduct this comparative study. The data collection in southern China was funded by the Department of Health, Guangdong province, P.R. China (C2009006/2009-2013); Department of Education, Guangdong province, P.R. China (BKZZ2011047/ 2010-2013); Medical Research Fund, Chinese Medical Association, P.R. China (2010-08-05); and the Community Health Research Fund, Community Health Association of China, P.R. China (2012-2-91). The Scottish School of Primary Care supported in part S.W.M.’s post and the development of the National Research Programme on Multimorbidity, which he leads.
-
Author contributions: S.Y.S.W., S.M.G., and S.W.M. conceived this international comparative study and provided overall guidance. H.H.X.W. and K.D.L. initially developed the morbidity list from chronic conditions reported in all 3 surveys, respectively, and J.J.W. further refined the list for cross-country comparison. J.J.W. led the data collection in China. K.D.L. did the initial extraction and management of the data in Scotland. Data in Hong Kong were obtained under a government-commissioned project using Thematic Household Survey on health-related issues, led by S.Y.S.W. All data analysis was done by H.H.X.W. and J.J.W., and all authors contributed to the literature search and interpretation of the data. H.H.X.W. and S.W.M. wrote the first draft, and all authors contributed to the feedback on study results and writing of the final report.
- Received for publication July 3, 2014.
- Revision received December 6, 2014.
- Accepted for publication December 12, 2014.
- © 2015 Annals of Family Medicine, Inc.
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Household and area determinants of emergency department attendance and hospitalisation in people with multimorbidity: a systematic review
- Impact of multimorbidity on healthcare costs and utilisation: a systematic review of the UK literature
- Characteristics of consistently high primary health care users in the DELPHI database: Retrospective study of electronic medical records
- Multimorbidity and healthcare utilization: A register-based study in Denmark
- Multimorbidity Trends in United States Adults, 1988-2014
- Prevalence of multimorbidity in the adult population attending primary care in Portugal: a cross-sectional study
- International primary care snapshots: Israel and China
- In This Issue: Developing and Amplifying the Effectiveness of the Primary Care Workforce