
Abstract
Genital tucking (tucking) is the practice of hiding or minimizing the appearance of one’s genitals and gonads. We aimed to better understand the prevalence of tucking and its potential effect on behavior and health. An online questionnaire was distributed to adults with a diagnosis of gender dysphoria or gender incongruence (n = 98). The risk of side effects increased with the length of tucking sessions (P = 0.046) with many patients avoiding medical care despite experiencing side effects. Health care providers should empathetically discuss tucking and its potential risks and benefits with transgender and gender diverse patients. Further research is needed to better quantify the potential risks involved with tucking and to assist in developing educational resources.
- gender affirming health care
- genital tucking
- gender incongruence
- gender dysphoria
- transgender
- gender diverse individuals
INTRODUCTION
Transgender and gender diverse individuals often experience significant harassment, abuse, and discrimination which can impact their self-beliefs and lead to negative health outcomes.1,2 As a result, they require care from enlightened health care providers and gender-affirming health systems.3
Transgender women are assigned male at birth and experience distress (dysphoria) regarding the discordance between their female gender identity and sex assigned at birth. Gender diverse is a term inclusive of nonbinary, eunuch, and intersex individuals who experience a gender identity that is not solely male or female.1 Transgender and gender diverse people may choose to hide or minimize the appearance of their genitals and gonads—a practice known as genital tucking (tucking). Tucking may be done with tape, underwear, or a special type of undergarment known as a gaff. This may or may not also involve pushing their gonads into the inguinal canal.4 Recent data suggest that tucking is correlated with reduced sperm quality.5,6 Prior survey data on this population suggests the risk of additional side effects but has not assessed individual perceptions regarding tucking or any associated effects on emotional health.7
The goal of this study was to improve our understanding of tucking, including prevalence, frequency, duration, attitudes regarding tucking, and self-perceived concern regarding potential and/or experienced side effects.
METHODS
We developed an anonymous survey, in English, using Qualtrics (Silver Lake Technology Management, LLC) software. The survey contained 27 questions in closed and open formats. Face validity was sought through review with 2 University of Virginia (UVA) committees: (1) the Gender Health Committee and (2) the Transgender Community Advisory Board.
We identified potential study participants by sorting for relevant International Classification of Diseases, 10th Revision (ICD-10) codes (eg, “gender dysphoria”) of established patients in the electronic medical record in 6 health system clinics. Exclusion criteria included individuals aged 17 years or younger and those assigned female at birth. Patients were invited to participate via an online web link through the MyChart patient portal. We provided a $25 Amazon gift card as an incentive to the first 100 participants via optional linked contact information to protect anonymity. The survey was administered from September to November 2022. Data analyses included descriptive statistics, χ2 test for variance in relation to the duration of tucking and reported side effects, fishers exact test in relation to age and tucking frequency, and qualitative analysis using thematic coding with 4 independent raters. Variability in denominators is due to participants skipping questions. This study was deemed exempt by the Institutional Review Board.
RESULTS
The survey was distributed to 300 individuals with 98 responses (33% response rate). Respondents’ ages ranged from 18 years to over 70 years. There was no identified association between age and either frequency or duration of tucking (P = 0.868).
Tucking was learned about from peers, experimentation, or Internet sources. Seventy-nine percent of respondents reported tucking, with 35% daily, 17% a couple of days per week, 13% a couple of days per month or every few months, and 14% a couple of days per year. Forty-three percent of respondents began tucking at the age of 18 years or younger. Fifty-one percent reported tucking from 8 to 13 hours per day.
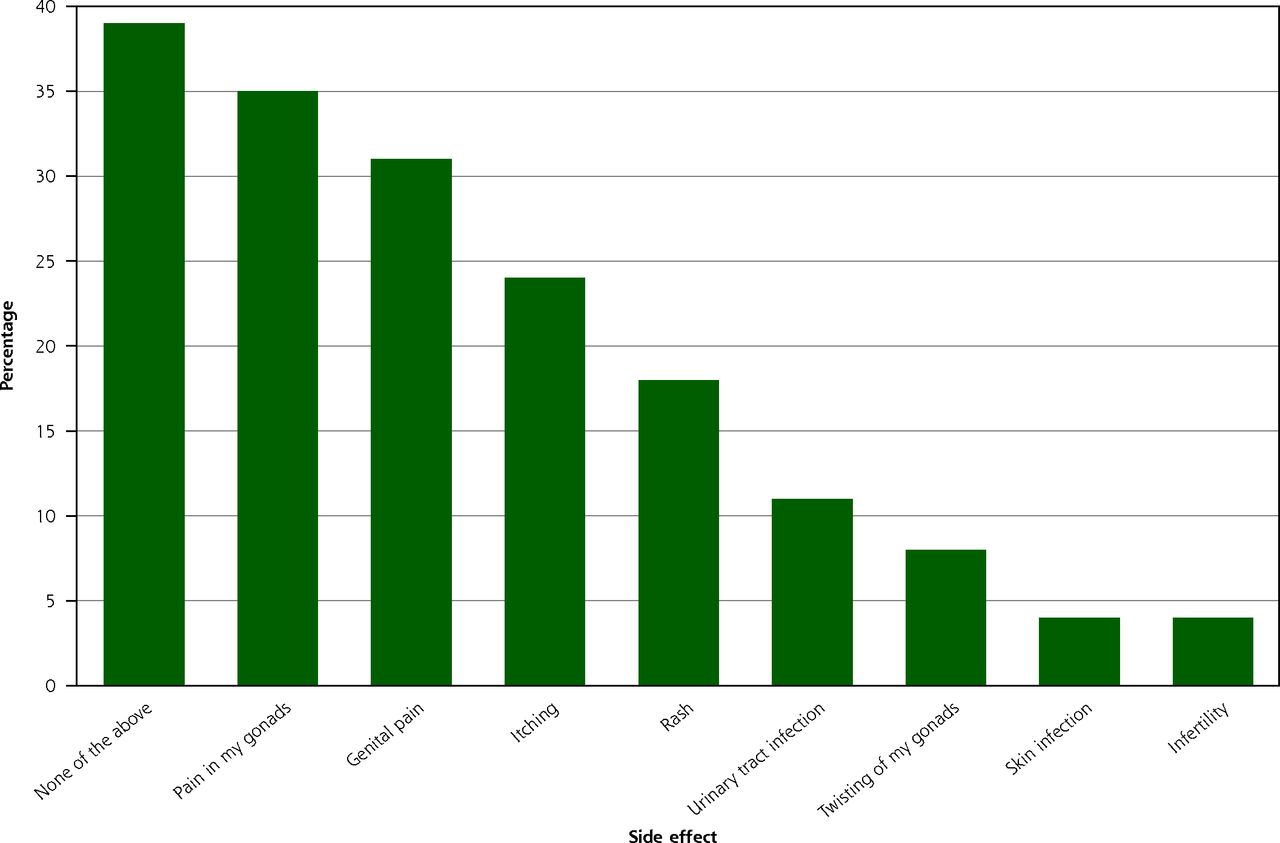
Of respondents who tucked, 52% reported taking breaks from tucking with breaks ranging from a couple of hours to months. Fifty-one respondents (65%) experienced at least 1 side effect from tucking (Figure 1), with gonad pain reported most frequently (32%). Seven respondents (10%) sought medical care for their side effects. Risk of side effects increased with cumulative daily duration of tucking χ2 (5, n = 75) = 11.27; P = 0.046.

Patient responses to question “Have you ever personally experienced any of the following symptoms that you attribute to tucking? (Please check all that apply).”
Note: n = 79.
While 70% of respondents felt they would be comfortable or very comfortable discussing tucking with their health care provider, only 23% reported having discussed tucking. A majority of participants felt that it would be helpful for clinicians to openly discuss the potential risks and benefits of tucking. Suggestions for clinicians included: asking permission, using inclusive and empathic language, explaining the reasoning behind broaching the topic, and being knowledgeable about methods and potential risks of tucking. Representative responses for each question are identified in Table 1.
Representative Responses to Open-Ended Survey Questions
DISCUSSION
Genital tucking is a common method transgender and gender diverse people use to alleviate dysphoria and feel safer. It is important to note, however, that tucking frequency and practices are individualized; some participants choose not to tuck or only tuck infrequently. The reported side effects in our population were similar to prior published survey data with predominantly mild side effects such as pain, itching, and rash.7 Major side effects were rarely reported.
Despite many participants experiencing side effects and some viewing any associated pain as a “necessary evil,” few had ever discussed tucking with their clinician(s). Participants cited prior traumatic medical interactions, dysphoria regarding discussing their anatomy, and concern for a potentially invasive exam as reasons for reticence. This is exacerbated by clinicians often feeling uncomfortable about their lack of knowledge of the topic. Despite this, the majority of participants encouraged clinicians to discuss tucking with their patients in an empathetic manner. Clinicians are encouraged to ask patients if they would like to discuss risks, benefits, and safe methods of tucking and ask about preferred anatomy terminology, as the words penis and testicles may be offensive to this population. This discussion may be of particular benefit to those who tuck for 8 or more hours per day as these individuals appear to be more likely to experience side effects.
Clinicians should assess motivations and ambivalence regarding tucking as well as discuss potential risks including impaired fertility, pain, itching, rash, and less likely but potentially more severe risks such as testicular torsion and infection. Impaired fertility appears to be reversible though there is insufficient evidence about reversibility of other side-effects.5 Respondents called for more health care–provided educational materials such as printouts or media to help guide safe practice; however, the paucity of published data makes creating evidence-based materials challenging.
Study limitations include limited sample size and generalizability. Respondents were recruited from 1 health care system and its catchment area. This study is at risk for non-response bias which may favor responses toward those who tuck more frequently or who experience more frequent or severe side effects. No demographic data other than age were collected to enhance anonymity. Further research is needed to identify the safety profile of tucking in order to help guide effective, evidence-based education for patients and clinicians. Additionally, future research is recommended to assess the effect of hormone treatment and gender-affirming surgery on individuals who tuck.
Acknowledgments
The authors would like to thank Dr Cornelius Normeshie for statistical support and Dr Fern Hauck for methodological support and review of the manuscript.
Footnotes
Conflicts of interest: authors report none.
Funding support: The University of Virginia Department of Family Medicine pilot research grant.
- Received for publication April 11, 2023.
- Revision received November 8, 2023.
- Accepted for publication November 20, 2023.
- © 2024 Annals of Family Medicine, Inc.
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.