
Abstract
PURPOSE To analyze spatiotemporal trends in hospitalizations for cardiovascular diseases (CVD) sensitive to primary health care (PHC) among individuals aged 50-69 years in Paraná State, Brazil, from 2014 to 2019 and investigate correlations between PHC services and the Social Development Index.
METHODS We conducted a cross-sectional ecological study using publicly available secondary data to analyze the municipal incidence of hospitalizations for CVD sensitive to PHC and to estimate the risk of hospitalization for this group of diseases and associated factors using hierarchical Bayesian spatiotemporal modeling with Markov chain Monte Carlo simulation.
RESULTS There was a 5% decrease in the average rate of hospitalizations for PHC-sensitive CVD from 2014 to 2019. Regarding standardized hospitalization rate (SHR) according to population size, we found that no large municipality had an SHR >2. Likewise, a minority of these municipalities had SHR values of 1-2 (33%). However, many small and medium-sized municipalities had SHR values >2 (47% and 48%, respectively). A greater Social Development Index value served as a protective factor against hospitalizations, with a relative risk of 0.957 (95% credible interval, 0.929-0.984).
CONCLUSIONS The annual risk of hospitalization decreased over time; however, small municipalities had the greatest rates of hospitalization, indicating an increase in health inequity. The inverse association between social development and hospitalizations for CVD sensitive to PHC raises questions about intersectionality in health care.
- cardiovascular disease
- primary health care
- hospitalizations
- health care disparities
- spatiotemporal analysis
- Social Development Index
INTRODUCTION
Cardiovascular disease (CVD) leads the rankings of morbidity and mortality worldwide. An estimated 17.9 million people died of CVD in 2019, with more than three-quarters of these deaths occurring in low- and middle-income countries and one-third occurring in individuals <70 years of age.1 In Brazil in the same year, CVD was the absolute leading cause of mortality, accounting for 364,132 deaths.2 In addition, CVD was the third most frequent cause of hospital morbidity, responsible for 1,179,365 hospitalizations.3
Despite the high incidence of CVD morbidity and mortality, approximately 80% of cases can be timely and effectively avoided by primary health care (PHC); this is referred to as “hospitalizations for primary care–sensitive conditions” or “potentially avoidable hospitalizations.”4,5 Primary health care is an opportune place to offer care related to good health habits, such as healthy eating, regular physical activity, smoking cessation, and limiting alcohol consumption,6,7 in addition to being a service for the diagnosis, management, and treatment of health conditions.8,9
In Brazil, PHC works via the Family Health Strategy, a decentralized service located close to people’s homes that, with a multidisciplinary team, provides health care for a population in a defined territory.10 To evaluate this health strategy, Brazil created the List of Sensitive Conditions for Primary Care in 2008, based on international references that measure hospital morbidities potentially avoidable by PHC.8 Studies agree that PHC decreases and prevents hospitalizations.9,11,12 However, there is a lack of research assessing different aspects of the PHC service to investigate the occurrence of hospitalizations for CVD sensitive to PHC in Paraná State, south of Brazil.
Hospitalizations for CVD sensitive to PHC analyzed from the perspective of spatial and temporal risks might be useful to identify areas of risk, temporal trends, and health inequalities. We aimed to assess spatiotemporal trends and risks for hospitalization for CVD sensitive to PHC and examine correlations with PHC services and the Social Development Index (SDI) of Paraná municipalities.
METHODS
Study Design and Location
We performed an ecological study using hierarchical Bayesian spatiotemporal modeling with Markov chain Monte Carlo (MCMC) simulations to analyze data on hospitalizations for CVD sensitive to PHC in Paraná State, Brazil, from 2014 to 2019. To analyze different aspects of a common health phenomenon, which is often studied using frequentist analysis, we decided to use a methodology that allows the visualization of the spatiotemporal risk of hospitalizations, following the recommendations from the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines.13
Paraná comprises a total area of 199,298.982 km2, located between latitudes 22°30′58″S to 26°43′00″S and longitudes 48°05′37″W to 54°37′08″W. The state had an estimated population of 11,597,484 inhabitants in 2021 according to the latest census14 and a Human Development Index of 0.792 in 2017 according to the most recent data available from the Brazilian Institute of Geography and Statistics,15 having the fifth greatest Human Development Index among the 26 Brazilian states, a value similar to those of developed countries. Paraná comprises 399 municipalities divided into 10 administrative regions and presents 323 (81%) municipalities with <25,000 inhabitants.16
Data Sources and Variables
We used public data from the Hospitalization Information System of the Department of Informatics of the Brazilian Ministry of Health (SIH-DATASUS; https://datasus.saude.gov.br/informacoes-de-saude-tabnet) to construct a database of hospitalizations for PHC-sensitive CVD among people aged 50-69 years in Paraná State. Cardiovascular disease is less common in individuals <50 years of age; therefore, if we include them, hospitalization rates per adjusted population will be low. Very elderly people, however, are highly likely to develop CVD that is not sensitive to PHC,17 making it difficult to distinguish between them. Thus, we considered the World Health Organization definition of premature mortality, which is <70 years of age, because medical advances in the prevention and treatment of chronic diseases are potentially capable of preventing mortality before this age.18
The causes of hospitalization, which comprised the outcome variable, were based on the International Classification of Diseases, 10th Revision (ICD-10), which in turn is referenced in the Brazilian List of Primary Care-Sensitive Conditions.8 We obtained the data used in the present research using the microdatasus package19 of RStudio version 4.1.0 (the R Foundation), accessed via the SIH-DATASUS. We calculated hospitalization rates as described in Table 1.
Data Sources, Variables, Disease Codes, and Calculation Methods Used for Data Synthesis
Predictor variables comprised 14 independent variables related to PHC. These were initially selected from free, publicly available databases. Variables were assigned to 5 categories: number of higher education health professionals, number of individual appointments related to CVD, population coverage by PHC services, group activities related to health education, and municipal SDI (Table 1). The hospitalization rate was calculated by dividing the number of hospitalizations into people aged 50-69 years by the estimated population of the same age group, multiplied by 10,000. Because collinearity was not identified (variance inflation factor was <5),20 variables were added within each category and converted to values per 1,000 people, with the exception of SDI.
Exploratory Analysis
We performed statistical analyses using a hierarchical Bayesian spatiotemporal model and conducted MCMC simulations, allowing us to estimate the posterior distribution of the parameters involved in the model. These analyses were carried out with the CARBayesST package of RStudio, version 4.1.0, following a tutorial on spatiotemporal disease risk modeling in R.21
Expected number of hospitalizations was calculated by indirect standardization, in which the age-adjusted population for each municipality was divided per 10,000 and multiplied by the average hospitalization rate of the state. Mathematically, this method estimated the expected number of individuals requiring hospital care as the state average of hospitalizations during the period 2014-2019, applied to each municipality for each year.22 We then calculated the standardized hospitalization ratio (SHR), dividing the number of hospitalizations observed by the number of hospitalizations expected in the same period. Standardized hospitalization ratio values >1 indicate that the number of hospitalizations was above the expected; for example, an SHR of 1.2 indicates that hospitalizations were 20% greater than the expected rate.21 We plotted the results on the map of Paraná State using Quantum Geographic Information System (QGIS) software version 3.12 (QGIS Development Team).
We examined the number of hospitalizations and independently configured the regression parameters to assess whether the selected independent variables exhibited any form of spatial or temporal autocorrelation at the hospitalization data.22 Subsequently, we used the log-linear Poisson model to depict the relations between the covariates and hospitalization rates, followed by the application of the maximum likelihood estimation technique to determine the coefficients of this model that offered the best fit to the observed data. This approach enabled us to identify potential significant patterns associated with geographic location and temporal variation in hospitalizations. Because hospitalization for PHC-sensitive CVD is a multifactorial event, it is difficult to establish the independence of parameters and samples; therefore, we used Bayesian analysis and MCMC simulation.23,24
The hierarchical Bayesian spatiotemporal model uses Bayes’ theorem to generate a new probability of spatiotemporal distribution, termed posterior distribution, and composes our updated estimates regarding the new parameters by combining our prior information with the new data.23 We adjusted this model with MCMC simulations to produce sequential samples (Markov chain), in which the next sample is obtained based on the previous one, following probabilistic rules, converging to stationary distribution, also termed posterior distribution.21
For this, 5 Markov chains were run for 2,200,000 generations, with an initial burn-in period of 200,000 iterations for variables that did not show convergence. The remaining 2,000,000 iterations were thinned by 1,000, which allowed us to almost completely eliminate auto-correlations; thus, 10,000 generations remained for analysis, 2,000 per chain.22 Assessment of the adequacy of the inference model assumes that samples must converge without trends in means or variances. Therefore, Geweke’s diagnostics were applied to measure convergence. Ideally, the results should range from −2 to 2.25 We obtained values of −1.3 to 2, indicating good convergence and model adequacy.
Model Inference
Our analysis produced 2 key outcomes related to the spatial pattern of disease risk: posterior median risk surface and posterior exceedance probabilities (PEP). To derive these, we constructed a matrix of MCMC samples for the regression parameters of all chains, considering a 95% credible interval (CI). The posterior median risk surface is an important tool to understand the spatial distribution of risk, given that it is the estimated value of risk of disease at different geographic regions based on our data and Bayesian analysis and MCMC simulation.25 Posterior exceedance probability is a way to quantify uncertainty regarding which regions exhibit significantly greater risk than others, indicating the chance of a specific place having a disease risk that exceeds a critical value, helping us to identify areas of heightened concern or to target intervention resources when the risk is pronounced.21
In addition, we examined temporal trends in relative risk by calculating the average risk of hospitalization for each year across the 399 municipalities. Finally, we quantified health inequalities year by year based on the variation in risk of hospitalization, considering predictive variables addressed in this study, between municipalities within the State of Paraná. To achieve this, we computed the interquartile range (third quartile minus first quartile) for hospitalization risk for each year.21,22
Ethical Aspects
In accordance with Resolution No. 510/2016 of the Brazilian National Health Council and considering that the data used in this study were obtained from secondary sources available to the general population, the Committee for Ethics in Research Involving Human Beings of the State University of Maringá (COPEP/UEM) waived the need for registration and ethical evaluation (Approval Letter No. 2/2021 COPEP).
RESULTS
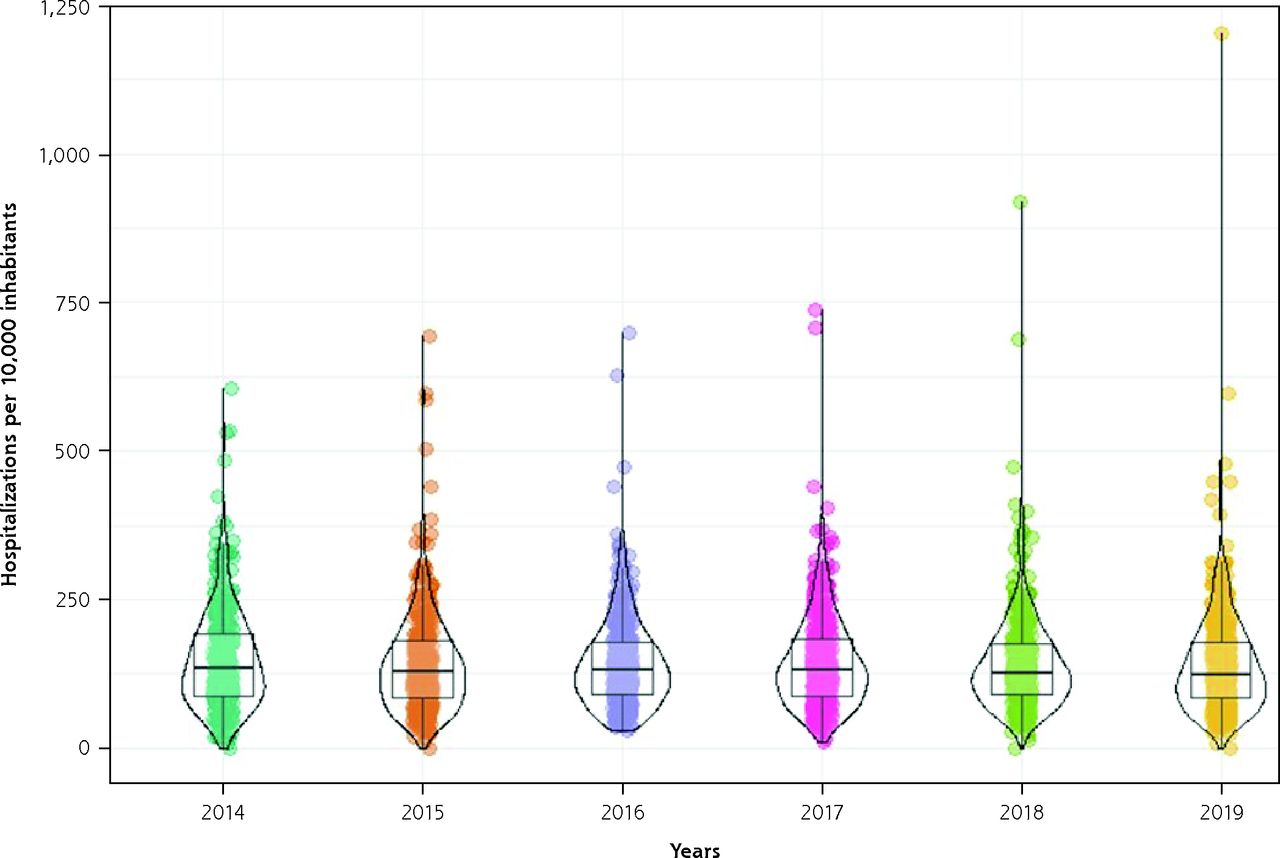
During the study period, there were 193,174 hospitalizations for CVD sensitive to PHC. The annual number of hospitalizations increased over time, from 30,738 in 2014 to 34,739 in 2019. However, the average number of hospitalizations per 10,000 people decreased from 149 ± 85.10 in 2014 to 142 ± 95.06 in 2019, reaching the lowest value in 2015 (141 ± 84.88). Some municipalities reported high hospitalization rates (outliers), particularly in 2018 and 2019. Figure 1 shows the temporal trend in hospitalizations.

Temporal trends in hospitalizations for cardiovascular diseases preventable by primary health care, per 10,000 inhabitants in Paraná State, Brazil, 2014-2019.
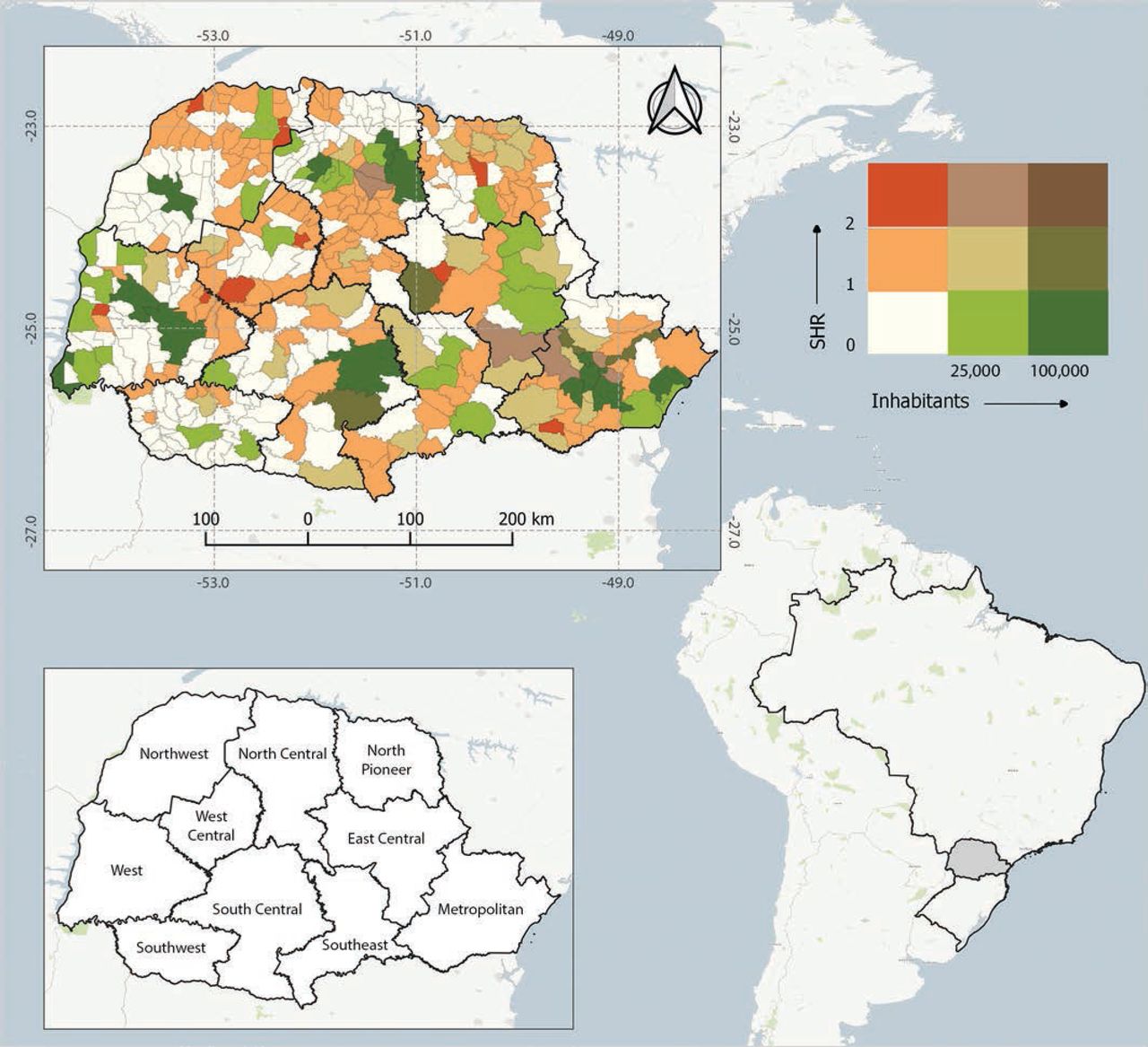
Comparison of observed vs expected hospitalization rates revealed that no large municipality had an SHR >2. Likewise, a minority of these municipalities had SHR values of 1-2 (33%). Many small and medium-sized municipalities, however, had SHR values >2 (47% and 48%, respectively) as shown in Figure 2.

Bivariate map showing relation between standardized hospitalization ratio and population size in Paraná State, Brazil, 2014-2019.
SHR = standardized hospitalization ratio.
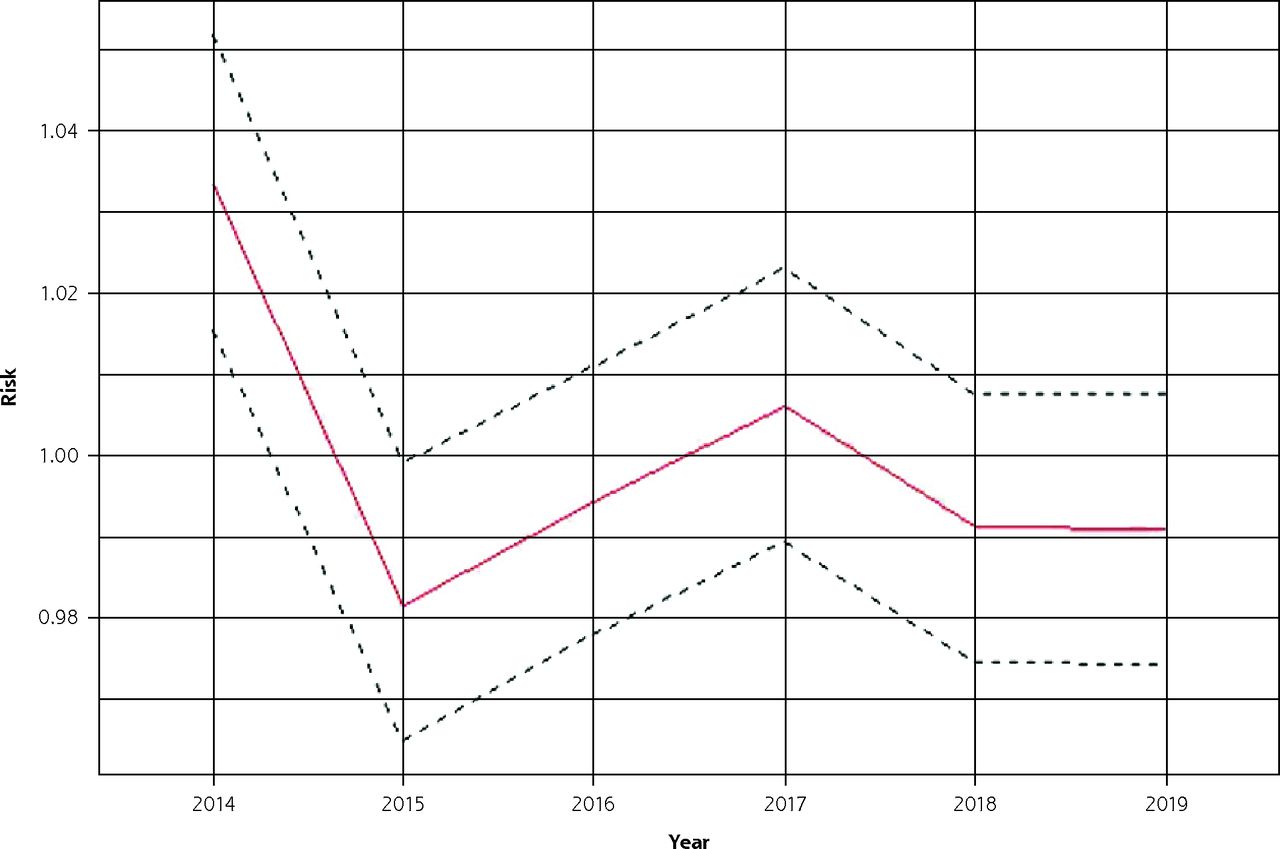
The annual risk of hospitalization was <1 for the majority of the study period. The risk peaked in 2014 (risk = 1.03) and achieved the lowest value in 2015 (risk = 0.98) (Figure 3). The only variable associated with prevention of hospitalization was SDI value (relative risk = 0.957; 95% CI, 0.929-0.984), demonstrating that if SDI increases 4.3%, hospitalizations for CVD sensitive to PHC decrease 4.3%. Health care professionals, attendance, coverage, and group activity were not statistically significant with respect to prevention of hospitalization.

Posterior mean and 95% credible interval for temporal risk of hospitalization for cardiovascular diseases preventable by primary health care in Paraná State, Brazil, 2014-2019.
Annual risk of hospitalization and PEP values are shown in Figure 4, which for the sake of brevity and to facilitate comparison between the first and last years of the study only show maps for 2014 and 2019. These maps showed spatial homogeneity, with some random municipalities presenting a risk >1 for hospitalization for PHC sensitive to CVD. We also observed a decrease in risk and PEP over time. In addition, not all municipalities with high PEP values had necessarily high risk, even though all municipalities with high risk had high PEP values.

Risk estimates (posterior means) and posterior exceedance probability of hospitalization for cardiovascular diseases preventable by primary health care in Paraná State, Brazil, 2014-2019.
PEP = posterior exceedance probabilities.
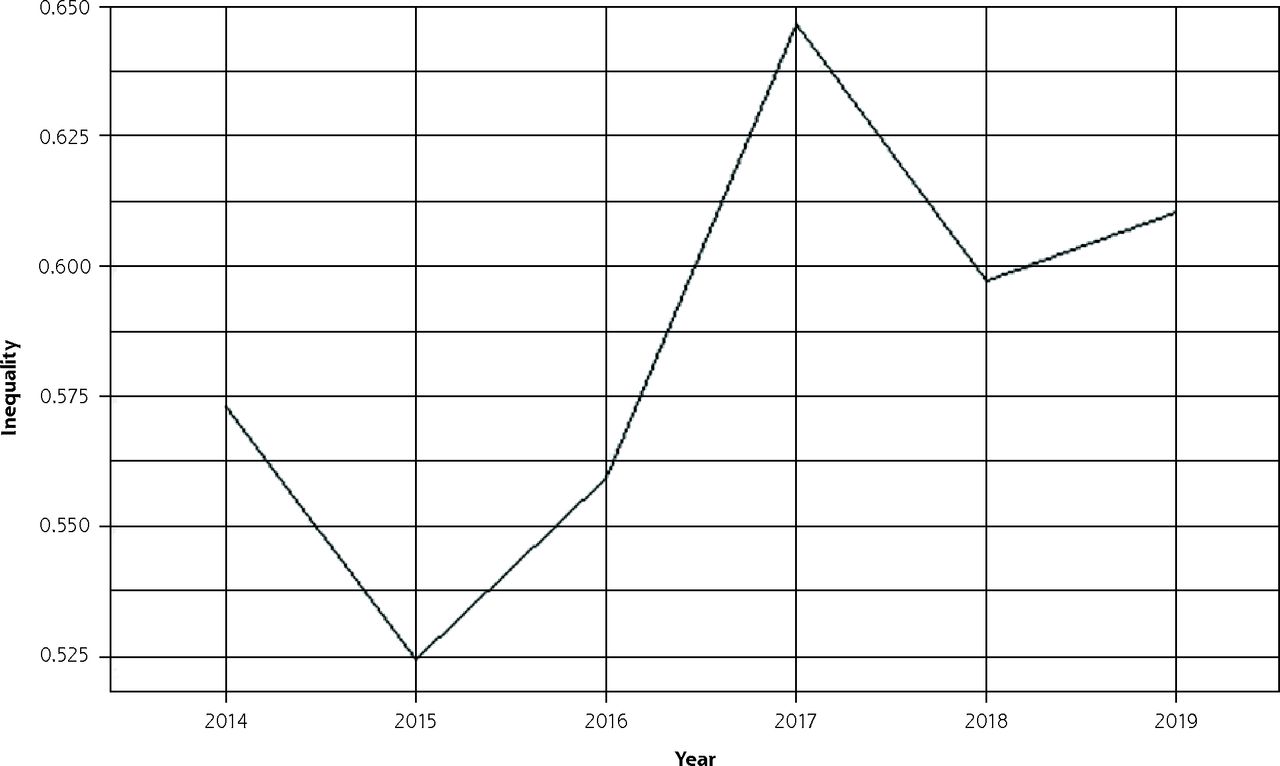
Although the annual risk of hospitalization decreased over the years, inequality in the risk of this event increased, as shown in Figure 5. Municipalities with marked discrepancies in the risk of hospitalization appeared from 2017 onward, which was the year with the greatest peak in inequality; by contrast, 2015 had the lowest risk inequality (0.525).

Estimates of temporal trends in inequality in the risk of hospitalization for cardiovascular diseases preventable by primary health care in Paraná State, Brazil, 2014-2019.
DISCUSSION
Understanding the spatial distribution of hospitalizations for PHC-sensitive CVD is important for developing more assertive public health policies. Many studies have sought to understand the occurrence of these preventable hospitalizations.12,17,26 The present study is the first to our knowledge to show a greater risk in small municipalities, the influence of social development as a preventive factor, and the growing disparity in the occurrence of hospitalizations between municipalities in Paraná.
The present study showed that living in small and medium-sized municipalities is a risk factor for hospitalization for CVD sensitive to PHC in the state of Paraná. These municipalities have predominantly rural characteristics that might result in decreased spatial access to health services, owing to greater geographic distance.27,28 Social dimensions, such as limited public transport in these regions, are also involved in access.29 In addition, the management of physical and human resources is less efficient in small municipalities, given that there are difficulties in maintaining qualified health professionals; health professionals tend to concentrate in urban areas where there are more job opportunities and better health infrastructure.30,31
Considering the social potential of access to health services, we reach another important finding of this study, which is greater social development as a protective factor against hospitalizations. Researchers agree that social marginalization, the result of several factors including low education and limited income, makes it difficult for the population to access healthy food, safe environments for physical exercise, and health services.28,32,33 The lack of health education implies a lower awareness of the importance of disease prevention, health care, and the adoption of healthy lifestyle practices.34 Thus, preventing hospitalizations for CVD is the result of several strategies that depend on the intersectionality of public policies to improve the population’s living conditions.10,35
Decreases in the risk and PEP of hospitalizations over time might be due to investments in public health and scientific advances in the treatment and prevention of diseases.36,37 However, we cannot exclude that many hospitalizations could have been avoided, given the high capillarity of PHC in Paraná, covering approximately 70% of the population.38 The lowest risk was observed in 2015. Not coincidentally, PHC population coverage peaked in 2015.38 In agreement with others, we infer that the greater the PHC coverage, the better the health outcomes of the population, and consequently, the fewer the number of hospitalizations due to exacerbation of chronic conditions.26,39
The spatial distribution of risk and PEP showed that not all municipalities with high PEP necessarily presented high risk. All municipalities at high risk, however, had high PEP. This might be due to the fact that some municipalities have characteristics, such as low PHC coverage and low SDI, that might increase the risk of developing high rates of hospitalization.32,39 It is also important to consider that the broad distribution of municipalities with high risk and PEP might be a reflection of the homogeneity of unhealthy lifestyle habits in the general population and the broad distribution of small municipalities throughout the state.10
Despite the aforementioned decrease in risk of hospitalization, there was an increase in risk disparities between municipalities in Paraná. This means that some cities had an extremely greater risk of hospitalization than others, and this difference has been increasing over time. This again shows that some municipalities are more advanced in providing health services for the population, to the detriment of others.40
There are some limitations that need to be considered, given that this research was conducted with secondary data and was dependent on the veracity of the primary records. Nevertheless, the quality of secondary data from the Brazilian Ministry of Health has improved over time, being the best available resource for acquiring public health data. Complementary studies involving individuals might help to better understand the specific clinical and physical patterns, and consequently the trends of CVD, in Brazil and other low- and middle-income countries.
CONCLUSION
Despite a decrease in the rates of preventable hospitalization, its occurrence is still very high in Paraná State, particularly in small and medium-sized municipalities. The inverse association of hospitalizations with social development raises questions regarding the importance of macrosocial investments in actions to prevent PHC-sensitive CVD hospitalizations. We strongly advocate that further research should be conducted on the individual determinants of potentially preventable hospitalizations.
Acknowledgments
We would like to thank the Group of Digital Technologies and Geoprocessing in Health (Grupo de Tecnologias Digitais e Geoprocessamento em Saúde [GETS/UEM]) for providing support with geospatial analysis.
Footnotes
Conflicts of interest: authors report none.
Funding support: This study was financed by the Coordenação de Aperfeiçoamento de Pessoal de Nível Superior - Brazil (CAPES), Finance Code 001.
- Received for publication April 4, 2023.
- Revision received October 1, 2023.
- Accepted for publication November 29, 2023.
- © 2024 Annals of Family Medicine, Inc.
References
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.