
Abstract
PURPOSE An adequate supply of family physicians who deliver comprehensive care is critical for addressing evolving population health needs, fostering health equity, and ensuring a cost-effective health system. Little is known about current trends of family physicians choosing focused practice and concurrent changes in comprehensive family physician numbers relative to population growth.
METHODS We conducted a repeated cross-sectional population-based study using administrative data to understand sex-stratified trends in focused practice from 1993/1994 through 2021/2022 in Ontario, Canada, accounting for population growth. For each fiscal year, we identified all active family physicians and classified them by practice type, leveraging a previously published algorithm on comprehensiveness.
RESULTS The proportion of family physicians in focused practice increased from 7.7% (856/11,103) in 1993/1994 to 19.2% (3,351/17,413) in 2021/2022. The 3 most prevalent focused practice types at the end of the study period were emergency (37.0%), hospitalist (26.5%), and addiction (8.3%) medicine. A greater proportion of focused practice physicians were male (60.1%) vs female (39.9%) in 2021/2022. Over the study period, the number of family physicians increased from 104 to 118 per 100,000; however, the number of comprehensive family physicians decreased from 71 to 64 per 100,000. Of the additional 6,310 family physicians who entered the workforce, 39.5% (2,495/6,310) were in focused practice.
CONCLUSIONS Over the study period, there was a decrease in the percentage of comprehensive family physicians and a substantial increase in family physicians pursuing focused practice, particularly in emergency and hospitalist medicine. Research and policy work is needed to understand and address the complex factors driving these trends.
INTRODUCTION
Countries around the world are struggling to ensure population-wide access to primary care.1,2 In Canada, more than 1 in 5 adults report not having a regular primary care clinician,3 while approximately 15% of those with access may lose their clinician to retirement by 2025.4,5 Concurrently, population health needs are growing with an aging population, medical complexity is rising across all ages, and socioeconomic inequalities are widening.6,7 About 95% of people in Canada report that their primary care clinician is a family physician.3 Thus, ensuring an adequate supply of family physicians who deliver comprehensive care is crucial for effectively addressing evolving population health needs, while fostering health equity and ensuring a cost-effective health system.8-10
Family physician training is broad and provides physicians with a range of potential career choices—from outpatient practices that specialize in palliative care or addiction medicine to hospital-based practices that include inpatient care, emergency medicine, or anesthesia. Not all qualified family physicians choose to practice longitudinal, comprehensive care where they support the full range of patient needs across the lifespan. A few studies from the United States and Canada, primarily conducted before the COVID-19 pandemic, have reported fewer family physicians providing comprehensive care and greater numbers pursuing focused areas of practice such as emergency or sports medicine.11-17 The pandemic may have accentuated this trend.18 Little is known, however, about current trends in family physicians choosing focused practice, how these trends compare with population growth, what the most prevalent types of focused practice are, and how these choices differ by physician sex.
We used health administrative data to understand trends in focused practice in Ontario, Canada from 1993 through 2021, stratifying for physician sex and years in practice, and evaluating concurrent changes in the number of comprehensive family physicians per capita. Understanding these trends is critical for health workforce planning and developing a strategy to ensure primary care meets population needs.
METHODS
Context and Setting
Ontario is Canada’s largest province with a population of approximately 15 million in 2021. Family physician visits are fully insured for all permanent residents through the provincial health insurance plan. Licensed family physicians can open a practice anywhere in the province, choose what services they provide, and bill the government directly through the provincial health insurance plan. Approximately 85% of family physicians practicing longitudinal, comprehensive care are part of a Patient Enrolment Model that includes formal patient enrollment, payment via blended capitation or fee-for-service, and accountability for delivering afterhours services.4
Study Design and Population
We conducted a repeated cross-sectional population-based study in Ontario, Canada spanning fiscal years 1993/1994 through 2021/2022 (abbreviated as 1993-2021 here onwards). The study cohort was composed of general practitioners and family physicians who were acquired independently for each study year using methods aligned with the existing literature.14 Both general practitioners and family physicians provide primary care. General practitioners are not certified by the College of Family Physicians of Canada and new designations were phased out in the early 1990s in Ontario. We leveraged multiple health administrative data sets, which were linked using unique encoded identifiers and analyzed at ICES (formerly known as the Institute for Clinical Evaluative Sciences), an entity authorized to collect and use health care and demographic data for health system evaluation and improvement. The use of these data for the purposes of this study was authorized under section 45 of Ontario’s Personal Health Information Protection Act, and did not require review by a research ethics board.
Categorizing Family Physicians by Type of Work
We began by assessing comprehensiveness of practice based on the following 3 previously published criteria: (1) physician worked a minimum of 44 days during the year; (2) more than 50% of billings were for core primary care services; and (3) the threshold for number of primary care activity areas necessary for a physician to be considered as providing comprehensive care was met.14 Physicians who did not meet these criteria for comprehensiveness were categorized as follows: (1) focused practice (eg, hospital care, emergency medicine); (2) worked less than 44 days per year (eg, physician on leave); (3) other—did not meet criteria for comprehensive or focused practice but billed the provincial health insurance plan and worked a minimum of 44 days per year (eg, rural physician splitting time between hospital, long-term care, office); (4) had no public billings (ie, physicians paid exclusively through salary [eg, working at a Community Health Centre], physicians working exclusively in the private system [eg, Workplace Safety and Insurance Board], retired physicians with an active license but not working clinically, and physicians exclusively doing non-clinical work [eg, working for the government, research]).
The College of Family Physicians of Canada conceptualizes a focused practice family physician as having a major part- or full-time commitment to 1 or more specific clinical areas in their practice.19 We operationalized this using 3 distinct approaches (Supplemental Appendix 1): (1) focused practice assessment billing codes, which enabled family physicians to be designated to 1 of 7 areas of focused practice starting in 2009; (2) visit locations (eg, emergency department, long-term care) or grouped visit types representing focused scopes of practice (eg, pain medicine, palliative care) found in the ICES physician database11; and (3) Ontario Health Insurance Plan billing codes for certain procedures (eg, radiology, dialysis, pulmonary function testing).
Data Sources
We used the provincial corporate provider for information on physician characteristics, including their affiliation with a primary care patient enrollment model; the ICES Physician database for physician specialty and active status; the Ontario Health Insurance Plan database to assess fee-for-service physician claims for all physicians in Ontario, including the number of services and payment received; and the Statistics Canada postal code conversion files to derive neighborhood income quintiles by linking practice postal code to census dissemination area. We determined rurality by linking postal code with the Rurality Index of Ontario.20 Population estimates were based on deidentified, aggregated, publicly reported data from Statistics Canada.
Analyses
We used descriptive statistics to compare characteristics of physicians in focused practice with those in other practice types. We reported differences in characteristics between the first and last study years as the absolute difference in either the percentage (categorical variables) or the mean (continuous variables). We conducted sex-specific bivariate analyses looking at practice type by career stage, comparing 2009 to 2021 (focused practice assessment billing codes were introduced in 2009). We examined the most prevalent types of focused practice, by sex and overall. Finally, we looked at temporal trends in the overall number of family physicians, and by practice type, in relation to the population growth. We assessed the sensitivity of these findings by regrouping those classified as other into the comprehensive group.
The SAS Enterprise Guide, version 9.4 (SAS Institute Inc) was used to conduct all analyses. This study followed the Strengthening the Reporting of Observational Studies in Epidemiology reporting guidelines.
RESULTS
The total number of family physicians increased from 11,103 in 1993 to 17,413 in 2021; however, the mean number of days worked per physician decreased from 170 to 151 (Table 1). Over time, there was an increase in the percentage of family physicians who were female (28.1% to 48.8%) and age 55 years or over (18.4% to 36.3%). Of the additional 6,310 family physicians who entered the workforce during the study period, 39.5% were in focused practice and 85.0% were female family physicians. Overall, the percentage of family physicians in focused practice increased from 7.7% in 1993 to 19.2% in 2021. The focused practice group had fewer mean days worked in 2021 at 156 days as compared with 196 days for the comprehensive practice group.
Characteristics of Focused Practice Physicians vs Other Practice Types, 1993 and 2021
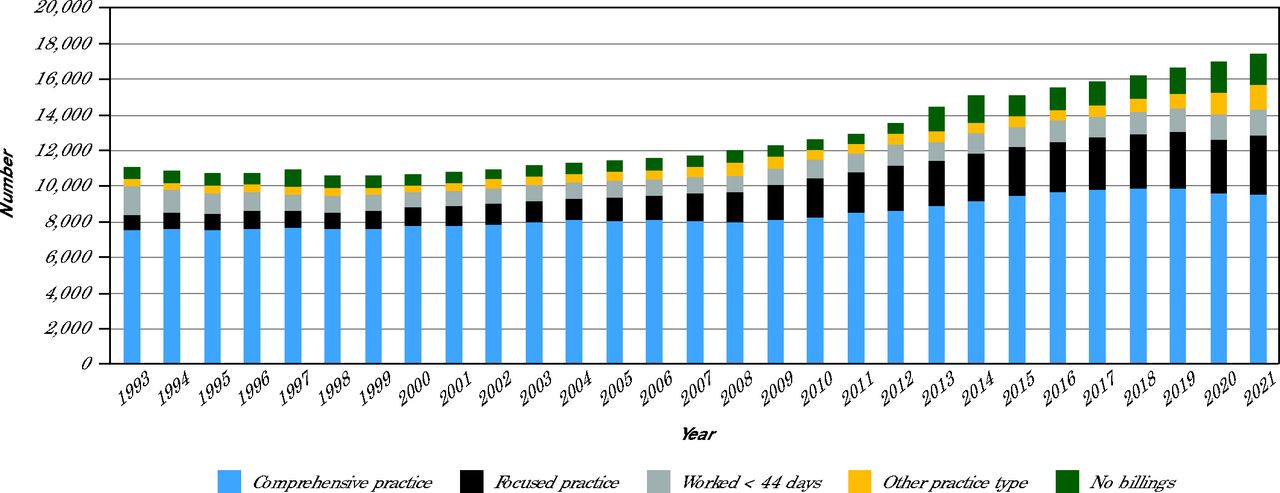
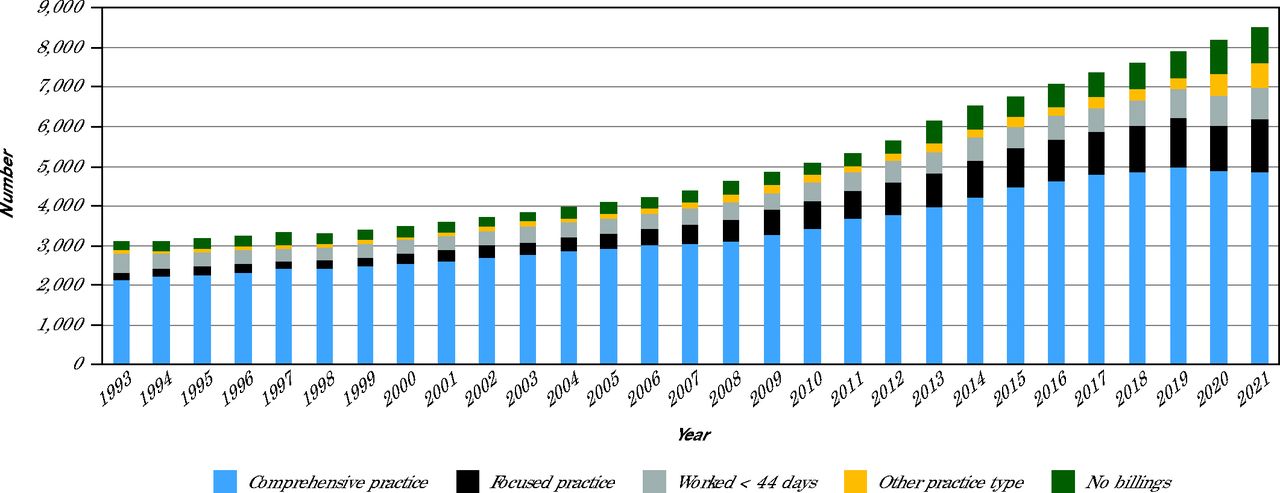
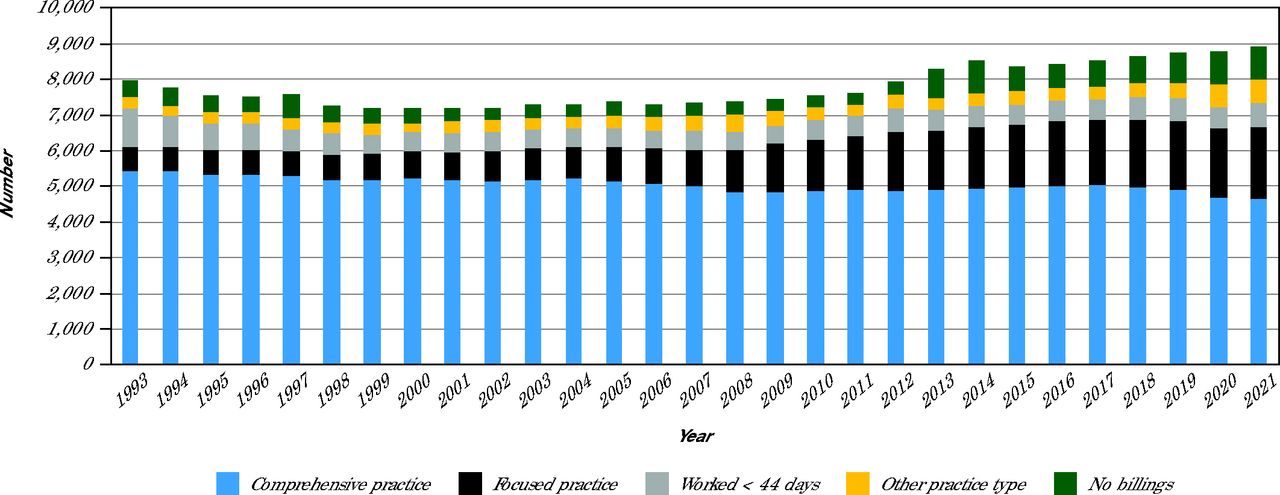
From 1993 to 2021, the percentage of all male family physicians in focused practice increased from 8% (669) to 23% (2,014) while the percentage of all female family physicians in focused practice increased from 6% (187) to 16% (1,337). At the end of the study period, there was a net increase of 944 male family physicians in the workforce, but an additional 1,345 males in focused practice and 771 fewer in comprehensive practice. In contrast, there were an additional 5,366 female family physicians in the workforce of which only 1,150 worked in focused practice. In 2021, 60% of focused practice physicians were male and 40% were female. Overall and sex-stratified trends in types of practice are summarized in Figure 1A-C.

Number of Family Physicians, by Practice Type, 1993-2021

Number of Female Family Physicians, by Practice Type, 1993-2021

Number of Male Family Physicians, by Practice Type, 1993-2021
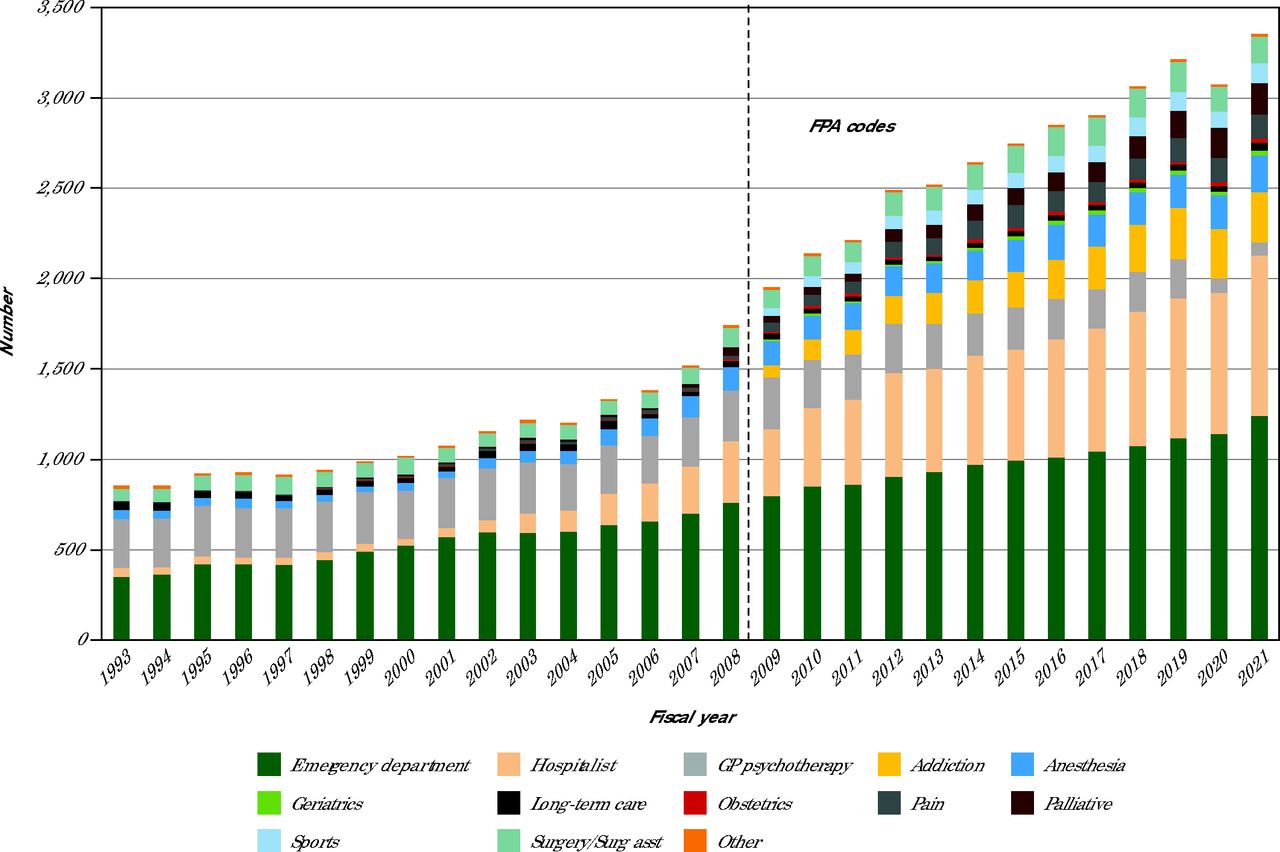
The 5 most prevalent focused practice types in 2021 were emergency medicine (37.0%), hospitalist medicine (26.5%), addiction medicine (8.3%), anesthesia (6.0%) and palliative medicine (5.1%) (Figure 2). There was a notable decline in the number of focused physicians in general practitioner psychotherapy, from 31.5% in 1993 to 2.2% in 2021. There was also some variation in the types of focused practice by sex (Supplemental Appendix 2). The most common type of focused practice among male physicians was emergency medicine (40.2% for males and 32.2% for females) while the most common type among female physicians was hospitalist work (32.2% for females and 22.6% for males).

Types of Focused Practice Physicians, 1993-2021
FPA = Focused Practice Assessment; GP = general practitioner; Surg asst = surgery assistant.
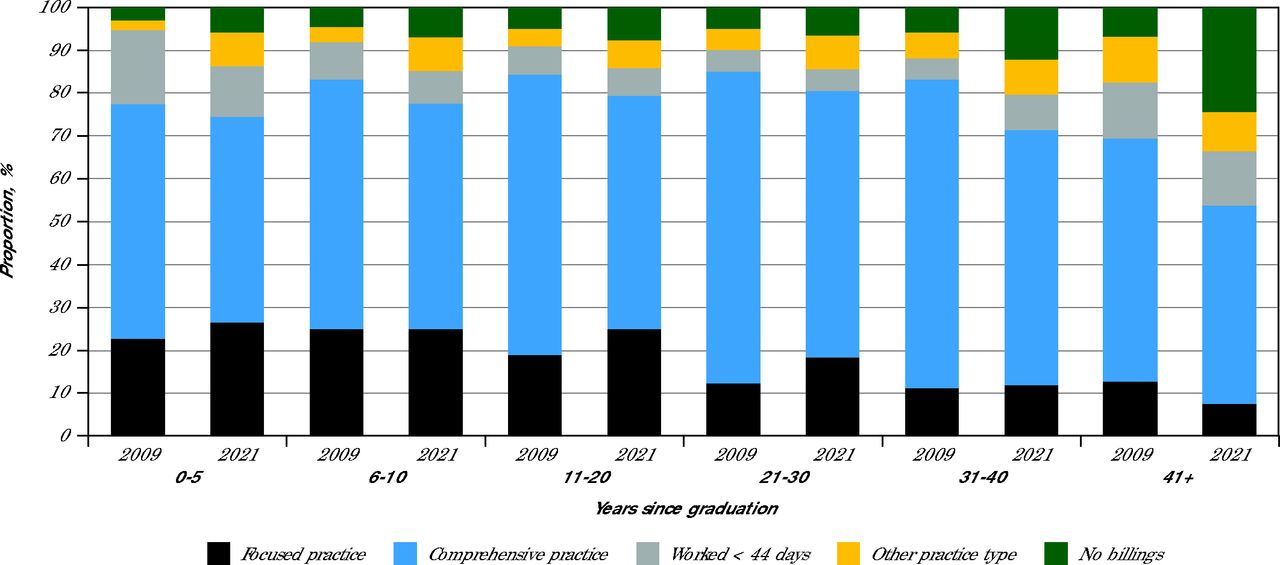
From 2009 to 2021, the percentage of family physicians doing focused practice stayed relatively stable or increased for all family physician graduation cohorts except for those graduating 41 or more years ago (Figure 3). The percentage doing focused practice, however, was higher among those graduating in the last 20 years (eg, in 2009, 22.7% among those graduating 0-5 years ago vs 11.3% among those graduating 31-40 years ago). There was a large increase from 2009 to 2021 in the percentage of family physicians doing focused practice in mid-career (from 31.3% to 43.5% for those graduating 11 to 30 years ago). For each graduation cohort, there were more male vs female family physicians working in focused practice (Supplemental Appendix 3).

Choice of Primary Care Practice Type, by Years From Graduation, 2009 vs 2021
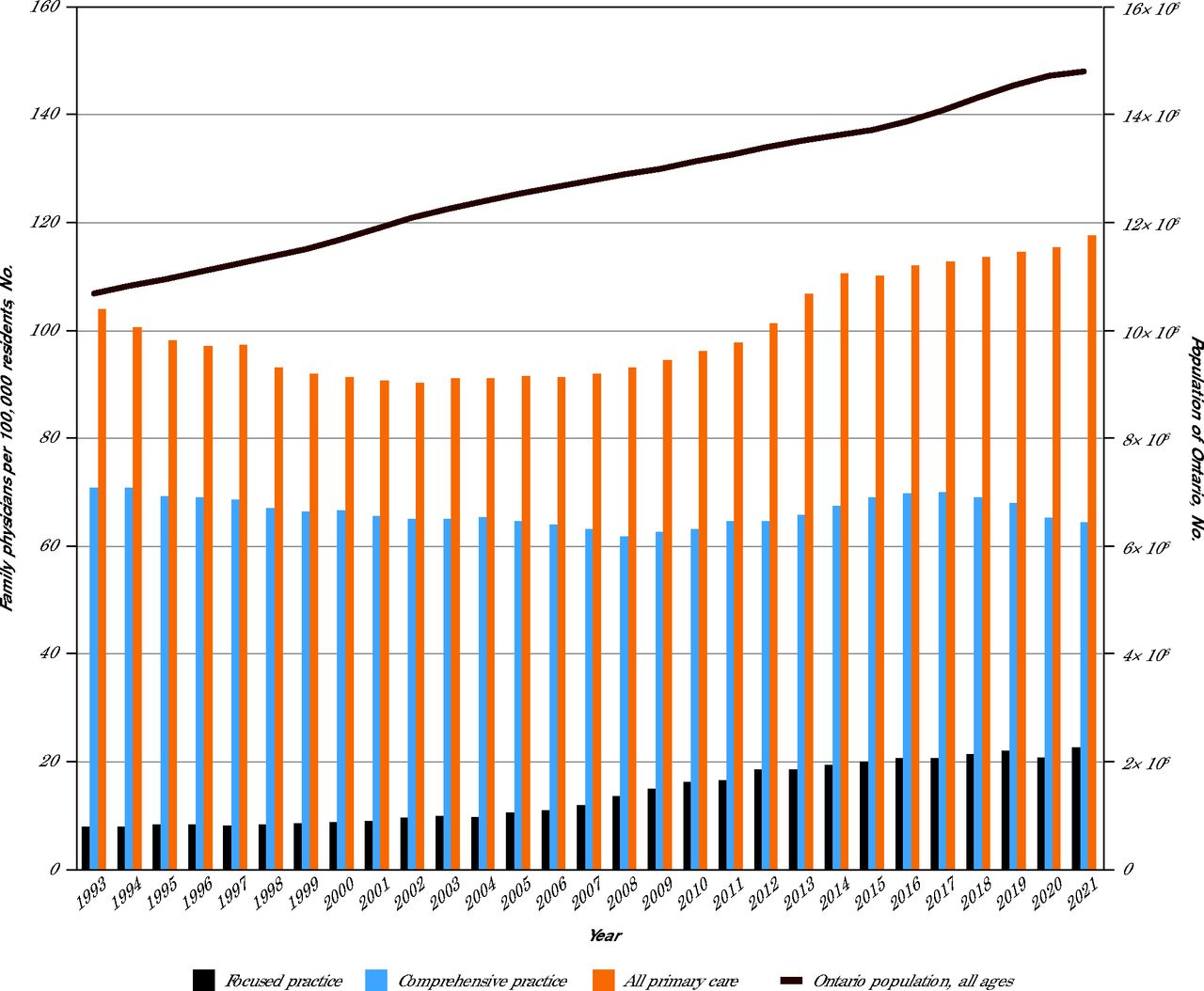
Ontario’s population (all ages) increased from 10.7 million in 1993 to 14.8 million in 2021, an increase of 38.5% (Figure 4). During this period, the number of family physicians increased by 14%, from 104 to 118 per 100,000. The number of focused family physicians increased from 8 to 23 per 100,000; however, the number of comprehensive family physicians decreased from 71 to 64 per 100,000. As part of sensitivity analyses, regrouping those classified as other with those in the comprehensive practice group showed a decrease from 75 to 73 family physicians per 100,000 (Supplemental Appendix 4), with impact on the magnitude but not the directionality of the trends.

Trends in the Number of Family Physicians Per Capita, by Practice Type, 1993-2021
DISCUSSION
In this repeated cross-sectional study comprising all active family physicians practicing in each fiscal year (1993 through 2021) in Ontario, Canada, we found that 1 in 5 were in focused practice in 2021 compared with 1 in 13 in 1993. Almost 40% of the growth in the total number of family physicians was attributable to focused practice, with emergency, hospitalist, and addiction medicine being most prevalent specialties. Although the proportion of focused practice family physicians was larger in early- and mid-career physicians, the decrease over time in the proportion of comprehensive physicians was apparent across all career stages. A greater proportion of male family physicians worked in focused practice. There was an increase in the overall number of family physicians, both in absolute terms and per capita, but a decrease in the proportion of comprehensive family physicians.
The decline in comprehensive family physicians is concerning due to the facts that 22% of Canadians lack access to primary care, population health needs are increasing, and the physician workforce is aging and nearing retirement.3,4,21 We found a decrease in the total number of family physicians in the first part of the study period (1993 to 2009) which is likely explained by pan-Canadian policies to reduce physician supply by reducing medical school and residency training spots in the 1990s.22 In contrast, the total number of family physicians per capita increased in the latter one-half of the study period, but only slightly over one-half of these were comprehensive family physicians by 2021. We also found that Ontario’s family physicians were increasingly female and on average, worked fewer days per year, trends consistent with other research.4 Although fewer female family physicians worked in focused practice compared with male colleagues, female physicians are known to have smaller rosters, take more time with patients, and work fewer hours.4,23-25 Taken together these findings caution against using a simple head count of family physicians to assess physician workforce supply.
Although causality cannot be directly inferred from our study, several changes to the health system and policy landscape may have contributed to the trends reported. One potential driver may have been the introduction of the designated focused practice billing codes which made focused practice more financially viable. Other factors may have been the restrictions on entry into capitation-based models and a pause on new team-based models.26 Most family medicine residents in Ontario train with preceptors in team-based capitation models, yet these options were no longer available to most graduates after 2012, potentially impacting career choice. The majority of focused practice family physicians pursued emergency or hospitalist medicine, with remarkable growth in the latter over the nearly 30-year period. Ontario hospitals have been under intense pressure to find financial efficiencies over the last decade and may have turned to family physicians as a way of maintaining services at reduced costs. In addition, changes in billing codes in the early 2010s increased remuneration for the most responsible physician providing care in hospital, making hospitalist work more financially rewarding. Furthermore, the number of specialist physicians per capita in Ontario is lower than Organization for Economic Co-operation and Development (OECD) comparator countries and may also drive the need for family physicians to play a role in hospitals.27
Family physicians may also be choosing focused practice, particularly hospital-based work, due to better remuneration, more job flexibility (ie, to take vacation or parental leaves), more team supports, no overhead, no hassles of running a small business, and overall better quality of life.13,28,29 Apart from personal or workplace-related factors, qualitative studies have also highlighted environmental-level drivers (eg, geography, local provider mix, regional economics) and population-level drivers (eg, increased prevalence of substance use).30 A complex interplay of a multitude of factors is likely driving the growth in hospitalist medicine,31 underscoring the significance of accounting for hospitalist medicine in workforce planning models going forward.
Our study has important limitations. We did not account for full-time equivalents, which may mean that we overestimated the provision of comprehensive care. There were likely some family physicians providing comprehensive care who were assigned to other categories. For example, exclusively salaried physicians working in Community Health Centers which provide care for 2% to 3% of Ontario’s population would have been classified as having no public billings. Similarly, some classified to the other practice type and focused practice groups may have provided some core primary care services, despite not meeting the eligibility criteria for comprehensiveness. To mitigate this, we conducted sensitivity analyses and included the physicians in other practice types with those in comprehensive practice. More work is needed to characterize physicians that were classified into the other practice type, worked less than 44 days, and no billings groups, and to validate the subcategories of focused practice ascertained through billing data. Finally, definitions of comprehensiveness and focused practice vary across jurisdictions as do policies affecting practice choices, thereby limiting external generalizability. A recent national investigation reported that 30% of Canadian family physicians are now practicing outside of primary care, however, rendering our findings as more conservative.32
CONCLUSIONS
Over the past 30 years in Ontario, Canada, there has been a decrease in the proportion of comprehensive family physicians and an increase in the proportion of family physicians pursuing focused practice, particularly emergency medicine and hospitalist work. Our findings caution against the exclusive use of family physician head counts in workforce planning. More research is needed to understand why family physicians are increasingly pursuing focused practice. Policy and practice changes, including better remuneration aligned to system goals, practice support, job flexibility, team-based care, and cross-sectoral health workforce planning, are needed to make comprehensive family practice the most attractive option to family physicians.
Footnotes
Conflicts of interest: authors report none.
Funding support: This study was supported by ICES, which is funded by an annual grant from the Ontario Ministry of Health (MOH) and Ministry of Long-Term Care. This study also received funding from the Canadian Institutes of Health Research (reference number SOP 162662), and the INSPIRE Primary Health Care Research Program which is funded through the Health Systems Research Program of the Ontario MOH. Parts of this material are based on data and information compiled and provided by Ontario MOH and the Canadian Institute for Health Information.
T.K. and R.H.G. are supported as Clinician Scientists by the Department of Family and Community Medicine (DFCM) at the University of Toronto and at St Michael’s Hospital and L.J. is a Clinician Investigator supported at the DFCM at the University of Toronto and Sunnybrook Health Sciences Centre. T.K. is the Fidani Chair of Improvement and Innovation in Family Medicine at the University of Toronto. M.E.G. is supported by the Brian Hennen Chair in Family Medicine at Queen’s University. Dr Premji is supported by the Junior Clinical Research Chair in Family Medicine at the University of Ottawa and is a PSI Knowledge Translation Fellow. H.A. is supported by the Canadian Institutes of Health Research Postdoctoral Health System Impact Fellowship, and Ontario Health.
Role of the Funder/Sponsor: The funders had no role in the design and conduct of the study; collection, management, analysis, and interpretation of the data; preparation, review, or approval of the manuscript; and decision to submit the manuscript for publication.
Disclaimer: The analyses, conclusions, opinions, and statements expressed herein are solely those of the authors and do not reflect those of the funding or data sources; no endorsement is intended or should be inferred.
Previous presentation: Canadian Association of Health Services and Policy Research; May 15, 2024; Ottawa, Canada.
Data sharing statement: The data set from this study is held securely in coded form at ICES. While legal data sharing agreements between ICES and data providers (eg, health care organizations and government) prohibit ICES from making the data set publicly available, access may be granted to those who meet pre-specified criteria for confidential access, available at www.ices.on.ca/DAS (email: das{at}ices.on.ca). The full data set creation plan and underlying analytic code are available from the authors upon request, understanding that the computer programs may rely upon coding templates or macros that are unique to ICES and are therefore either inaccessible or may require modification.
Additional information: This study used data adapted from the Statistics Canada Postal CodeOM Conversion File, which is based on data licensed from Canada Post Corporation, and/or data adapted from the Ontario Ministry of Health Postal Code Conversion File, which contains data copied under license from Canada Post Corporation and Statistics Canada
- Received for publication August 11, 2024.
- Revision received January 5, 2025.
- Accepted for publication January 20, 2025.
- © 2025 Annals of Family Medicine, Inc.
References
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.