
Abstract
PURPOSE There is debate about whether community health centers (CHCs) will experience increased demand from patients gaining coverage through Affordable Care Act Medicaid expansions. To better understand the effect of new Medicaid coverage on CHC use over time, we studied Oregon’s 2008 randomized Medicaid expansion (the “Oregon Experiment”).
METHODS We probabilistically matched demographic data from adults (aged 19–64 years) participating in the Oregon Experiment to electronic health record data from 108 Oregon CHCs within the OCHIN community health information network (originally the Oregon Community Health Information Network) (N = 34,849). We performed intent-to-treat analyses using zero-inflated Poisson regression models to compare 36-month (2008–2011) usage rates among those selected to apply for Medicaid vs not selected, and instrumental variable analyses to estimate the effect of gaining Medicaid coverage on use. Use outcomes included primary care visits, behavioral/mental health visits, laboratory tests, referrals, immunizations, and imaging.
RESULTS The intent-to-treat analyses revealed statistically significant differences in rates of behavioral/mental health visits, referrals, and imaging between patients randomly selected to apply for Medicaid vs those not selected. In instrumental variable analyses, gaining Medicaid coverage significantly increased the rate of primary care visits, laboratory tests, referrals, and imaging; rate ratios ranged from 1.27 (95% CI, 1.05–1.55) for laboratory tests to 1.58 (95% CI, 1.10–2.28) for referrals.
CONCLUSIONS Our results suggest that use of many different types of CHC services will increase as patients gain Medicaid through Affordable Care Act expansions. To maximize access to critical health services, it will be important to ensure that the health care system can support increasing demands by providing more resources to CHCs and other primary care settings.
- community health centers
- primary care utilization
- Medicaid
- Patient Protection and Affordable Care Act
- ACA
- Oregon Experiment
- health policy
- practice-based research
- vulnerable populations
INTRODUCTION
The Patient Protection and Affordable Care Act (ACA) created health insurance coverage options for millions of people in the United States.1–3 It is predicted that ACA insurance expansions will lead to increased demand for primary care services by those gaining coverage.4–6 Community health centers (CHCs) currently provide primary care and other critical services to many uninsured patients likely to be affected by the ACA. For example, in 2012, CHCs provided care to an estimated 21 million patients; 36% of these patients were uninsured and 40% were covered by Medicaid.7 It is unknown whether ACA expansions will affect use of CHCs. Some postulate that individuals who gain Medicaid will increase their use of CHCs, contrary to other assumptions that the newly insured will go elsewhere.8–13
Predictions of individuals’ increased health care demand after gaining insurance are based on studies showing an association between coverage and better access to health care.14 Most of these previous studies examined coverage gains that occurred as a result of major life changes (eg, aging, disability, new job).15–17 Other studies attempted to isolate the effect of gaining insurance by assessing “natural policy experiments” in which individuals gained coverage because of a policy change, rather than a potentially confounding life event.9,18–22 For example, studies of Massachusetts’ 2006 expansions found that patients who gained coverage used ambulatory care services at higher rates postcoverage.9,19–21 This body of quasiexperimental research is based on the assumption that the observed changes in outcomes are caused by a change in insurance status and not due to unmeasured confounding variables.23 Assessing persons randomly assigned to an intervention leading to insurance coverage (or no coverage) would yield stronger data for establishing causality, but it is nearly impossible to design such a study.24–26
The “Oregon Experiment” provides a rare opportunity to assess causality within an insurance intervention.26–30 In 2008, the Oregon Health Plan (OHP) reopened enrollment for its expansion Medicaid program (OHP Standard), seeking to enroll 10,000 noncategorically eligible adults (ie, persons not meeting federally mandated eligibility criteria). OHP Standard had been closed to new enrollment since 2004, so it was anticipated that demand for enrollment would exceed the allocated budget. Uninsured, low-income adults were encouraged to put their names on a “reservation list.” From this list, there were 8 random drawings; individuals selected in these drawings were invited to apply for OHP coverage. The reservation list included more than 90,000 names; approximately 30,000 people were randomly selected to apply, and approximately 10,000 were enrolled.30 Detailed information about the Oregon Experiment is available elsewhere.26–28,30
Early studies of the Oregon Experiment found increased demand for primary care services among patients who gained coverage based on respondents’ self-reported use and receipt of care.26,28 To confirm these findings and specifically quantify the effect of gaining Medicaid coverage on use of CHCs, we analyzed electronic health record (EHR) data from 108 CHCs to examine CHC use among more than 30,000 patients during the initial 36 months after the Oregon Experiment. These data allow us to retrospectively capture postintervention data directly from a patient’s medical record without risk of biases inherent in self-report (eg, recall bias, nonresponse bias).31–35 This is the first study to directly examine CHC use among Oregon Experiment participants.
METHODS
Data Sources
OCHIN (originally the Oregon Community Health Information Network, but shortened to OCHIN when membership expanded beyond Oregon) supports more than 300 CHC sites in 20 states by providing a centrally hosted EHR.36,37 We used EHR data from the 108 CHC sites in Oregon that were part of the OCHIN practice-based research network in 2007–2011. State administrative data were used to identify OCHIN CHC patients on the reservation list; Oregon’s Medicaid enrollment data were used to determine periods of Medicaid coverage.
Study Population
We used Link Plus software (Centers for Disease Control and Prevention)38 and demographic variables common to both data sets to probabilistically match 100,407 individuals on the reservation list to all 515,575 patients in the OCHIN database (Figure 1). Two research staff (S.R.B. and another staff member) independently validated matches and performed case-by-case review of uncertain matches. We identified 35,411 matched individuals, 13,422 of whom were selected to apply for coverage, and 21,989 of whom were not selected. To preserve randomization, individuals were not required to have a visit during the study period and we applied minimal exclusions: we excluded patients aged younger than 19 years (26 patients) and older than 64 years (404 patients), patients not alive at the end of the postselection period (130 patients), and those with unknown sex (2 patients). Our final study population consisted of 34,849 patients: 13,219 selected to apply for coverage and 21,630 not selected.
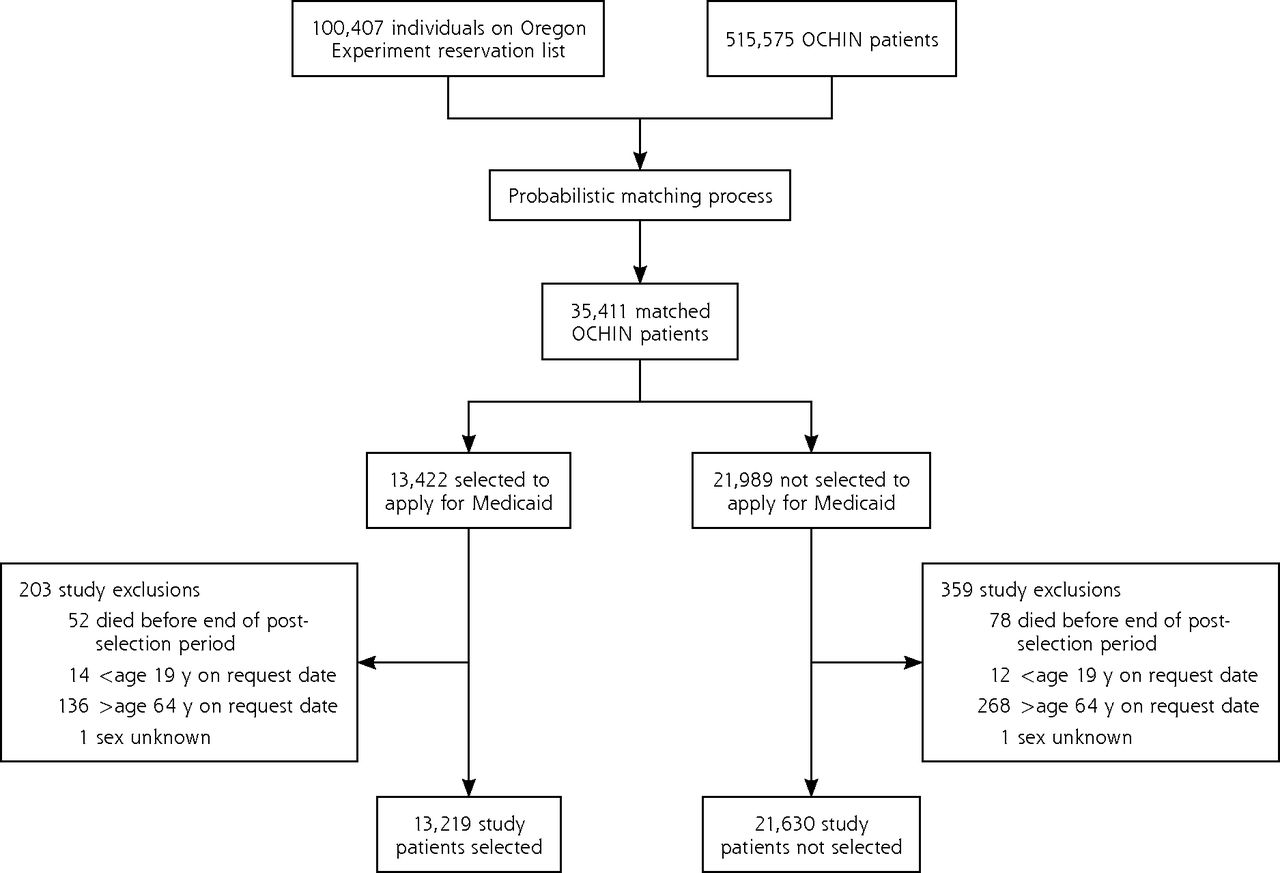
Study population flow diagram.
Analytic Approach
Random selection to apply for Medicaid coverage occurred through drawings held between March 2008 and October 2008. Individuals on the reservation list were not screened for eligibility before the randomization. If selected, an individual was invited to complete an application that was used to determine eligibility; thus, some selected individuals were deemed ineligible to receive coverage via the Experiment or did not return the application after randomization.30 Among selected individuals, coverage “start dates” were retroactively assigned as the date of selection notification (the selection date). Persons not selected to apply for coverage were randomly assigned a 2008 selection date based on the distribution of selection dates among those selected to apply.
To preserve the randomization, we first conducted an intent-to-treat (ITT) analysis comparing use between patients randomly selected to apply for Medicaid coverage vs those not selected. This analysis included all patients regardless of whether those selected to receive the “treatment” (ie, insurance coverage) actually received it. The ITT analysis maintains covariate balance generated from the random selection and limits inferences based on arbitrary subgroups of patients in the trial.39 A substantial number of individuals randomly selected in the Oregon Experiment did not actually gain Medicaid coverage, however. Because our primary interest was to estimate the effect of actually gaining Medicaid on health care use, we considered 2 analytic techniques: an effect of treatment on the treated (ETOT) approach and an instrumental variable (IV) approach. The ETOT approach is conducted in many randomized trials but has limitations because of bias introduced when treated and nontreated groups differ. The IV approach was developed as a more valid way to address some of those limitations and is preferred when appropriate “instrument(s)” can be identified. The IV approach is designed to provide unbiased, consistent estimates when unobservable factors are present and correlated with the treatment and outcome variable. The benefit of the IV approach is that, if its assumptions hold, it provides a causal estimate of gaining Medicaid on use, as opposed to a measure of association.40
Fortunately, we were able to identify 2 valuable instruments for conducting an IV analysis in this study: random selection to apply for Medicaid and having any Medicaid coverage in the 12 months before selection. The treatment variable was having at least 6 months of continuous Medicaid coverage in the postselection period starting from the selection date. Because the IV analysis is a stronger methodologic approach than the ETOT analysis, we include the methods and results of the IV analysis here. (ETOT findings are given in Supplemental Appendix Tables 1 and 2, available at http://www.annfammed.org/content/13/4/312/suppl/DC1.)
Use Outcomes
We measured rates of use of CHC services in the 36 months after the selection date (the postselection period). The use outcomes were primary care office visits, behavioral/mental health visits, laboratory tests, referrals, immunizations, and imaging. Laboratory tests, referrals, immunizations, and imaging were identified using standard procedure codes (eg, Current Procedural Terminology) and groupers that categorize data and inform quality performance assessments in the OCHIN EHR.10,41 Not all clinics had the EHR capability to designate behavioral/mental health visits; therefore, these analyses were limited to the subset of 33 clinics with the behavioral/mental health indicator.
Covariates
We used EHR data to obtain patient age, sex, race/ ethnicity, household income, and baseline health status. Patients’ household income was collected at visits as percent of federal poverty level; we created a composite federal poverty level based on the average from visits wherein this information was collected. To measure baseline health status, we assessed diagnosis of 5 chronic conditions—asthma, coronary artery disease, diabetes, dyslipidemia, and hypertension—before each patient’s selection date using standard code sets as part of EHR Meaningful Use criteria42 or the Healthcare Effectiveness Data and Information Set (HEDIS).43 A patient was considered to have a given condition if a qualifying diagnosis code appeared on the problem list or in at least 2 encounters before the selection date.
Statistical Methods
ITT Analyses
We first described and assessed differences between those randomly selected and not selected, using χ2 tests for categorical variables and 2-sample t tests for continuous variables. Next, we conducted ITT analyses, comparing use in the 36-month postselection period between the selected and nonselected groups. To better model the distribution of the use count data, we considered several regression models. The Vuong test44 suggested that the zero-inflated Poisson (ZIP) models45 provide a better fit to the data than standard Poisson regression, owing to the number of zeroes and data dispersion. These ZIP models were adjusted for baseline covariates that differed significantly between selection groups. We calculated rate ratios between the groups and monthly outcome rates per 1,000 patients. Robust clustered sandwich estimators of the variance46,47 were used to estimate rate ratio confidence intervals to correct for clustering of patients within CHCs.
IV Analyses
Many people randomly selected to apply did not submit an application. Further, as eligibility for Medicaid was not determined until after an individual had been selected and submitted a full application, some people on the reservation list did not meet income requirements or already had Medicaid coverage, making them ineligible to obtain coverage via the Oregon Experiment. To address these potential issues, we used IV analyses to estimate the causal effect of gaining Medicaid coverage on CHC use during the 36-month period after random selection. To be considered valid instruments,48 variables must be associated with Medicaid coverage, but must not be associated with the use outcome except through its effect on Medicaid coverage. Under these criteria, we used 2 IVs that met the standards for valid instruments: (1) selection status in the Oregon Experiment (randomly selected to apply, or not) and (2) Medicaid coverage status in the 12 months before selection (any or none). Both of these variables were strongly associated with postselection period coverage, but neither would be expected to be directly associated with postselection period use except through their association with postselection period coverage. For consistency and because the Vuong test suggested a ZIP model to be a better fit for the use outcomes, we used 2-stage residual inclusion IV models49 instead of 2-stage ordinary least-squares IV models as the former have shown to be more consistent and less biased for complex models such as the ZIP model.50 The 2-stage residual inclusion models controlled for age and race/ethnicity. The validity of the instruments was tested using an overidentification test.51 We used bootstrapping with 2,000 repetitions clustered by CHC52 to obtain confidence intervals for the rate ratio estimates accounting for clustering of patients within CHC. All statistical tests were 2-sided, and statistical significance was defined as a P value less than .05. Statistical analyses were performed using SAS version 9.3 (SAS Institute Inc) and Stata version 12.1 (StataCorp). This study was approved by the institutional review board at Oregon Health & Science University.
RESULTS
Demographics
The majority of study patients were female (57.8%), were non-Hispanic white (65.3%), and had a household income of less than 100% of the federal poverty level (62.2%) (Table 1). The selected and nonselected groups differed significantly with respect to race/ethnicity and categorical age; however, the percentage differences were relatively small.
Demographic Characteristics of Study Sample by Selection Status (N = 34,849)
Ultimately, 39.8% of the selected group gained Medicaid coverage, compared with 10.1% of the non-selected group.
ITT Analyses
In adjusted ITT analyses, compared with nonselected patients, patients selected to apply had significantly lower rates of behavioral/mental health visits (adjusted rate ratio [aRR] = 0.89; 95% CI, 0.81–0.99) and higher rates of referral (aRR = 1.18; 95% CI, 1.02–1.35) and imaging (aRR = 1.08; 95% CI, 1.01–1.16) in the 36-month postselection period (Table 2). The 2 groups did not differ significantly with respect to primary care office visits, laboratory tests, and immunizations.
Intent-to-Treat Outcome Rates by Selection Group (Selected n = 13,219; Not Selected n = 21,630)
IV Analyses
Table 3 displays the causal effects of gaining Medicaid coverage on CHC use in the 36-month postselection period, estimated by the IV approach. The 2-stage residual inclusion model estimates indicated that participants who received Medicaid coverage had significantly more primary care office visits compared with those who did not, with 81 additional visits per 1,000 Medicaid-covered patients per month (aRR = 1.39; 95% CI, 1.16–1.66). The number of primary care office visits per month was 282 per 1,000 Medicaid-covered patients, compared with 201 for patients without such coverage. Medicaid coverage led to a 58% higher rate of referrals (aRR = 1.58; 95% CI, 1.10–2.28), with gastrointestinal and orthopedic referrals being the most common for both groups. Receipt of Medicaid coverage also resulted in a 27% higher rate of orders for laboratory tests (aRR = 1.27; 95% CI, 1.05–1.55) and a 33% higher imaging rate (aRR = 1.33; 95% CI, 1.07–1.64) in the 36-month postselection period. We found no significant effect of Medicaid coverage on behavioral/ mental health visit rates and immunization rates.
Estimated Effect of Gaining Medicaid Coverage on Use Outcomes Among Oregon OCHIN Patients Who Participated in the Oregon Experiment (N = 34,849)
DISCUSSION
To better predict how use of CHC services might change after ACA Medicaid expansions, we studied primary care use over a 36-month period among a population of low-income adult CHC patients who gained coverage after Oregon expanded its Medicaid program in 2008. Consistent with previous studies of self-reported data from Oregon Experiment participants in general primary care settings,26,53 our results suggest that use of primary care services in CHCs will increase when patients gain Medicaid through ACA insurance expansions. The fact that we found an increase in specialty services (referrals, imaging, laboratory tests) in CHCs among those who gained Medicaid insurance is promising because it suggests that as CHC patients gain insurance via the ACA, they will be able to access services that have been difficult to obtain while uninsured.54,55
Our findings have important implications. Accessible and appropriate primary care services are associated with improved health outcomes.56–58 Insurance coverage acts interdependently with access to primary care to accomplish these outcomes.59–61 Our analyses—and others—suggest that insurance expansions could lead to increased demand for services from CHCs and other primary care settings. To ensure these crucial services are available, CHCs and other primary care settings need more resources. One study projected the need for an estimated 52,000 additional primary care physicians by 2025, with 8,000 of those necessary just to meet the needs of patients newly covered under the ACA by 2020.62 As in Massachusetts, if primary care services are not expanded to meet this need, patients who gain insurance coverage may seek emergency department care for primary care–treatable conditions.63 Primary care workforce shortages and other access barriers might help to explain the higher emergency department visit rates observed among those who gained Medicaid coverage in a prior Oregon Experiment study, compared with those who remained uninsured.29
Our findings strengthen observational evidence of positive associations between insurance coverage and increased access to primary care services.10,14,64–66 Our use of EHR data enabled direct capture of care received, allowing us to overcome potential biases that can result when asking patients to recall services received.34,35 The EHR data also provided information about services used during periods without health insurance, thus overcoming past limitations of analyzing insurance claims (billing) data, which only report use when a patient has insurance coverage.67–69 The randomization component of Oregon’s 2008 Medicaid expansion enabled us to examine both the effects of being selected to apply for Medicaid coverage (through the randomization process and ITT analyses) and the isolated effect of actually gaining Medicaid coverage (through the IV techniques).
Limitations
We found that patients continue to seek health care services from CHCs and increased their use of many different types of CHC services after obtaining insurance; however, we were unable to assess the extent to which study participants sought care at non-study CHC settings. Research suggests that federally qualified health centers are more likely to see patients newly insured via Medicaid compared with other providers70; however, future studies are needed to determine what percent of patients seek care elsewhere after receiving insurance to more accurately assess the net impact on demand patterns in these settings.
Although individuals in this study were similar to those gaining Medicaid through ACA-supported expansions, participation in the Oregon Experiment was voluntary, and ACA policies include a coverage mandate. Further, this study was conducted in a single state and may not be generalizable to others.
In IV analyses, we used 2 instruments: random selection to apply for OHP and preexisting Medicaid coverage. Such models assume that the instruments are not correlated with the outcomes, except indirectly through the treatment variable (Medicaid coverage). It is possible that preexisting Medicaid coverage correlated with establishing care at a CHC, but it is unlikely that coverage in the past would directly affect future use of CHC services independent of postselection period coverage, particularly in CHCs that provide services to uninsured patients. The ETOT findings (Supplemental Appendix Table 2) were consistent with what was observed in the IV approach, increasing our confidence in the results of this study. Additionally, tests of overidentifying restrictions for the inclusion of 2 IVs provide support for the set of study instruments (results not shown).
Finally, although we did not find an increase in use of mental/behavioral health services, we assessed only services provided in the primary care setting. We were not able to assess use of services for more severe mental health conditions that likely prompted referral for specialty care. Research suggests that recent policy changes (parity law) are associated with increased use of services for a subset of patients with more severe mental illness.71,72
Conclusions
Results from this randomized insurance experiment suggest that use of primary care services in CHCs will increase when patients gain Medicaid through ACA insurance expansions. If the US health care system adequately expands resources in CHCs and other primary care settings to fully meet this demand, it could lead to better access to health care for previously uninsured patients. If the US health care system is not able to adequately provide primary care services, potential gains in population health may not be realized, and health care costs will increase unnecessarily if patients must seek hospital care for primary care–treatable conditions.
Acknowledgments
The authors gratefully acknowledge the OCHIN network and the OCHIN PBRN.
Footnotes
Conflicts of interest: authors report none.
This study has been registered as an observational study at clinicaltrials.gov (NCT02355132).
Funding support: This study was supported by grant R01HL107647 from the National Heart, Lung, and Blood Institute, and grant K08HS021522 from the Agency for Healthcare Research and Quality.
Disclaimer: The funding agencies had no involvement in the design and conduct of the study; analysis and interpretation of the data; and preparation, review, or approval of the manuscript.
Previous presentations: How Did the Oregon Medicaid Experiment Affect Utilization of Health Care Services Among Patients of Federally-Qualified Health Centers? Oral presentation at the 2014 North American Primary Care Research Group Annual Meeting; November 21–25, 2014; New York City, New York.
Supplementary materials: Available at http://www.AnnFamMed.org/content/13/4/312/suppl/DC1/.
- Received for publication February 12, 2015.
- Revision received May 15, 2015.
- Accepted for publication May 26, 2015.
- © 2015 Annals of Family Medicine, Inc.




{kind=link}