
Article Figures & Data
Figures
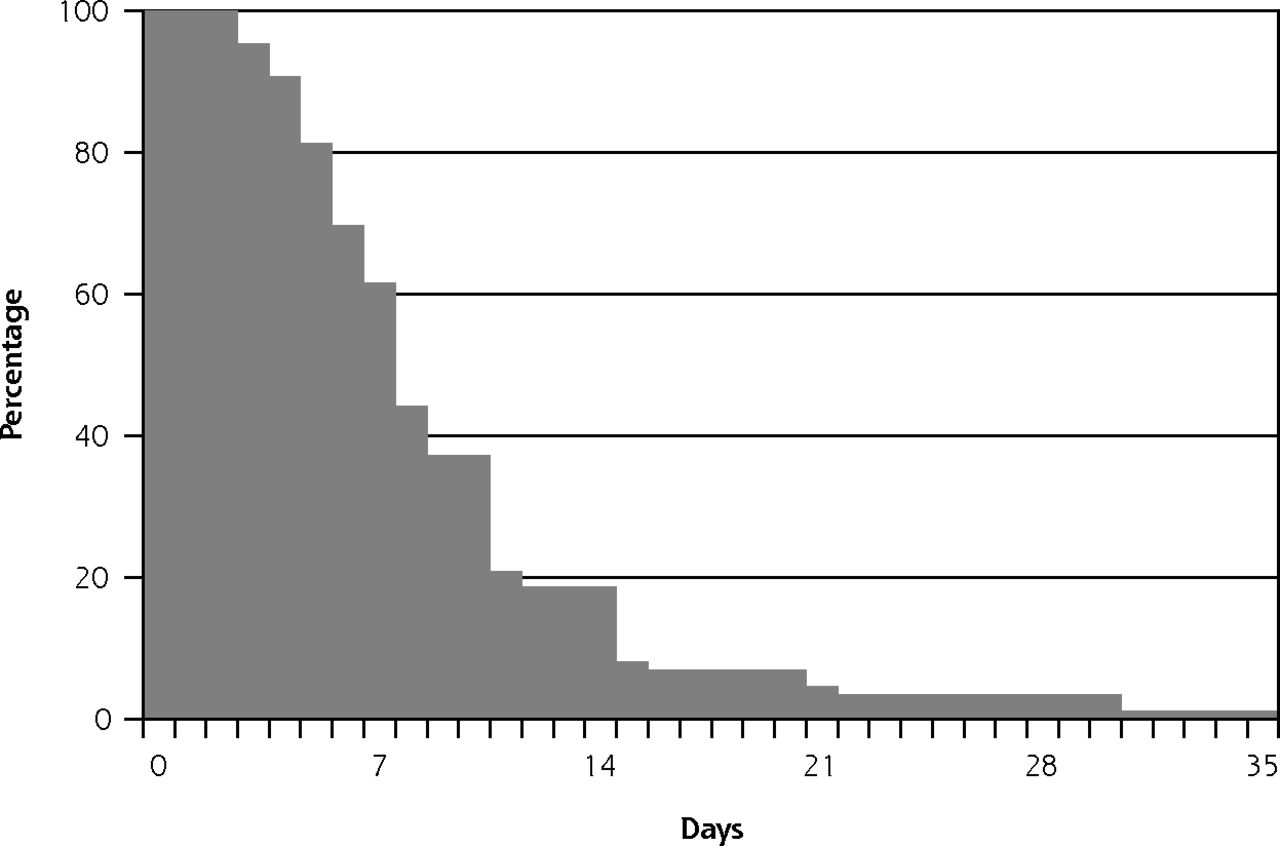
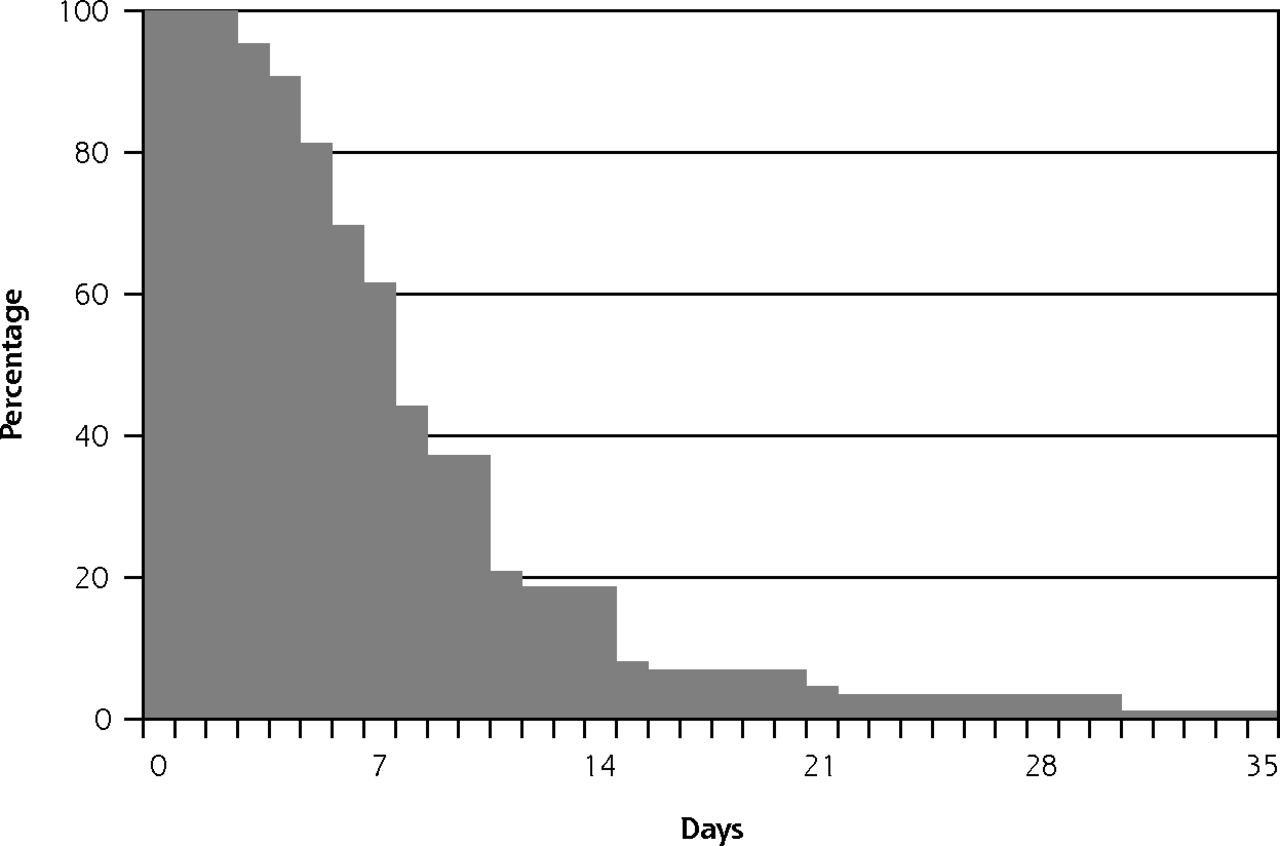
- Figure 1
Cumulative survival curve for duration until death after start of VSED.
VSED = voluntary stopping of eating and drinking.
Note: Median time to death was 7 days. Data for 86 patients; 10 responding physicians did not remember, and 3 missing (13.1%).
Tables
- Table 1
Background Characteristics of Physician Respondents: Family Physicians With and Without VSED Experience
Characteristic Total (N = 708) Experience With VSED (n = 313) No Experience With VSED (n = 383) Age, y Mean (SD)a 50 (8) 52 (8) 49 (9) Range 31–72 32–70 31–72 Sex, male, % 61 62 60 Is religious, %b 37 36 39 Working experience as family physician, y Mean (SD)a 19 (9) 20 (9) 18 (9) Range 1–42 2–39 1–42 Additional expertise, % Received training in palliative carec 73 75 72 Palliative care consultant 2 2 3 Experiences with VSED, % Experience with VSED 46 100 NA Experience with VSED in the last year 9 19 NA Palliative sedation in VSED, % Has administered palliative sedation in case of VSED 23 47 NA Conceivable to administer palliative sedation in case of VSEDa,d,e 81 90 73 PAS, % Has performed PAS 79 82 77 Conceivable to perform PASd 93 93 92 VSED and PAS, % Has ever suggested VSED to a patient with a wish for PASa 34 49 21 NA = not applicable; PAS = physician-assisted suicide; VSED = voluntary stopping of eating and drinking.
Note: Missing values ranged from 1.0% to 3.8%, unless otherwise specified.
↵a Significant difference between respondents with experience with VSED and respondents without this experience, calculated by Fisher’s exact test (2-tailed) for dichotomous variables and by independent t test for continuous variables. P <.001 in all cases.
↵b As described by respondent. Religion was Christianity in 93% of cases.
↵c Not including regular curricular training.
↵d Physicians who had done so were categorized under conceivable.
↵e Missing values for 13.1%.
Characteristic % (95% CI) Age at the time of death ≤65 y 6 (3–13) 66–80 y 23 (16–33) >80 y 70 (60–78) Partner Yes 25 (18–35) No, widow(er) 64 (54–72) No, other 11 (6–19) Residence Home (independently or with family) 52 (42–62) Residential home 42 (33–52) Hospice 5 (2–12) Other 1 (0–6) Diagnosisa A somatic disease, not cancerb 39 (30–49) Cancer 27 (19–37) (Early-stage) dementia 12 (7–20) Psychiatric disease 7 (3–14) No severe physical or psychiatric disease 24 (17–34) ECOG performance statusc 0 4 (1–10) 1 8 (4–15) 2 11 (6–19) 3 47 (38–57) 4 29 (21–39) Life expectancy <1 wk 2 (0–8) 1–4 wk 32 (23–41) 1–12 mo 41 (32–51) >1 y 26 (18–35) Patient was mentally competent Yes 90 (83–95) Partly 7 (3–15) Nod 2 (0–8) ECOG = Eastern Cooperative Oncology Group; VSED = voluntary stopping of eating and drinking.
Note: Missing values ranged from 0.0% to 5.1%.
↵a Respondents could give one or more answers.
↵b 10% Neurologic disease, 10% musculoskeletal or rheumatic disease, 9% cardiovascular disease, 7% respiratory disease, 6% sensory loss or general decline, 4% pain syndrome, 3% diabetes, 4% other.
↵c ECOG performance status: (0) fully active; (1) restricted in physically strenuous activity but ambulatory and able to carry out light work; (2) ambulatory, capable of all self-care but unable to carry out work activities; up and about more than 50% of waking hours; (3) capable of only limited self-care, confined to bed/chair for more than 50% of waking hours; (4) completely disabled, no self-care possible, totally confined to bed or chair.27
↵d Two patients were not mentally competent: 1 had depression and 1 had depression and early-stage dementia.
- Table 3
Family Physician-Reported Patients’ Motives for Decisions to Hasten Death by VSED (99 Patients) and Physician Involvement
Characteristic % (95% CI) Patient’s Motive Somatic 79 (70–86) Fatigue, general weakness 60 (50–69) Physical deterioration 51 (41–60) Pain 18 (11–26) Dyspnea 9 (5–17) Other physical symptoms 8 (4–16) Existential 77 (68–85) Suffering without hope for improvement 41 (32–51) Tired of living 40 (32–51) Missing a purpose in life 38 (29–48) Dependence 58 (48–67) Being dependent 32 (23–42) Disability, immobility 30 (22–40) (Fear of) loss of autonomy 27 (19–36) Not wanting to be a burden on family anymore 15 (9–24) No longer being able to reside independently 7 (3–14) Loss of dignity, loss of self 37 (28–47) Loss of dignity 29 (21–39) Cognitive decline or inability to communicate 11 (6–19) Social 21 (14–30) Loneliness 15 (9–24) Death of a loved one 8 (4–16) Psychiatric suffering 14 (9–23) Depressive symptoms 13 (8–22) Fear, anxiety 3 (1–9) Physician’s involvement and attitude Physician had suggested the possibility of VSED to the patient 18 (11–27) Physician could agree with the patient’s decision to hasten death by VSED 94 (87–97) Patient had requested for PAS 19 (12–28) PAS = physician-assisted suicide; VSED = voluntary stopping of eating and drinking.
Note: Missing values ranged from 2.0% to 4.0%.
Characteristic % (95% CI) Preparation phase Physician was informed of the patient’s intention in advance Yes, by the patient 46 (36–56) Yes, by the patient’s proxy 4 (1–11) No, but the patient had stated that he/she did not want to continue living 25 (17–35) No 25 (17–35) Physician or proxy involvement No family physician or proxy 16 (10–24) Family physician (for guidance, support, or care)a In preparing for VSED 21 (14–30) During the process of VSED 55 (45–65) Palliative sedation until death 28 (20–38) No 38 (28–48) Proxiesa In preparing for VSED 44 (34–54) During the process of VSED 53 (43–63) No 28 (20–38) Don’t know 3 (1–9) Terminal phase Symptoms in the last 3 days before deathb Yes 36 (28–46) None 42 (32–52) None (but palliative sedation was given) 10 (6–18) Don’t know 11 (6–20) Symptoms reportedc,d Pain 14 (8–23) Fatigue 9 (5–18) Impaired cognitive functioning 8 (4–16) Thirst or dry throate 7 (3–15) Delirium 6 (2–13) Dyspnea 6 (2–13) Reduced consciousness 5 (1–12) Agitation 5 (1–12) Impaired communication 4 (1–10) Otherf 6 (3–15) Physicians’ impression that dying process went according to the patient’s wish Yes 80 (71–87) Partly 18 (11–27) No 2 (0–8) If partly or no, reason whyc Duration too long 11 (6–20) Patient preferred PAS 3 (1–9) Communication problems 1 (0–6) Inability to say goodbye 1 (0–6) Agitation 1 (0–6) PAS = physician-assisted suicide; VSED = voluntary stopping of eating and drinking.
Note: Total number of cases was 96, as data for 3 patients were missing (3.0%).
↵a Respondents could give 1 or more answers.
↵b Phrasing of the question: “Did the patient have physical, psychological or other symptoms or complaints in the last 3 days before death?”
↵c Open-ended question; respondent could give multiple answers.
↵d n = 85, 11 did not know, 3 missing (13.9%).
↵e Thirst 3%, dry mouth or throat 3%.
↵f Other: decubitus (2%), (deterioration of) heart failure (2%), gloom or sadness (2%), edema (1%), problems ingesting medication (1%).
The Article in Brief
Primary Care Patients Hastening Death by Voluntarily Stopping Eating and Drinking
Eva E. Bolt , and colleagues
Background Voluntary stopping of eating and drinking (VSED) is sometimes considered a feasible way to hasten death for people who suffer unbearably. This report from the Netherlands examines physicians' involvement with VSED to better understand the characteristics and motives of VSED patients and describe the duration and prevalent symptoms in the last days of life.
What This Study Found The survey of 285 family physicians revealed VSED is not uncommon in Dutch primary care and seems to be a relatively comfortable way to hasten death if sufficient palliative care is available. Specifically, the study found almost one-half of respondents had cared for a patient who hastened death by VSED, and that patients' motives to do so were both physical and psychosocial. Patients who decided to use VSED were mostly aged older than 80 years, in poor health, and dependent on others for everyday care. The median time until death was seven days, and the most common symptoms before death were pain, fatigue, cognitive decline and thirst or dry throat. Most patients electing VSED involved others for support; family physicians were involved in 62 percent of cases.
Implications
- The authors conclude that family physicians can play an important role in caring for VSED patients and their proxies by providing them with information, support and symptom management.
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- Patients Who Seek to Hasten Death by Voluntarily Stopping Eating and Drinking: A Qualitative Study
- Japanese physicians experiences of terminally ill patients voluntarily stopping eating and drinking: a national survey
- Drawing the line on physician-assisted death
- In This Issue: Generalist Care Around the World
- Voluntary Stopping of Eating and Drinking (VSED), Physician-Assisted Death (PAD), or Neither in the Last Stage of Life? Both Should be Available as a Last Resort