
Article Figures & Data
Figures
- Figure 1
Community health center director pointing to a sign in a residence entryway that indicates the names and contact information for clinical team that serves residents of the building.
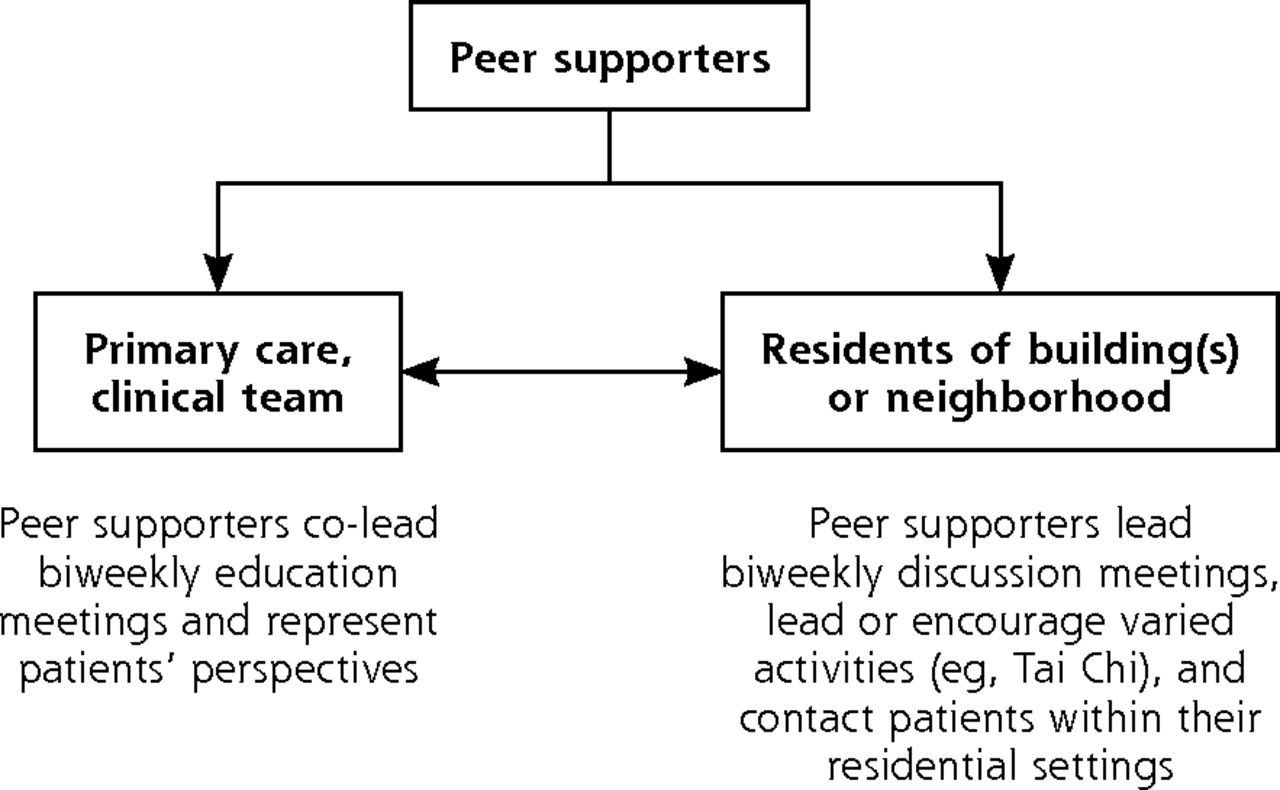
- Figure 2
Relationships among peer leaders, clinical teams, and community residents in the Peer Leader Support Program.
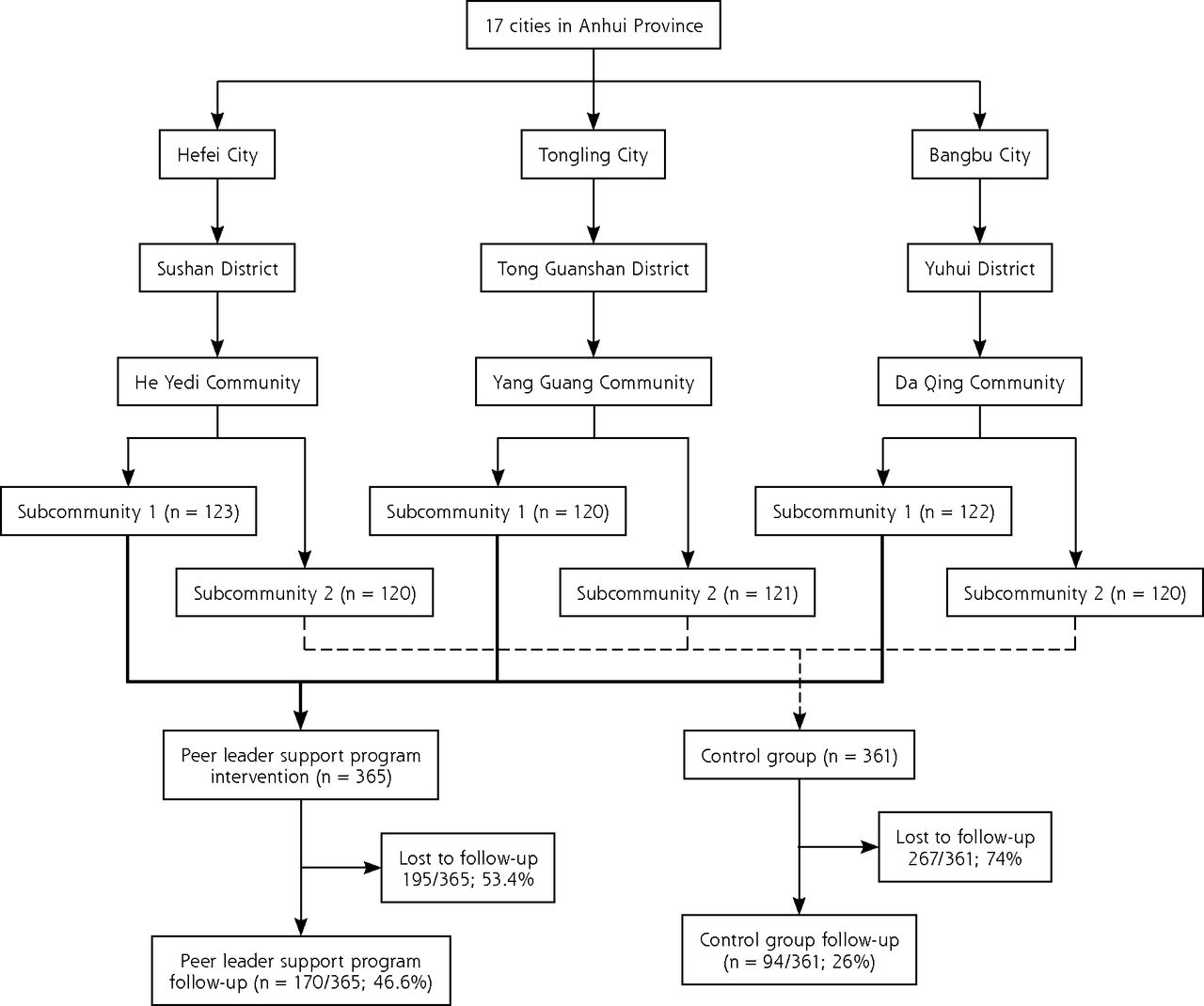
- Figure 3
Recruitment and retention of study sites and participants.



Tables
- Table 1
Observations from Participants, Peer Leaders, and Clinical Staff and Administrators Regarding Acceptability and Feasibility of the Peer Leader Support Program (PLSP)
“We will provide meeting rooms or other instrumental support if this project is implemented in our community.” (Representative of Community Neighborhood Committee) Community residents “are familiar with each other and like group activities such as Mahjong, dancing, walking and chatting…. (Representative of Community Neighborhood Committee) “Peer leaders are like the bridge to link our CHSC with patients in their served neighborhood.” (Community Health Center Director) “This is an innovative program from which we could learn new knowledge and skills. Also, it may help us to use this approach for other health issues and diseases.” (Community Health Center Director) “We hope the Anhui CDC will give us more training and direction during project implementation.” (Community Health Center Director) “This project can help us to manage our registered patients with diabetes.” (Community Health Center Station Staff Member). “We don’t have many intervention services from our CHSC.” (Patient) “If the community organized a diabetes peer support group, we would be keen to attend this group because this is beneficial for our disease and health.” (Patient) - Table 2
Average Numbers of Key Meetings and Activities and of Participants in Each PLSP Subcommunity
Category Subcommunity 1 Subcommunity 2 Subcommunity 3 Average number of biweekly educational meetings co-led by CHSC staff and peer leaders (12 by protocol) 8.78 7.73 4.24 Number of biweekly discussion meetings led by peer leaders (12 by protocol) 11.63 9.35 6.47 Number of enrollees 123 120 122 Number participants who attended ≥6 meetings 111 128 40 - Table 3
Changes in Outcome Variables Comparing PLSP and Control Participants Who Completed Follow-up
Variable PLSP (n = 135) Control (n = 94) P Values Baseline Mean (SD) Follow-up Mean (SD) Baseline Mean (SD) Follow-up Mean (SD) Baseline vs Follow-up Interaction: Condition X Time Lapse Knowledge 6.49 (2.53) 7.33 (2.82) 7.88 (2.04) 6.39 (3.24) .12 <.001 Attitudes 27.2 (6.03) 3,418 (4.87) 27.6 (4.96) 33.3 (4.52) .59 .37 Self-Efficacy 36.1 (4.27) 35.2 (3.95) 36.7 (5.52) 32.9 (4.04) .41 .002 Social support 32.5 (8.02) 31.7 (7.15) 30.4 (3.65) 30.5 (6.51) .41 .14 Self-management Diet 18.9 (1.96) 20.0 (2.36) 19.0 (1.54) 19.7 (2.11) .75 .40 Physical activity 10.2 (3.19) 10.3 (3.04) 9.7 (2.65) 10.1 (2.88) .16 .48 Glucose monitoring 3.86 (1.56) 4.13 (1.67) 5.12 (1.30) 4.86 (1.38) .35 .15 Medication adherence 3.93 (1.86) 4.04 (1.70) 4.18 (1.45) 4.39 (1.20) .047 .64 BMI (kg/m2)a 24.3 (2.88) 23.7 (2.80) 23.5 (2.50) 24.0 (2.49) .40 <.001 Systolic blood pressure 136 (14.91) 128 (11.29) 130 (11.80) 131 (14.29) .84 <.001 Diastolic blood pressure 82.5 (8.72) 79.1 (7.33) 79.0 (8.67) 78.6 (8.58) .84 .02 Fasting glucose (mmol/L) 7.68 (2.13) 6.76 (1.80) 6.38 (1.48) 6.66 (1.63) .74 <.001 Fasting glucose (mg/dL)b 138 122 115 120 2-Hour post-prandial glucose (mmol/L) 11.8 (3.54) 10.7 (3.65) 10.4 (2.05) 10.5 (3.39) .77 .02 2-Hour post-prandial glucose (mg/dL)b 212 192 187 189 PLSP = peer leader support program.
Note: The table is derived from GLM repeated measures analyses controlling for sex, age, education, family income, and community.
Description of Self-Report Measures
Knowledge: Total of 12 items: 4 concerning glucose; 3 concerning diabetic complications; 2 concerning diet; and 3 concerning insulin. Correct responses received 1 point and incorrect answers or “don’t know/unsure” received 0, yielding a range of 0 to 12. Higher scores indicate greater knowledge.
Attitudes (ie, attitudes toward self-management): 9 items scored 1 to 5 (strongly disagree to strongly agree), yielding a range of 9–45. Higher scores indicate more positive attitudes.
Self-efficacy: 9 items scored 1 to 5 (strongly disagree to strongly agree), yielding a range of 9–45. High scores indicate greater self-efficacy.
Social support (ie, perceived support for self-management): 9 items scored 1 to 5 (never to always), yielding range of 9–45. High scores indicate greater perceived support. Self-management: 9 items, scored 1 to 5, resulting in subscores for diet (4 items, with a range of 4 to 20), physical activity (2 items, with a range of 2 to 10), glucose monitoring (2 items, with a range of 2 to 10), medication adherence (1 item, with a range of 1 to 5).22 Higher scores indicate better self-management practices.
↵a For groups of Chinese origin, BMI values of 24.0 kg/m2 for men and 23.0 kg/m2 for women have been recommended as cut-offs for obesity.23
↵b Glucose levels in mg/dL are conversions from means expressed as mmol/L.
- Table 4
Observations of Participants, Peer Leaders, and Clinical Staff and Administrators Regarding Implementation and Emergent Features of the Peer Leader Support Program (PLSP)
Facilitating factors for the Community Health Support Centers (CHSC) A CHSC director indicated that peer leaders can help CHSC staff implement primary care more effectively, for example through group monitoring and care, with peer leaders helping to invite patients to attend. Instead of telephoning patients individually, peer leaders can contact them in groups and through their neighborhoods. CHSC staff suggested developing an ongoing network from the provincial level to community levels to facilitate program implementation, requiring that patients with diabetes receive diabetes self-management education, and improving PLSP outcomes through implementation over a longer time. Barriers for CHSCs Limited time and human resources, system coordination, and external locus; “We worry a little bit that the program may bring a large work burden for us.” (Community Health Center Station Staff Member) Although required to provide public health services, CHSCs tended to focus on fee-producing clinical services, while public health services depended largely on local government. Facilitating factors for peer leaders Instrumental support for peer leaders through collaboration with CHCS staff: “We contacted CHSC staff and professionals more frequently…. I have more close ties with CHSC staff. If we want them to help us, they always can do that.” Confidence: Training, discussions, and participation in the PLSP had increased diabetes knowledge, skills for diabetes self-management, and confidence in leading group meetings/activities. Sense of importance: PLSP meetings and activities were viewed as the best ways for those with diabetes to help each other. Peer leaders felt pride that they were able to meet needs, provide help, and be valuable to others and their communities. Barriers for peer leaders Need for modest financial support for materials (eg, table tennis balls), transportation, or refreshments. Limited ability to promote diabetes management; “I would like to have more time training.” (Peer Leader) “I would like to have a chance to learn from others. Could the CHSC organize us to visit another community to learn from them?” (Peer Leader) Facilitating factors for participants Most participants expressed positive views of group meetings and activities and valued the openness of their implementation, such as by being told in advance of topics to be discussed. Barriers for participants Reasons cited for not attending group meetings or activities included weather, family matters, inconvenient or non-preferred meeting times, and planned topics of little interest. Practical, specific support provided by peer leaders “…it is difficult to get up in the morning to do exercise. My peer leader had a phone call in the morning for weeks and waited for me under my building to get me doing morning exercise. Then I could get up every morning to do exercise with the group.” (Participant) “I often forgot the date to get my blood sugar checked free by the CHSC. My peer leader always gave me a call to mention that I needed to go to CHSC for a routine check the next day. If I still forgot, he would call me again to ask me to come to the CHSC for a check.” (Participant) Emergence of emotional support “The peer support group is like our ‘second home’ in which you can say what you want to say, without worry about misunderstanding and discrimination.” (Participant) “We could easily talk with peer leaders and peer group members when we felt unhappy, and we didn’t want to talk with our children because we didn’t want to burden them.” (Participant) Dissemination of the PLSP model CHSC leaders saw peer support as an innovative strategy for addressing needs other than diabetes management: “The peer support approach is a good method to help manage chronic disease, not only for diabetes…. I am preparing to set up peer groups to target hypertension patients.” (CHSC Director)
Supplemental Appendixes
Supplemental Appendixes
Files in this Data Supplement:
- Supplemental data: Appendixes - PDF file




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Pre-diabetes virtual health management community (VHMC) intervention and group interaction management model in China: a randomised clinical trial protocol
- Effectiveness of a clinic-based randomized controlled intervention for type 2 diabetes management: an innovative model of intensified diabetes management in Mainland China (C-IDM study)
- Key Features Of Peer Support In Chronic Disease Prevention And Management