
Article Figures & Data
Figures
- Figure 1
Patient experience of the conversation group medical visit.
Note: Data are drawn from an evaluation that patients completed to assess their levels of agreement with 4 statements concerning acceptability of the Conversation Group Medical Visit. The evaluation used a 5-point Likert scale. (n = 29; 2 patients did not complete evaluations.)
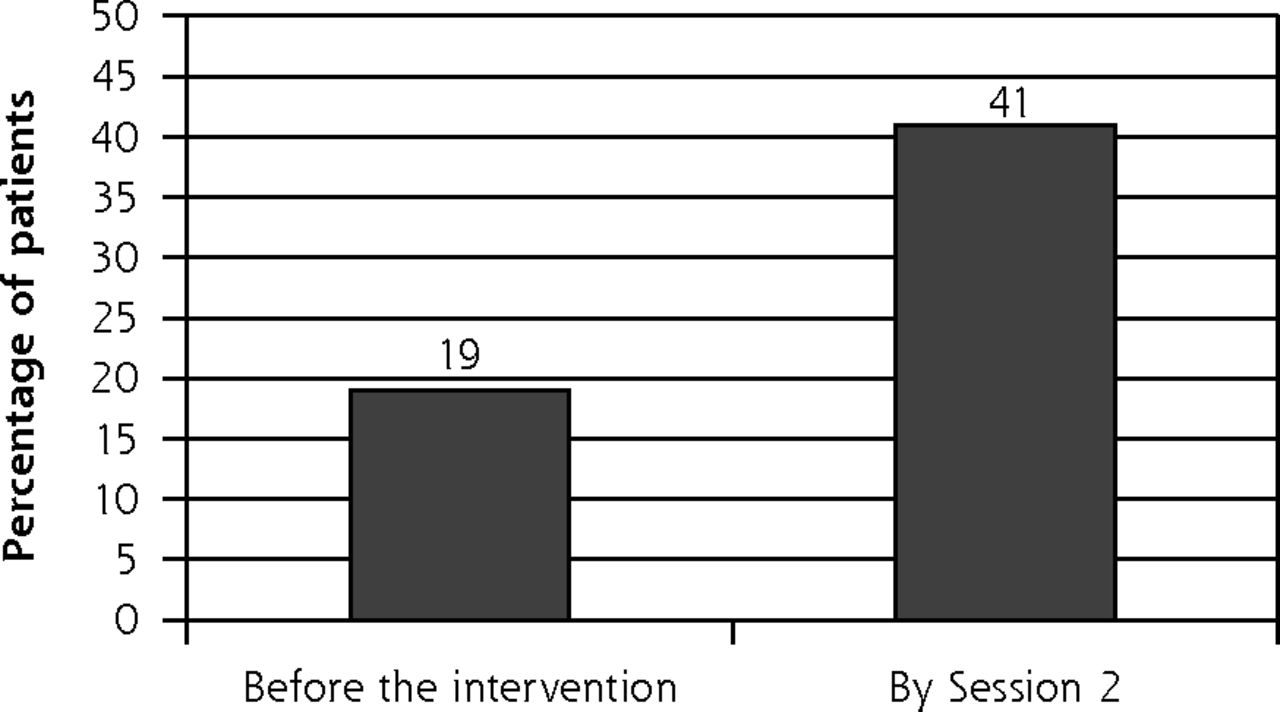
- Figure 2
Patient engagement in advance care planning conversations.
Note: During Session 1 and after participating in Session 2, patients were asked if they had had an advance care planning conversation. Bars represent the percentage of patients who answered, “Yes. The conversations included enough details that I feel confident my loved ones know my wishes.” (P = .02)

Tables
Structural Element Content Overview Sessions Two sessions, 1 month apart Patients Goal of 8 to 12 patients per cohort Practice setting A practice able to coordinate group medical visit processes as a clinical team. Location Clinic conference room Optional resources Patient handouts; video projector; white erase board; water Facilitator considerations Facilitators need to represent 2 disciplines (physician and social worker).
One needs to be a physician, physician assistant or advanced practice nurse able to bill for the medical visit.
Facilitators must be able to facilitate a group and engage patients in behavior change.
Facilitators must be knowledgeable in advance care planning.Group visit session format 2-hour sessions formatted as follows:
Arrival, check-in, medical update (30 minutes)
Introductions and rapport building (20 minutes)
Advance care planning discussion using a communication guide and decision aids (60 minutes)
Individual goal-setting (10 minutes)
Optional: Workshop time to complete advance directives
Optional: Individual clinical visits (10 minutes)Documentation and billing Document any individual evaluation and management services provided (typically CPT code 99213).
Update record with surrogate decision maker(s), care preferences, advance directives, medical orders for scope of treatment, code status preference as needed.
Communicate advance care planning preferences with primary care provider.CPT = Current procedural terminology.
Topic Examples of Facilitator Questions and Sample Prompts Session 1 Introduction Today’s goals are to talk about what’s important to you for your future health care choices and advance care planning. As we start, can you introduce yourself and share why you chose to come today? Share advance care planning experiences Have you started thinking about what is most important to you? Have you or someone close to you had experiences with serious illness or death? Consider personal values Referring to the Conversation Starter Kit, “Consider ‘what matters to me is…’ and ‘what matters to me at the end of life is…’. What do these questions bring up for you?”20
What do you worry about concerning your health in the future?Choose a surrogate decision maker(s) Who would be a good decision maker? Do you have a medical durable power of attorney? Have you talked with him or her? Goal-setting Based on today’s discussion, what goal do you have for between now and next session? [Suggest identifying a surrogate decision maker.] Session 2 Review individual advance care planning goals What was your goal regarding advance care planning or having a conversation, and how did it go? Consider flexibility in decision making Let’s watch videos from the PREPARE website.24 This is about how much flexibility you want a decision-maker to have. Do you want him or her to have total flexibility, some flexibility, or no flexibility? Consider future health care choices Have you thought about the kind of care you would or would not want to receive if you became very sick?24 How much are you willing to go through if it means you might have more time? Plan for conversations with health care professionals How much does your primary care provider know about what’s important to you? What questions do you need to ask him or her? Goal setting What are your next steps regarding advance care planning? [Suggest talking with a clinician.] - Table 3
Characteristics of Conversation Group Medical Visit Participants Compared With Patients Who Were Approached But Did Not Participate
Characteristic Participated(n = 32) Did Not Participate (n = 48) Age, mean (SD), y 79 (5.3) 78 (6.8) Women, No. (%) 19 (59) 34 (71) Race, No. (%) Native American 1 (3.1) N/A Hispanic or Latino 1 (3.1) Black or African American 7 (22) White (non-Latino) 23 (72) Relationship status, No. (%) Married or with partner 16 (50) N/A Widowed 9 (28) Divorced or separated 4 (13) Single 2 (6.3) Self-reported health status,a No. (%) Excellent or very good 13 (42) N/A Good, fair, or poor 13 (42) Caregiver for another person, No. (%) 7 (23) N/A Attended with a partner, No. (%) 10 (31) N/A Type of insurance,b No. (%) Medicare 32 (100) 45 (94) Medicare supplement 14 (44) 21 (44) Tricare 17 (53) 19 (40) Medicaid 4 (13) 4 (8.0) Education, No. (%) Less than high school graduate 1 (3.1) N/A High school graduate/GED 3 (9.4) Some college 7 (22) College graduate 7 (22) Any postgraduate or professional 10 (31) Living situation, No. (%) Home or apartment 27 (84) N/A Independent living community 3 (9.4) Referral Source, No. (%) Referred by primary care clinician 26 (81) 43 (90) Self-referred 3 (9.4) 0 (0) Referred by partner or friend 3 (9.4) 5 (11) Reason for not participating, No. (%) Interested, but at a future date N/A 2 (4.2) Declinedc N/A 30 (63) Unable to reach N/A 3 (6.3) Scheduled but cancelled or no show N/A 13 (27) Topic Quotation Advance directives Advance directives are not something done once in your lifetime…. Your health changes. Your circumstances. You age. They don’t have to be something that is done only once. Artificial nutrition and hydration The main thing is to keep people comfortable. Keep them out of pain. But without eating, without food, isn’t there pain? If they don’t feed you intravenously? Cardiopulmonary resuscitation On CPR, one of the things was busted ribs…. There were several other negative aspects of getting CPR. Dementia I have a new dilemma since my wife has dementia. We both have signed Do Not Resuscitate. The question is should we also sign a Do Not Prolong Life statement? For instance, if she gets a urinary tract infection, should they give her antibiotics? Emergency care Let me ask you about the practicality of things. Let’s say you have documents but you have an emergency at home and the ambulance comes and takes you to the nearest hospital. Well, they don’t have that document. Hospice care I’m thinking of my mother, who told me in May…. She said ‘I’m ready to go. I’ve done everything in my life I want to do.’ It chokes me up when I heard this. And she was 93. She wasn’t in any pain…. And she had hospice, which she had agreed to earlier.
Can you explain Hospice to me? We have a friend that has cancer and he’s getting that, and I just don’t know that much about it.Life sustaining treatment Is there a significant number who have declared I do not want life support and then changed their mind at the last moment? Long-term care I’ll finish this sentence: What matters to me at the end of life is… I’ve had some experience. I just put down no Nursing Home. Because I had an experience of two months with assisted living and then I had two months in rehab…. And so I indicated in my own family that it is really the last place I want to be. Organ donation As you approach our age, are there any organs that are still desirable? Palliative care I think we tend to agree that at this stage we would basically go with palliative care… to make sure she is comfortable. CPR = cardiopulmonary resuscitation.
The Article in Brief
Advance Care Planning Meets Group Medical Visits: The Feasibility of Promoting Conversations
Hillary D. Lum , and colleagues
Background Primary care needs new models to facilitate advance care planning conversations. This study describes a pilot demonstration of a group visit for advance care planning that engages patients in detailed conversations by providing a safe and supportive environment.
What This Study Found Group visits offer a feasible approach for facilitating discussions about advance care planning. Most participants evaluated the group visit as better than usual clinic visits for discussing advance care planning. After two 90-minute sessions, patients reported increases in detailed advance planning conversations. Participants were willing to share personal values and challenges related to advance care planning and initiated discussions about a broad range of related topics.
Implications
- The authors conclude the model warrants further evaluation for effectiveness in improving advance care planning outcomes for patients, clinicians and the health care system.
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Advance care planning in COPD: guidance development for healthcare professionals
- Clinician Perspectives on Group Visits for Advance Care Planning Among Caregivers and Older Adult Patients With Heart Failure
- Feasibility of Group Visits for Advance Care Planning Among Patients with Heart Failure and Their Caregivers
- Effect of an Interactive Website to Engage Patients in Advance Care Planning in Outpatient Settings
- Barriers, enablers and initiatives for uptake of advance care planning in general practice: a systematic review and critical interpretive synthesis
- CPR decision-making conversations in the UK: an integrative review
- A Group Visit Initiative Improves Advance Care Planning Documentation among Older Adults in Primary Care
- In This Issue: Confronting Constraints on Individual Behavior & Outcomes