
Abstract
Collaborative visit agenda setting between patient and doctor is recommended. We assessed the feasibility, acceptability, and utility of patients attending a large primary care safety-net clinic typing their agendas into the electronic visit note before seeing their clinicians. One hundred and one patients and their 28 clinicians completed post-visit surveys. Patients and clinicians agreed that the agendas improved patient-clinician communication (patients 79%, clinician 74%), and wanted to continue having patients type agendas in the future (73%, 82%). Enabling patients to type visit agendas may enhance care by engaging patients and giving clinicians an efficient way to prioritize patients’ concerns.
INTRODUCTION
Collaborative agenda setting is a communication skill that helps patients identify concerns early in the clinic visit,1,2 possibly diminishing the number of “Oh, by the way” items at the end of visits,3 and increasing patient satisfaction.4 Agenda setting, however, is often limited by time constraints.4
Electronic medical records (EMRs) offer patients access to their medical data, including doctors’ notes,5 and have the capability to facilitate increased patient involvement in their health care and also contribute to their health data. OpenNotes is a national initiative, not a software program, that invites patients to review their visit notes written by their doctors, nurses, or other clinicians. Existing OpenNotes research shows enthusiasm among both patients and clinicians,6 but this is the first Open-Notes study of cogeneration of clinic notes.
Allowing patients to type their agenda into their clinic note before a visit may facilitate communication of health concerns. This article reports a pilot study of feasibility and patient and clinician perceptions of patient-typed visit agendas among a vulnerable patient population at a safety-net clinic.
METHODS
This study was approved by the University of Washington Institutional Review Board. All patients and clinicians provided informed consent.
Study Population
Harborview Medical Center (HMC) is a safety-net county hospital in Seattle, Washington caring for the region’s most vulnerable patients. We recruited patients and clinicians between June 9 and July 22, 2015 from the HMC Adult Medicine Clinic, a 67-clinician (attending physicians, residents, and advanced practice registered nurses) primary care clinic serving approximately 5,000 patients annually.
We invited a convenience sample of primary care clinicians present in clinic when the research assistant (M.A.) was available. Participating clinicians’ patients were recruited via telephone the night before their appointment and asked to arrive 30 minutes early or were approached by the receptionist if they had not been reached by phone but still arrived early. Patients younger than 18 years of age, unable to read or write in English, or uncomfortable typing on a computer were ineligible. The research assistant met patients in the waiting room, provided them with a laptop computer with the clinic’s EMR interface, and let them type their agenda. The patient typed the agenda in the clinician’s “progress notes” field under the research assistant’s name with the heading, “The following was typed by the patient as part of a pilot study on patient written visit agendas.” Participating clinicians reviewed the agenda before or upon entering the patient’s exam room, and the patient’s agenda remained in the notes section of the permanent visit record, adjacent to the physician’s note, in the EMR. Patients and clinicians were offered gift cards ($10 and $20, respectively) to participate and were surveyed after the visit about their experiences.
Patient and Clinician Surveys
The patient survey queried demographic characteristics, self-reported health, and perceptions of the experience, using a 5-point Likert scale (strongly disagree, disagree, neutral, agree, strongly agree). Clinicians completed a brief survey after each visit asking if the agenda: (1) gave them an improved understanding of the patient’s health concerns, and (2) was helpful. Clinicians completed an additional survey at the study’s conclusion soliciting age, sex, role in clinic, and perceptions of agendas that mirrored the patient survey. The research assistant also collected time spent typing agendas, number of words typed, and the clinician’s billed visit diagnoses and level of service. Surveys are available in the Supplemental Appendix, available at http://www.AnnFamMed.org/content/15/2/158/suppl/DC1/.
Data Analysis
Descriptive statistics characterized patient and clinician demographics and perceptions of the agendas, and agenda characteristics such as length and typing time.
RESULTS
Of 209 invited patients, 26 (12%) declined and 54 (26%) were not eligible. Ineligible patients included 35 uncomfortable typing on a computer, 9 who could not read or write in English, and 10 with difficulty both typing and reading/writing. Of the 129 remaining patients, 17 did not come to their appointment or arrived late, 112 typed an agenda, and 11 left before the post-visit survey, leaving 101 patient participants.
Characteristics of this convenience sample (Table 1) are relatively representative of this clinic’s patients, and age and diagnoses were not statistically different between those who participated and those who chose not to participate (data not shown). Agendas were brief; 83% of patients typed for <10 minutes, and 80% typed <60 words. Table 2 shows an example patient-typed agenda and responses from the patient and clinician follow-up surveys.
Characteristics of Patients, Clinicians, and Visit Agendas
Example of a Patient-Typed Agenda and Clinician Comment; Examples of Patients’ and Clinicians’ Responses from the Follow-Up Survey
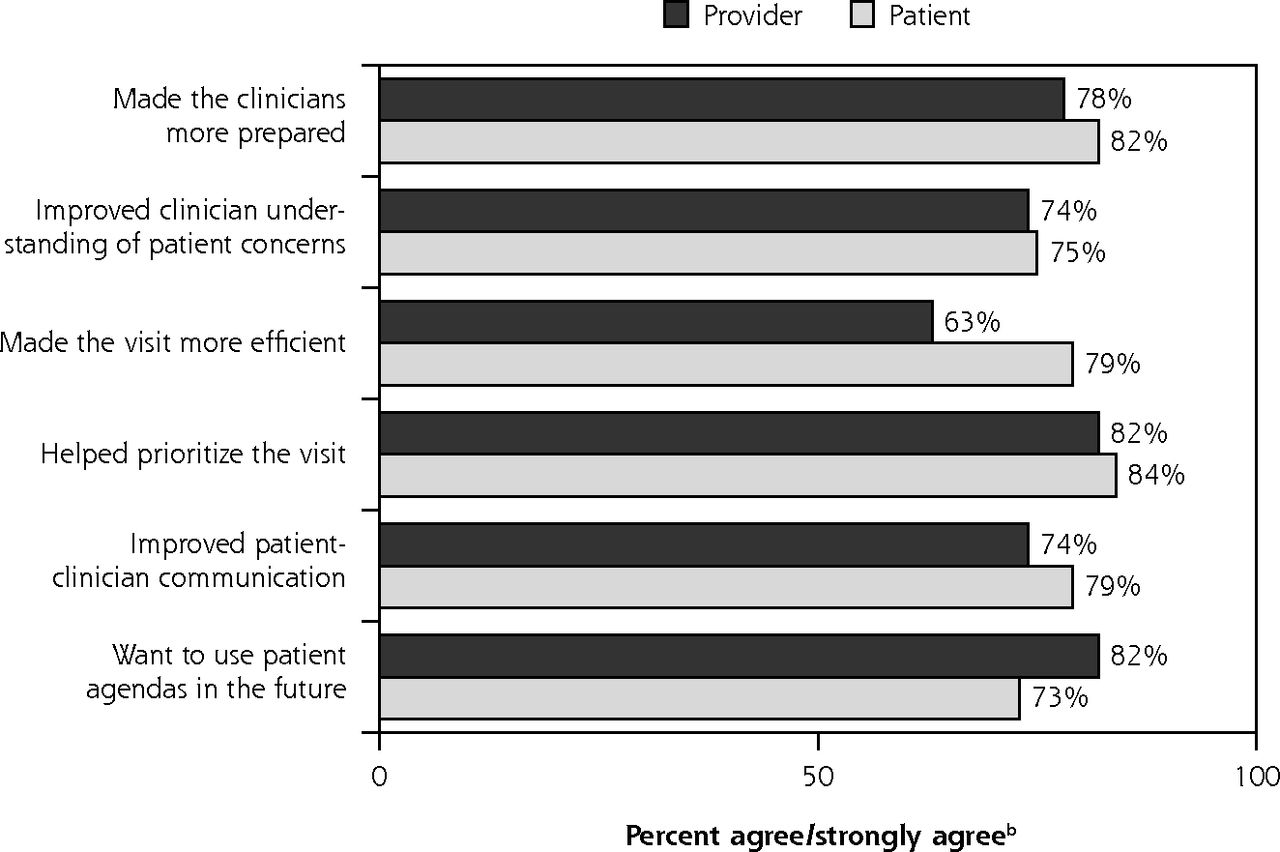
Agenda perceptions were strongly positive among both patients and clinicians (Figure 1).
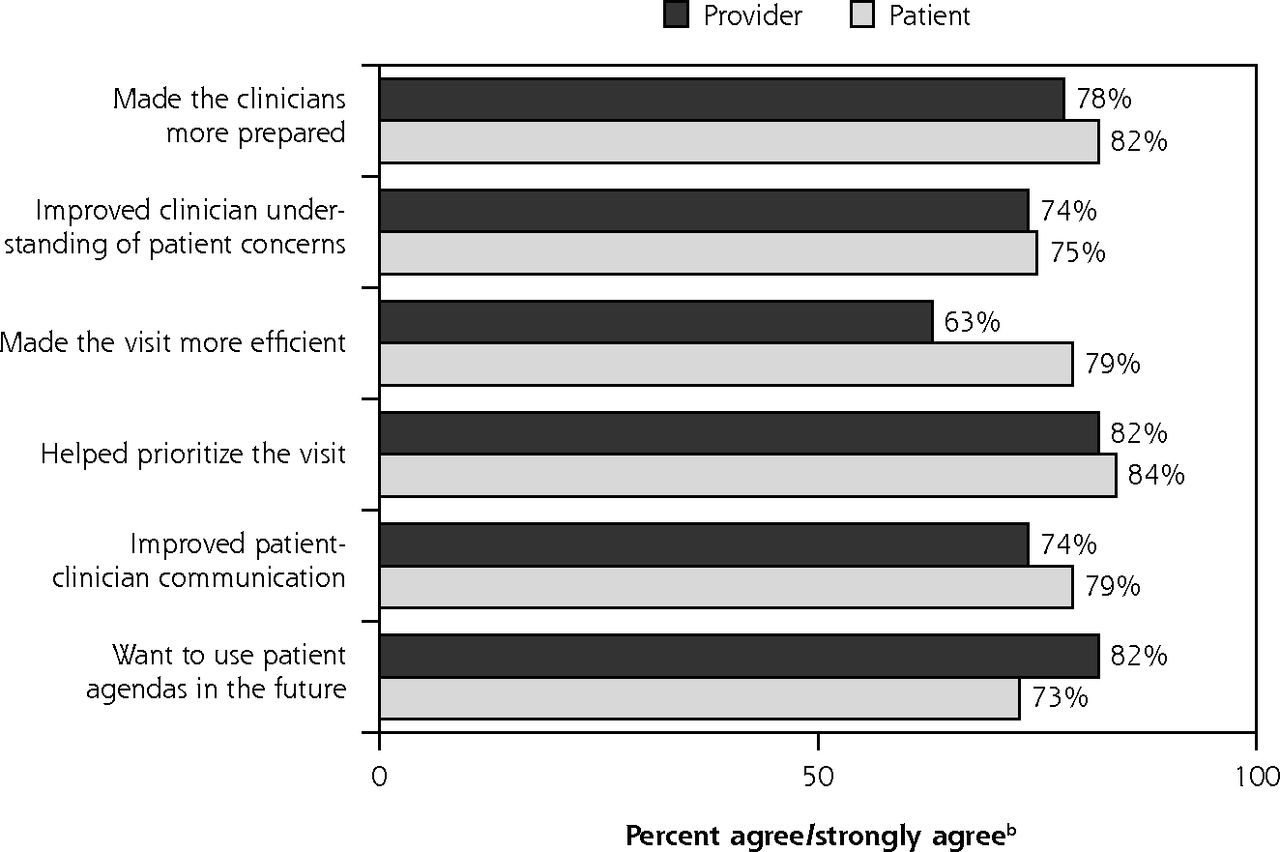
Patient (N = 101) and clinician (N = 27) perceptions of patient-written agendas.a
aSurvey items for patients: “Because of writing my visit agenda, my doctor: (1) seemed more prepared for my visit than usual, (2) Had a better understanding of my health concerns than usual”; “Writing my visit agenda: (1) made this visit more efficient, (2) helped me prioritize my health concerns, (3) improved communication between me and my doctor”; “I would like to type the reasons for my visit before my appointments in the future.”
Survey items for clinicians: “When my patients typed their visit agenda, this: (1) made me better prepared for my patients’ visits than usual, (2) helped me prioritize my patients’ concerns, (3) helped me utilize my time more efficiently during my appointments, (4) improved communication with my patients”; “Overall, I would like for my patients to type visit agendas in the future.”
bLikert scale responses were collapsed into binary categories (“agree” + “strongly agree” = “yes”) to simplify presentation.
DISCUSSION
Patients attending a safety-net primary care clinic were interested and able to type their agenda into the EMR visit note. Patients and clinicians felt this improved communication and both expressed interest in patient-written agendas in the future. In this diverse population of patients with complex medical conditions, 28% employment, and 32% high school or less education, nearly two-thirds of the patients approached were not limited by lack of English or computer literacy and participated.
Clinicians often cite inadequate visit time as a barrier to relationship development and communication with patients.2,7 Interacting with EMRs during patient interviews has also eroded clinicians’ ability to connect with patients8 and led to clinician dissatisfaction with clinical practice, particularly in primary care.9 This pilot study suggests a possible way for the EMR to offset the time and computer barriers to communication. By allowing patients to set agendas before appointments, patients and clinicians can optimize their time together.
The Patient Protection and Affordable Care Act identifies patient activation and engagement as key components of accountable care organizations and patient-centered medical homes.10 A few studies have addressed electronic portals and patient activation with promising initial results.11,12 In the original OpenNotes study, 59% to 62% of patients believed they should be able to comment on their clinic notes.6 In our current study, patients accepted the opportunity to directly contribute to their visit notes by typing their visit agendas. Future studies could evaluate the relationships between agenda setting and other contributions to notes, and patient engagement.
This pilot study was limited to a small convenience sample at a single clinic with no comparison group, and the results may not be generalizable to other settings. We provided financial incentives for participants, and a research assistant facilitated the agenda typing process. This study involved a vulnerable patient population; it is also important to note that of those approached, 12% declined and 26% were not eligible because they could not type or write in English. Though not available in this study, patient navigators, peer coaches, translators, or audio and touch-screen technologies may be able to address limitations in English or computer literacy, or low vision, hearing, or comprehension. Nevertheless, approximately one-half of our target patients completed the intervention and both patients and clinicians found agenda setting worthwhile.
The patient cogeneration of visit notes, facilitated by new EMR functionality, reflects a shift in the authorship and “ownership” of visit notes. Patient-written visit agendas could increase the collaborative nature of the clinical encounter between patient and clinician, but require further study, including measurement of patient engagement and health outcomes.
Acknowledgments
The authors gratefully acknowledge support from The Commonwealth Fund, Robert Wood Johnson Foundation, Gordon and Betty Moore Foundation, Peterson Center on Healthcare, and Cambia Health Foundation, the National Cancer Institute (K05 CA104699; J.E.), and the University of Washington School of Medicine Medical Student Research Training Program (M.A.).
Footnotes
Conflicts of interest: authors report none.
Previous presentation: These results were presented at the Society of General Internal Medicine (SGIM) annual conference; May 11–14, 2016; Hollywood, Florida.
Supplementary materials: Available at http://www.AnnFamMed.org/content/15/2/158/suppl/DC1/
- Received for publication June 21, 2016.
- Revision received September 28, 2016.
- Accepted for publication October 10, 2016.
- © 2017 Annals of Family Medicine, Inc.
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- Patient and family contributions to improve the diagnostic process through the OurDX electronic health record tool: a mixed method analysis
- Filling a gap in safety metrics: development of a patient-centred framework to identify and categorise patient-reported breakdowns related to the diagnostic process in ambulatory care
- In This Issue: On-the-Ground Advances & High-Level Influences