
Abstract
PURPOSE Although evidence exists for the efficacy of psychosocial interventions to prevent the onset of depression, little is known about its prevention in primary care. We aimed to evaluate the effectiveness of psychological and educational interventions to prevent depression in primary care.
METHODS We conducted a systematic review and meta-analysis of relevant randomized controlled trials (RCTs) examining the effect of psychological and educational interventions to prevent depression in nondepressed primary care attendees. We searched MEDLINE, PsycINFO, Web of Science, OpenGrey Repository, Cochrane Central Register of Controlled Trials, and other sources up to May 2016. At least 2 reviewers independently evaluated the eligibility criteria, extracted data, and assessed the risk of bias. We calculated standardized mean differences (SMD) using random-effects models.
RESULTS We selected 14 studies (7,365 patients) that met the inclusion criteria, 13 of which were valid to perform a meta-analysis. Most of the interventions had a cognitive-behavioral orientation, and in only 4 RCTs were the intervention clinicians primary care staff. The pooled SMD was −0.163 (95%CI, −0.256 to −0.070; P = .001). The risk of bias and the heterogeneity (I2 = 20.6%) were low, and there was no evidence of publication bias. Meta-regression detected no association between SMD and follow-up times or SMD and risk of bias. Subgroup analysis suggested greater effectiveness when the RCTs used care as usual as the comparator compared with those using placebo.
CONCLUSIONS Psychological and educational interventions to prevent depression had a modest though statistically significant preventive effect in primary care. Further RCTs using placebo or active comparators are needed.
- depression/prevention & control
- delivery of health care
- primary health care
- systematic review
- meta-analysis
- psychological interventions
- educational interventions
INTRODUCTION
According to the World Health Organization, major depressive disorder affects about 350 million people worldwide.1 An international study found the average 12-month prevalence of major depression to be 5%.2 In primary care, though, this figure is higher (11%).3 About 60% to 70% of patients with acute depression experience suicidal ideas, with the actual incidence of suicide in depressive patients being 10% to 15%.4 Patients with a specific physical illness who develop depression have an excess mortality of 52%.5 In terms of global disease burden measured in disability-adjusted life years, major depressive disorder increased by 37% between 1990 and 20106 and is projected to become the single leading cause of disease burden by 2030 in high-income countries.7
Two ways exist to reduce the disease burden of depression: treatment and prevention of new cases. Despite effective treatments for depression, the disease burden of depression can be reduced by only 20%; not all cases are recognized, and when recognized, not all patients receive appropriate therapy or adhere to treatment.8
In recent decades interest in prevention has grown,9 and it is now a key objective in the strategic plan of the National Institute of Mental Health (NIMH).10 Hundreds of randomized controlled trials (RCTs) designed to prevent depression, as well as dozens of systematic reviews, have been undertaken on this topic.11–22 Most RCTs to prevent depression examined interventions with a cognitive-behavioral orientation. Additionally, more than 70% of RCTs to prevent depression have been conducted in children and adolescents, and only 24% of RCTs to prevent depression lasted longer than 12 months of follow-up.23 Although interventions to prevent depression are beneficial, their effect sizes are small,23,24 and no conclusive data exist on the superiority of any particular intervention.24
Primary health care services are the ideal setting in which to undertake disease prevention strategies for many illnesses, including depression.25 At the patient level, many people at risk of depression are seen in general practice. At the population level, primary care serves defined communities, so that prevention can be population based. Although some trials for primary prevention of depression in primary care have been undertaken, no systematic review or meta-analysis of these trials has yet been conducted.
Our objective was to evaluate the effectiveness of psychological and educational interventions to prevent depression in primary care.
METHODS
We followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines.26 The protocol was registered in the International Prospective Register of Systematic Reviews (PROSPERO, registration number: CRD42014006067).
Search Strategies and Screening Procedures
We searched MEDLINE (via PubMed), PsycINFO, Embase, Web of Science (WOS), OpenGrey Repository (System for Information on Grey Literature in Europe), and Cochrane Central Register of Controlled Trials (CENTRAL) from inception to May 2016 without restrictions. The last search was on May 27, 2016. We reviewed the reference lists of relevant meta-analyses and reviews,11–24 as well as retrieved articles, to find additional publications. We also contacted experts in the field to identify other pertinent articles.
The search strategy included the following terms: “randomized controlled trial,” “depressive disorder,” “prevention,” “primary health care,” and “intervention.” Search results were restricted by the term “randomized controlled trial.” The search strategy was developed first in MEDLINE (via PubMed) and later adapted to all databases (Supplemental Appendix, available at http://www.annfammed.org/content/15/3/262/suppl/DC1).
Selection Criteria
Studies had to meet specific inclusion and exclusion criteria (Table 1).
Inclusion and Exclusion Criteria for Included Studies
We selected RCTs because they provide more evidence on causality and are considered a reference standard for clinical trials.27 We included all primary care patients, excluding those with depression at baseline, which allowed us to separate the effectiveness of prevention from that of treatment. We focused on psychological and educational interventions because they share the same mechanism of action, facilitating changes in attitudes and behavior, and because most interventions to prevent depression are of this type.28 All languages were considered.
Study Selection
The entire selection process was reviewed independently by the first 2 authors (S.C.C. and P.M.P.). In the event of disagreement, a third author (J.A.B.) was consulted. The degree of agreement between the first 2 authors was excellent (κ= 0.78; 95% CI, 0.59–0.98).29,30
Data Extraction
Data were independently extracted by the 3 reviewing authors using a purposefully designed data extraction form. Discrepancies between the reviewers were reconciled by consensus. Wherever necessary, the reviewers contacted the authors of published articles to obtain missing data.
Risk of Bias
We assessed methodological quality using the Cochrane Collaboration risk of bias tool.31 This tool measures the quality of RCTs through 6 criteria: random sequence generation, allocation concealment, blinding of participants and clinicians, blinding of outcome assessment, incomplete outcome data, and selective reporting. All assessments of risk of bias were performed independently by 2 authors (S.C.C. and P.M.P.) and discrepancies were resolved by consensus between them. There was excellent inter-researcher agreement (intraclass correlation coefficient = 0.85; 95% CI, 0.74–0.92).32
Statistical Analysis
We used Comprehensive Meta-Analysis Software, version 3.0 (Biostat, Inc) for all analyses.
We used standardized mean difference (SMD) as effect size because most RCTs included in our meta-analysis assessed differences in depressive symptoms. For each study, we first calculated the SMD by combining the SMD at different follow-up times into a single estimate as average. We then calculated the pooled SMD of all RCTs, as well as its 95% CI. Cohen proposed the following interpretation for this effect size: 0.2 small; 0.5 medium, and 0.8 large.33 Negative SMDs indicated a better outcome (reduction of depressive symptoms) in the intervention group. The random-effects model assumes that the included studies are drawn from populations that may differ and we believed this model was more appropriate to our study.31 We conducted all analyses using both fixed-and random-effects models.
As a test of heterogeneity of effect sizes, we estimated the I2 statistic, which can be expressed as a percentage, where a value of 0% indicates no heterogeneity, and 25%, 50%, and 75% can be interpreted as low, moderate, and high levels of heterogeneity, respectively.34 We also calculated the Q statistic and its P value.
Publication bias was evaluated by inspecting the funnel plot on the primary outcome measure and by Duval and Tweedie’s trim-and-fill procedure,35 which yields an estimate of the effect size after adjusting for publication bias. We also performed Begg and Mazumdar rank correlation and Egger’s test, which quantify the bias captured by the funnel plot. We calculated the Rosenthal’s fail-safe N test, which computes the number of missing studies (with SMD of 0) that would need to be added to the analysis to yield a statistically insignificant overall effect.
Because the SMD could differ at varying follow-up periods, we conducted sensitivity analyses at the first and last follow-up. We also conducted subgroup analyses according to type of prevention, country, age, comparator, clinician, intervention format, number of sessions, and sample size. Meta-regression analyses were conducted to see whether differences existed in effect sizes with time or depending on their risk of bias.
RESULTS
Search Results
A total of 35 articles were retrieved for further full-text evaluation of the inclusion criteria. Of these 35 articles, 19 were excluded (Table S1, Supplemental Appendix, available at http://www.annfammed.org/content/15/3/262/suppl/DC1), leaving a total of 14 RCTs36–50 (reported in 16 publications) that met all the inclusion criteria and that were selected. Figure 1 displays the flowchart describing the inclusion process.

Flowchart of the studies reviewed.
CENTRAL = Cochrane Central Register of Controlled Trials; WOS = Web of Science.
Characteristics of Included Studies
The 14 RCTs36–50 were published between 1993 and 2016. Six RCTs were conducted in the United States, 3 in Spain, 2 in the Netherlands, 2 in the United Kingdom and 1 in China; 9 were aimed at adults and 5 at specific populations. Concerning type of prevention, 9 evaluated the indicated prevention, 4 evaluated selective prevention, and 1 evaluated universal prevention. Overall, the RCTs evaluated a total of 7,365 participants: 4,018 in the intervention group and 3,287 in the control group; 1 RCT did not report information about the intervention and control sample size separately.50 The population size of the RCTs ranged from 29 to 3,326 (median = 169). We excluded the antidepressant arm from 3 RCTs.38,48,49
The intervention orientation was based on the principle of cognitive behavioral therapy (CBT) in 12 RCTs. The comparators in 11 RCTs were care as usual, no intervention, or waiting list.
The intervention format was delivered as individual sessions in 10 RCTs and in 4 as group sessions. The number of sessions ranged from 3 to 12 (median = 6). The interventions were delivered by primary care staff in only 4 RCTs.
Concerning outcome, 9 RCTs measured depressive symptoms, 2 measured incidence of depression, and 3 measured symptoms and incidence.
The follow-up periods varied between 7 weeks and 60 months (median = 12 months). Six RCTs reported a follow-up of greater than 12 months and 5 had a follow-up of less than 6 months. More details about the 14 RCTs included are displayed in Table 2.
Randomized Clinical Trials to Prevent Depression in Primary Care
Risk of Bias in Included Studies
Ten RCTs had a low (4 or fewer points), 1 had a moderate (5 to 6 points), and 3 had a high (7 or more points) risk of bias. Table 2 shows details about the risk of bias for each study.
Effectiveness of the Interventions to Prevent Depression
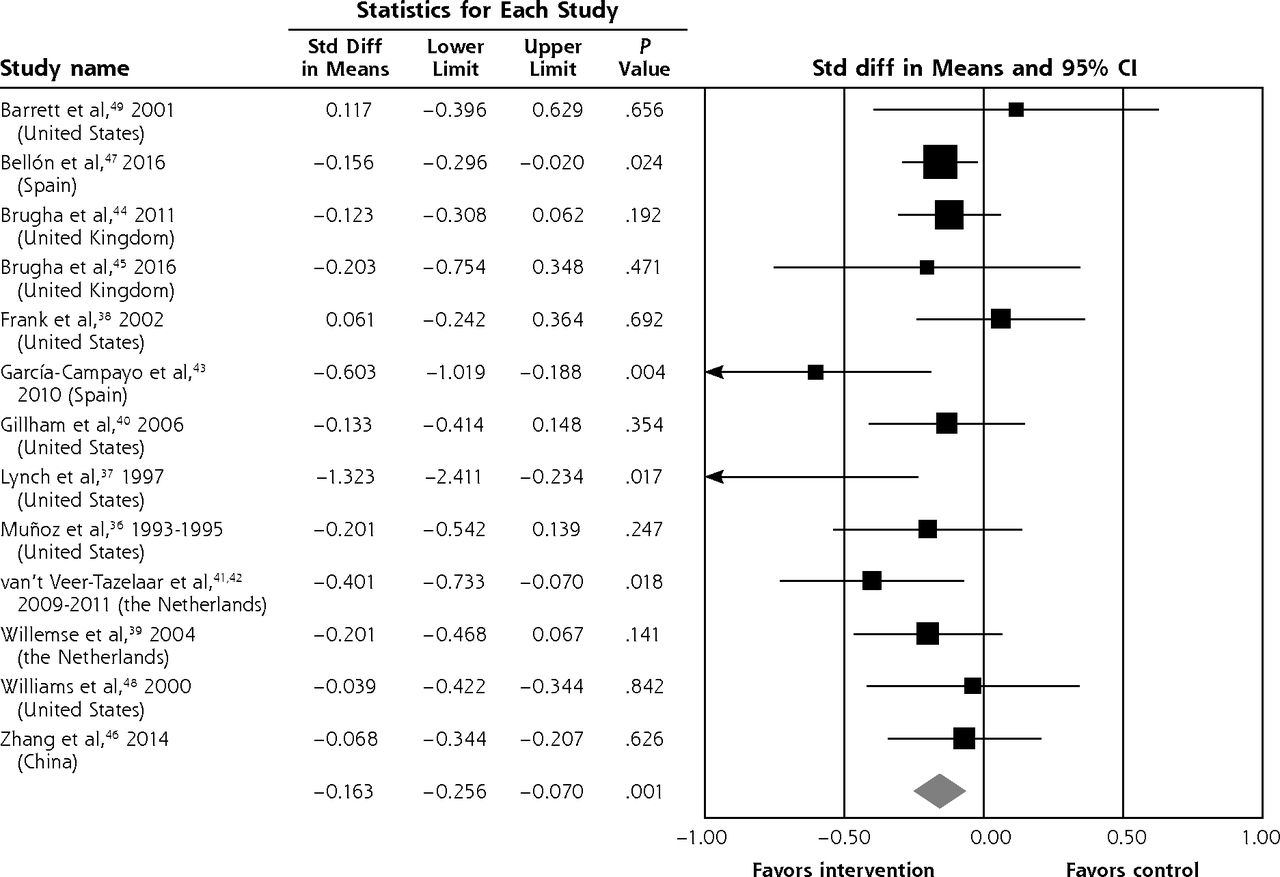
For meta-analysis calculations we used 13 RCTs because 1 RTC50 of the 14 included in the systematic review did not report the necessary data. The pooled SMD was −0.158 (95% CI, −0.234 to −0.082; P = .000) for the fixed-effects model and −0.163 (95% CI, −0.256 to −0.070; P = .001) for the random-effects model; the odds ratio (OR) of this latter effect size, transformed by the Comprehensive Meta-Analysis Software, was 0.744 (95% CI, 0.629 to 0.881; P = .001), which means that psychological and educational interventions in primary care had a small, although statistically significant, effect to prevent depression. Heterogeneity was low (I2 = 20.6%) and statistically nonsignificant (Q = 15.12; 12 df; P = 0.235). Figure 2 is a forest plot for the overall and individual effect sizes.
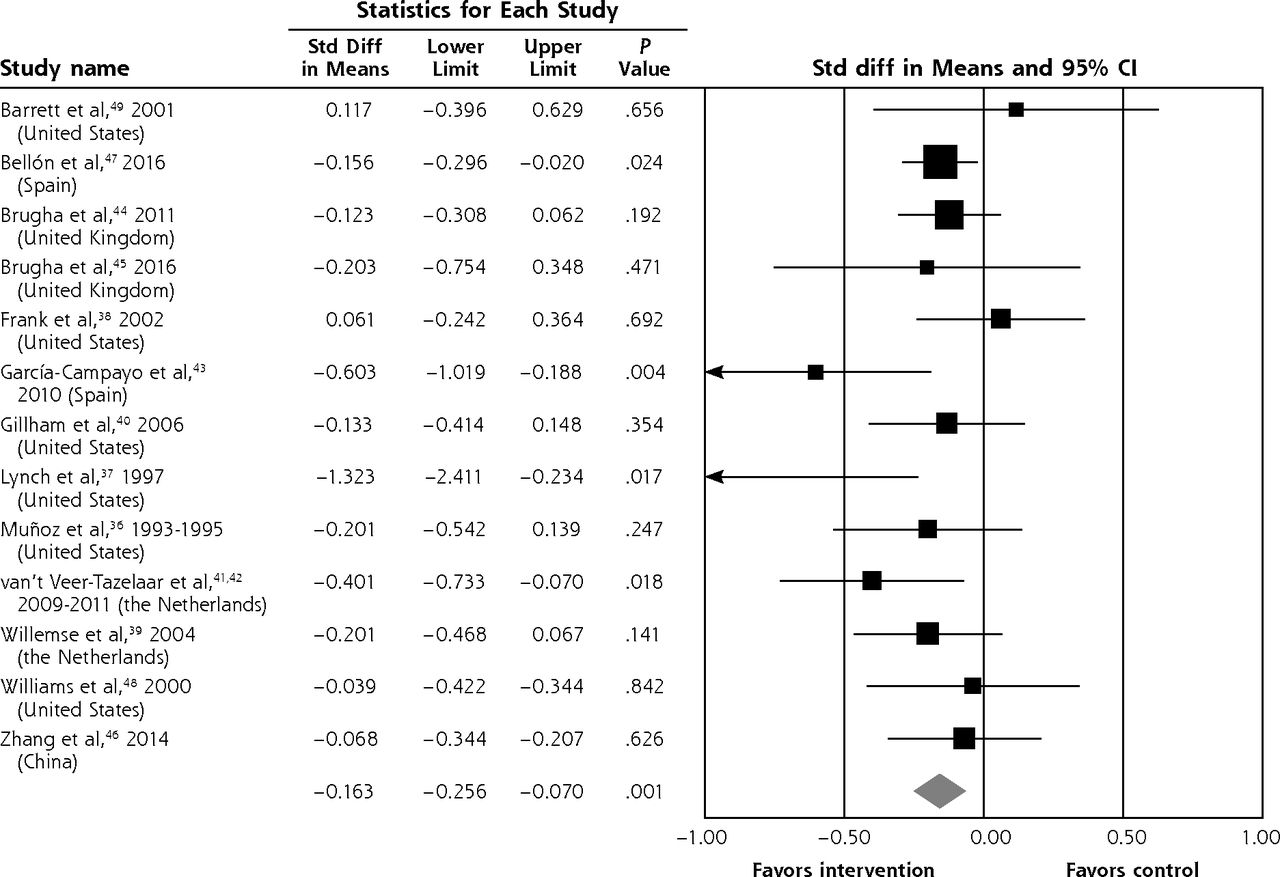
Forest plot of comparison: intervention vs control group, using a random-effects model.
Std diff = standardized difference.
Sensitivity Analyses
Because the effect sizes for the fixed- and the random-effects models were very similar, we report the results for only the random-effects model. The pooled SMD using the first evaluation over time (posttreatment) of each RCT was similar to the last evaluation (Table 3). When we excluded from the analysis the only RCT that used the reduction of depressive symptoms as a secondary outcome,43 the pilot study of Brugha,45 or both studies,43,45 the pooled SMDs were then similar (Table 3).
Analysis of the Studies Included in the Meta-Analysis of Psychological and Educational Interventions to Prevent Depression in Primary Care
Meta-Regression
The effect sizes increased with time (β = −0.0094; 95% CI, −0.0170 to −0.0018; P = .015). When the variable type of comparator was included in the equation, however, this effect was not statistically significant (β = −0.0076; 95% CI, −0.017 to .001; P = .095). There was no statistically significant association between effect size and risk of bias (β = −0.024; 95% CI, −0.083 to 0.035; P = .432), nor after adjustment for the type of comparator (β = −0.001; 95% CI, −0.059 to 0.056; P = .959).
Publication Bias
The funnel plot and Duval and Tweedie’s trim-and-fill procedure35 (Figure S1, Supplemental Appendix, available at http://www.annfammed.org/content/15/3/262/suppl/DC1) were symmetric. After adjustment for potential publication bias, the pooled SMD was −0.163 (95% CI, −0.256 to −0.070). The Egger’s test was nonsignificant (intercept = −0.841; 95% CI, −2.395 to 0.713; P = .259). The fail-safe N was 48, which means we would need to locate and include in our meta-analysis 48 studies with an SMD of 0 to reduce the pooled SMD obtained to a statistically nonsignificant level. Thus, we found no evidence of publication bias.
Subgroup Analyses
Subgroup analyses (Table 3) suggested that psychological and educational interventions to prevent depression in primary care were more effective when the comparator was care as usual or no intervention vs placebo.
DISCUSSION
We selected 14 RCTs, with a total of 7,365 nondepressed primary care attendees of different ages. Most of the 14 RCTs had a low risk of bias. In the meta-analysis we found a modest, although statistically significant, effect size for prevention of depression. The sensitivity analyses confirmed these results. We also found low heterogeneity and no evidence of publication bias. To our knowledge, this meta-analysis is the first studying the effectiveness of psychological and educational interventions to prevent depression in primary care.
We included only RCTs that excluded depression at baseline; therefore, we are sure that effectiveness for prevention, not for treatment of depression, was assessed. In primary care we obtained an effect size, SMD = −0.163 (OR = 0.74), very similar to the most recent meta-analysis of psychological interventions to prevent depression in all types of population (incidence rate ratio (IRR) = 0.79).24 Accordingly, the incidence of new episodes of depression could be reduced on average by 26% and 21% in our study and in the van Zoonen et al24 study, respectively. The effectiveness of psychological interventions to prevent depression is a robust finding,13–24 even though its effect size is small.
We only included 1 RCT40 of psychological and educational interventions in adolescents to prevent depression in primary care; when this setting restriction was not used, however, most trials were limited to children and adolescents.23
In only 4 RCTs43–45,47 were intervention clinicians primary care staff, and their pooled effect size (SMD = −0.197) was not different when compared with mental health providers (SMD = −0.141); although there were too few RCTs to draw conclusions. We excluded 1 RCT51 because the comparator was not care as usual, waiting list, or placebo; in both arms of this RCT, however, primary care physicians implemented interventions to prevent depression (motivational interviewing vs brief advice to engage adolescents with an Internet-based depression program). As compared with other types of clinicians, primary care staff may have various advantages, such as greater accessibility, closeness, knowledge of patients, and less stigma, as well as continuity of care and a comprehensive and holistic focus,52 though there may be certain drawbacks, such as the need for training and lack of time to carry out the intervention.53 A recent overview of reviews23 reported that most trials to prevent depression have been conducted by mental health specialists, to a lesser extent by educational staff (for children and adolescents), more sparsely by lay persons, and rarely by primary care professionals. Further trials with primary care staff as providers of depression interventions are needed.
Our meta-analysis included 3 RCTs38,48,49 that used placebo as the comparator, and all found the intervention not effective. These 3 RCTs contributed to reduce the pooled effect size; consequently, subgroup analysis showed a greater and statistically significant effectiveness when the RCTs used care as usual as the comparator. Similar results were found in a review of psychological and educational interventions for preventing depression in children and adolescents,16 and the placebo effect is known to be high when applied to depression.54 Future studies including more active comparators would greatly improve the strength with which conclusions can be drawn about the effectiveness of preventing depression.
The pooled effect size of the first evaluation (SMD = −0.166) was very similar to the last evaluation (SMD = −0.154), and meta-regression found no association between effect size and follow-up period. In other meta-analyses, however, the effect size of the first evaluations was greater than for the last evaluations.13,24
Interventions based on interpersonal therapy might be more effective than those based on CBT.13,24 In our study the psychological and educational interventions were mostly based on the principles of CBT, so we have no data to discuss the superiority of any particular kind of intervention. Only 1 RCT had a completely different approach to all the others.47 This RCT was implemented by primary care physicians, who measured each patient’s individual risk for developing depression, identifying in each patient specific risk factors for depression that are amenable to change. This information was then used with each patient to improve knowledge and alter behavior. This RCT was also the only one included in our study that involved universal prevention. Although the RCTs by Brugha et al44,45 could have been considered to involve universal prevention, including puerperal and pregnant women implies in itself that the intervention was applied in a high-risk population (selective prevention). In our meta-analysis, selective prevention seemed to have a greater effect (SMD = −0.236) than indicated prevention (SMD = −0.134); this difference, however, was not statistically significant, and only 4 RCTs included selective prevention.
Our study has several limitations that should be considered. First, with the use of truncation and the choice of expression for the terms in PubMed, we performed a search with less sensitivity; therefore, some potentially useful articles were not included. This loss might be minimized, however, by the search in the other 5 databases and the references of relevant previous reviews, meta-analyses, and retrieved articles. Second, the number of studies that satisfied all our inclusion criteria was relatively small (14 RCTs). Thus, there was a lack of statistical power to find differences in subgroup and meta-regression analyses. Accordingly, these results should be interpreted with caution. Third, 9 RCTs measured only depressive symptoms as outcome. Though this procedure is valid, it is less rigorous than standardized diagnostic interviews; reduction of depressive symptoms, however, also has a positive impact on quality of life and cost.55 Fourth, although 6 RCTs had follow-up periods of more than 12 months, only 4 reached 24 months or more. Another 4 RCTs had follow-up periods that were too short (11 or fewer weeks). Consequently, we are unable to draw clear conclusions about the long-term effect.
We found a modest but positive effect of psychological and educational interventions to prevent depression in primary care. According to our results, primary care managers and physicians could implement programs and interventions to prevent depression. Not enough information is available, however, about what program or intervention is more efficient in primary care.
Acknowledgments
The authors thank the Primary Care District of Malaga for their support.
Footnotes
Conflicts of interest: authors report none.
Funding support: The following institutions contributed financial support: Instituto de Salud Carlos III and the European Regional Development Fund, “Una manera de hacer Europa” (grant PI12/02755), Consejería de Salud de la Junta de Andalucía (grant PI-0583-2012), and Red de Investigación en Actividades Preventivas y Promoción de la Salud (redIAPP) (grant RD06/0018).
Supplementary materials: Available at http://www.AnnFamMed.org/content/15/3/262/suppl/DC1/.
- Received for publication May 31, 2016.
- Revision received October 22, 2016.
- Accepted for publication November 18, 2016.
- © 2017 Annals of Family Medicine, Inc.
References
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Effectiveness of complex multiple-risk lifestyle interventions in reducing symptoms of depression: a study protocol for a systematic review and meta-analysis of randomised controlled trials
- Effectiveness of online interventions in preventing depression: a protocol for systematic review and meta-analysis of randomised controlled trials
- In This Issue: Innovations in Primary Care and at the Annals