
Article Figures & Data
Figures
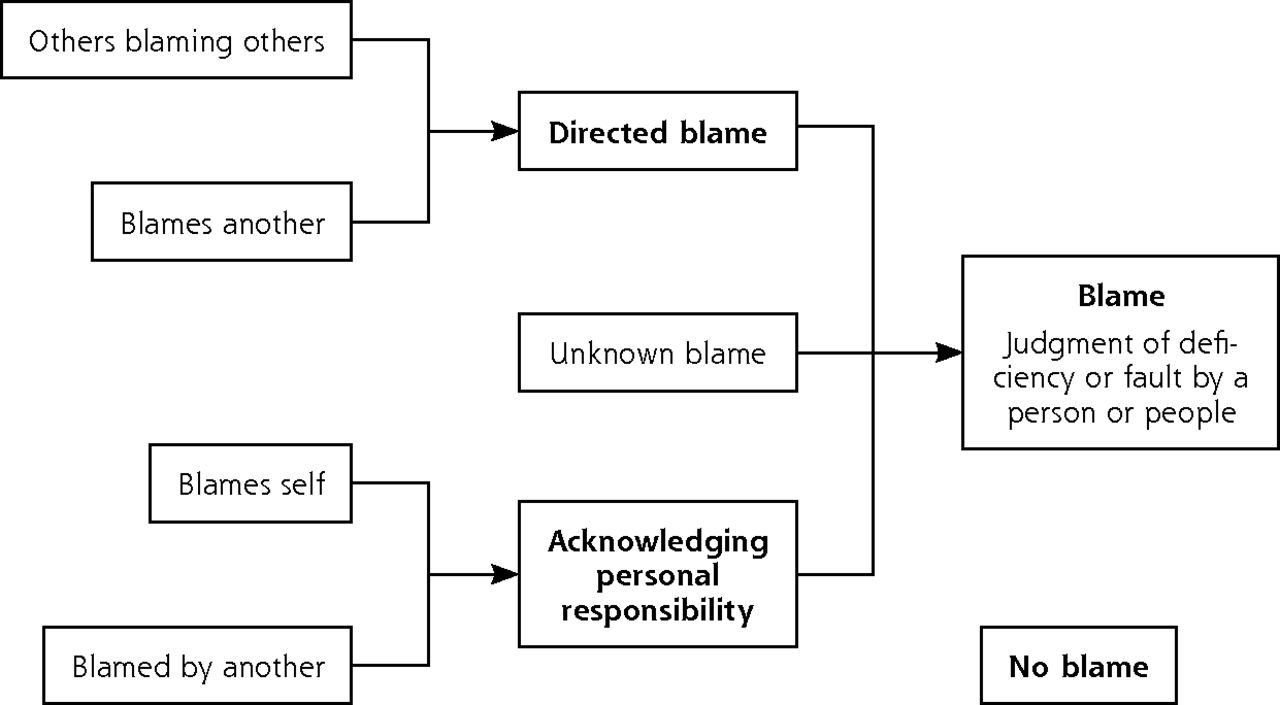
- Figure 1
Types of blame.
Tables
Blame Focus and Definition Example Acknowledging personal responsibility Blames self “Seen as temporary resident for an inguinal hernia awaiting operation. Was incarcerated (probably) and I acted on his history of this being reducible. I should have admitted him there and then and didn’t. No complaint by patient.” Blames himself/herself for the incident Blamed by another “The patient was diagnosed as having a [rare type of cancer]. He had attended the surgery on and off since [date] with urinary symptoms which seemed to respond to antibiotics. He saw every clinical member of the practice and was examined but a thorough examination was impossible. He was referred for a possible hernia on [date] and to the urology department on [date]. He was seen by both specialties within a week and diagnosis was confirmed. There has been a comment made to the family by a consultant that we should have spotted it sooner.” Describes a third party blaming him/her for the incident Directed blame Blames another Example 1: “A terminally ill patient attended A&E in possible retention of urine. This patient has a syringe driver in situ with morphine and metoclopramide. The syringe driver was clearly labelled as per policy but despite this the doctor who saw the patient in A&E took the syringe driver down and left the patient without any analgesia or anti-sickness medication. As a result, the patient was in a lot of pain and was only given a small amount of oral analgesia after being in A&E for some hours. TOTALLY UNACCEPTABLE. Medication error/critical incident. Complete lack of knowledge demonstrated by the doctor. Inadequate assessment and lack of knowledge on behalf of the doctor, and failure to listen to the patient, as he did question why they were taking the syringe driver down.” Blames another individual for the incident Others blaming others “Patient had an appointment with the doctor. Patient was in discomfort with problems swallowing and indigestion. This lady has complex co-morbidities. After a few days she felt very ill and thought it was the medication that had been prescribed on the day of her appointment. The patient contacted the practice but the practice would/could not provide an appointment that day or indeed the next day. The doctor eventually agreed to do another prescription without seeing her again (stemetil). When the patient went to collect the medication the pharmacist would not dispense the medication as it was not suitable for people with under active thyroid and it was for vertigo/nausea/vomiting. The patient could not raise this issue since the practice was then closed. The patient added that this is not the first time that something has happened like this.” Describes another individual being blamed for the incident Unknown blame “Patient with rheumatoid arthritis on steroids was taken off bone protection medication for 1 year giving a ‘drug free holiday’ to reduce the incidence of atypical fracture (without a review date to re-start). She had been on this medication for 7 years. Stopping this medication was inappropriate.” Blame identified but source unclear No blame “Computer system misinterpreted the directions for the dose of amiodarone and printed out 1/2 tablet daily instead of 1 1/2 stated on the prescription even though the patient’s computer record showed 1 1/2 daily as issued.” No attribution of blame to a person A&E = accident and emergency; GP = general practitioner; INR = international normalized ratio.
- Table 3
Likelihood of Directed Blame Attribution With Different Types of Safety Incidents Reported
Incident Type Reports No. Reports Containing Directed Blame No. (%) OR (95% CI)a Discharge planning 33 27 (82) 6.5 (2.7–15.8) Communication 36 25 (69) 3.3 (1.6–6.6) Referral 170 106 (62) 2.5 (1.8–3.5) Diagnosis and assessment 62 37 (60) 2.1 (1.3–3.6) Medication 417 228 (54) 1.9 (1.6–2.4) Administration 379 181 (48) 1.4 (1.1–1.7) Treatment 77 37 (48) 1.3 (0.8–2.1) Equipment provision 94 40 (43) 1.0 (0.7–1.6) Other 68 27 (40) 0.9 (0.6–1.5) Investigations 251 76 (30) 0.6 (0.4–0.8) Record keeping and documentation 80 19 (24) 0.5 (0.3–0.7) Vaccination 100 21 (21) 0.4 (0.2–0.6) Pressure ulcer 381 70 (18) 0.3 (0.2–0.3) OR=odds ratio.
↵a ORs for odds of directed blame when incident type is present vs incident type absent.
Contributory Factor Reports No. Directed Blame No. (%) OR (95% CI)a Staff factors (eg, staff knowledge, failure to follow protocols) 351 203 (58) 1.7 (1.3–2.3) Organizational factors (eg, staffing level, continuity of care) 216 122 (56) 1.4 (1.0–1.9) Patient factors (eg, frailty, language barrier) 263 100 (38) 0.5 (0.4–0.7) Equipment factors (eg, faulty or missing equipment) 35 8 (29) 0.3 (0.1–0.6) No contributory factors reported 1,283 461 (36) … All reports 2,148 894 (42) … OR=odds ratio.
↵a Comparing odds of directed blame where contributory factor is present vs odds of blame where an alternative contributory factor is present.
Variable Reports No. Directed Blame No. (%) OR (95% CI)a No harm 271 145 (54) 1.0 Mild 1,028 435 (42) 0.6 (0.6–0.9) Moderate 149 66 (44) 0.7 (0.7–1.4) Severe 21 2 (10) 0.1 (0.0–0.5) Death 6 5 (83) 4.4 (0.6–46.2) Patient out-come not reported 673 241 (36) … Total reports 2,148 894 (42) … ICPS = International Classification for Patient Safety; OR = odds ratio; WHO=World Health Organization.
Note: Based on WHO ICPS harm level classification.
↵a Odds of directed blame for each level of harm compared with odds of blame for no harm.
The Article in Brief
Nature of Blame in Patient Safety Incident Reports: Mixed Methods Analysis of a National Database
Andrew Carson-Stevens , and colleagues
Background A culture of blame and fear of retribution are recognized barriers to reporting patient safety incidents. The extent to which blame is assigned in patient safety incidents reports is unknown. This study set out to explore the nature of blame in family medicine incident reports.
What This Study Found When primary care staff members report patient safety incidents, they often attribute blame not to system failures but to the actions of individuals. Based on analysis of incident reports from the England and Wales National Reporting and Learning System, researchers found that healthcare professionals making incident reports attributed blame to a person in 45 percent of cases. In 36 percent of cases, reporters attributed fault to another person, while 2 percent of reporters took personal responsibility. Blame directed at others was more likely in discharge planning, communication, referrals, and diagnosis and assessment incidents, and was commonly associated with incidents where a complaint was anticipated.
Implications
- The high frequency of blame in primary care incident reports, the authors suggest, may reflect a health care culture that leads to blame and retribution. Improving patient safety through analysis of incident reports and identifying areas for learning will require a shift towards a culture that identifies system failures rather than blaming individuals, they conclude.
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- What became of the 'eyes and the ears?: exploring the challenges to reporting poor quality of care among trainee medical staff
- Patient and caregiver factors in ambulatory incident reports: a mixed-methods analysis
- Mixed-methods study protocol: do national reporting and learning system medication incidents in palliative care reflect patient and carer concerns about medication management and safety?
- Nature and type of patient-reported safety incidents in primary care: cross-sectional survey of patients from Australia and England
- In This Issue: Tools to Help Focus on What is Valuable