
Abstract
PURPOSE In July 2015, all children aged younger than 6 years gained free access to daytime and out-of-hours general practice services in the Republic of Ireland. Although 30% previously had free access, 70% did not.
METHODS To examine subsequent changes in service use, we retrospectively analyzed anonymized visitation data from 8 general practices in North Dublin providing daytime service and their local out-of-hours service, comparing the 1 year before and the 1 year after introduction of free care.
RESULTS In the year after granting of free general practice care for children younger than 6 years, 9.4% more children attended the daytime services and 20.1% more children were seen in the out-of-hours services. Annual number of visits by patients increased by 28.7% for daytime services and by 25.7% for out-of-hours services, translating to 6,682 more visits overall. Average visitation rate for children this age increased from 2.77 visits per year to 3.25 visits per year for daytime services, but changed little for out-of-hours services, from 1.52 visits per year to 1.59 visits per year.
CONCLUSIONS Offering free childhood general practice services led to a dramatic increase in visits. This increase has implications for future health care service planning in mixed public and privately funded systems.
- general practice
- health care utilization
- primary health care
- after-hours
- out-of-hours
- child
- pediatrics
- Ireland
- fee-for-service
- fees and charges
- practice-based research
- health planning
- state medicine
INTRODUCTION
Visitation rates are influenced by the way health care is financed.1,2 In the Republic of Ireland, 55% of all citizens do not qualify for state-funded, means-tested general practitioner care3 and thus must pay out-of-pocket fees (approximately US$50 to US$65) for each general practice visit.4
On July 1, 2015, all 440,000 children aged younger than 6 years in the Republic of Ireland were granted free access to general practice visits, regardless of parental income.5,6 This policy change allowed 300,000 additional children free visits to both daytime and out-of-hours care settings.6
The primary aim of this study was to use general practice electronic health records to analyze changes in daytime and out-of-hours service use since implementation of the new policy.
METHODS
We used anonymized retrospective visit data from general practice electronic health record systems. Ethical approval for the study was obtained from the Trinity College Dublin/Health Service Executive General Practice Training Scheme Ethics Committee.
Settings
We studied health care use in 2 settings: 8 daytime general practice services and their local out-of-hours service, called NorthDoc. NorthDoc offers urgent general practice services outside of normal office hours from 5 treatment centers in North County Dublin. It covers 140 participating general practices, including the 8 in this study.7 Data pertaining to face-to-face general practice visits were collected for a 1-year period before the date of introduction of free general practice care (July 1, 2014 to June 30, 2015) and for a 1-year period after that change (July 1, 2015 to June 30, 2016).
Data Collection
For daytime services, we sent all 140 practices registered with NorthDoc an e-mail inviting them to participate if they used the electronic health record Socrates. Eight practices indicated their interest and thus were included in this study.
For out-of-hours service, we collected anonymized visitation data for the study period from NorthDoc’s central database. All 140 general practices are included in this data set.
Analyses
We analyzed differences in the number of patients making visits, for both those paying out of pocket and those seen free of charge, and their number of visits in the period before and period after the policy change using the χ2 test.
RESULTS
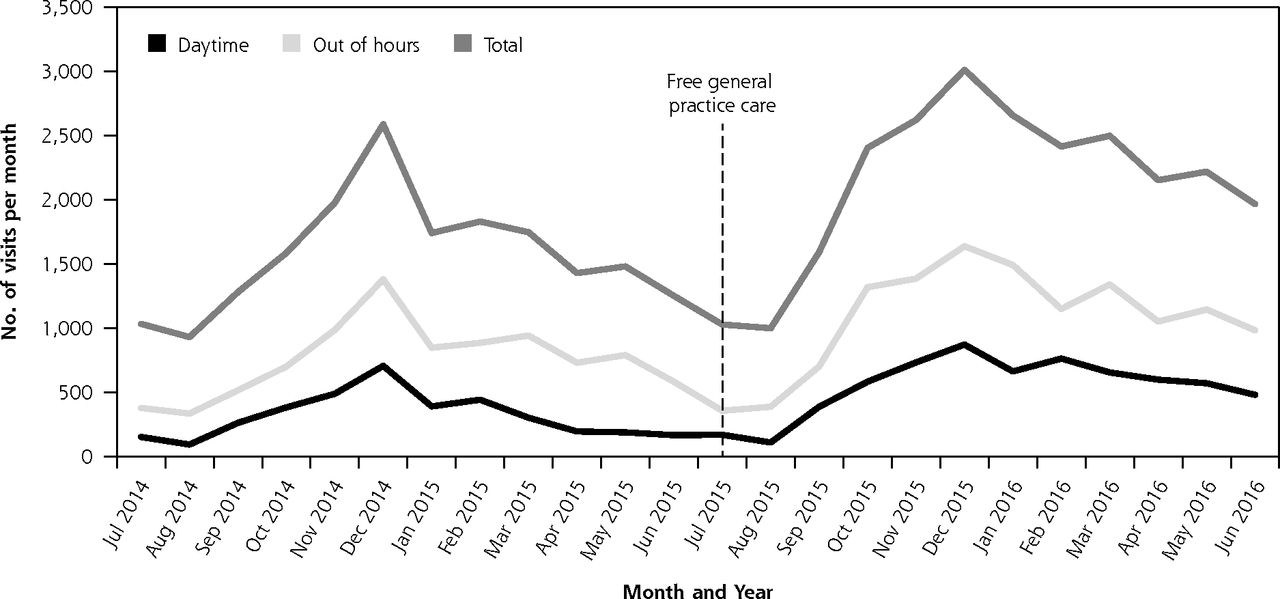
Table 1 shows general practice visitation data for both the daytime and out-of-hours settings. Comparison of the periods before and after the policy change showed significant increases in both numbers of patients and numbers of visits by children aged younger than 6 years, in daytime and out-of-hours settings alike (P <.001 for all). Figure 1 shows changes over time in number of visits per month for this age-group.
Comparison of General Practice Use in the Year Before and the Year After Policy Change

Temporal pattern of monthly general practice visits by children aged younger than 6 years.
Daytime Services
The number of children aged younger than 6 years who used the daytime general practice services at least once increased from 3,540 in the period before the policy change to 3,874 in the period thereafter (a 9.4% increase). General practitioners saw children this age for 9,789 visits in the former period and for 12,600 visits in the latter period (a 28.7% increase).
The average visitation rate for all children aged younger than 6 years rose from 2.77 (95% CI, 2.68–2.85) visits per patient per year in the period before policy change to 3.25 (95% CI, 3.17–3.33) visits per patient per year in the period after policy change. The number of children having free visits almost tripled to 3,347 during the latter period.
Out-of-Hours Services
A total of 9,898 children aged <6 years made 15,087 visits to the general practice out-of-hours service in the period before the policy change, and 11,890 children made 18,958 visits in the period after. The difference equated to 20.1% more children seen at least once and 25.7% more visits in the latter period.
The number of children seen free of charge more than doubled to 10,824 during the year after policy change. These children made a total of 17,290 visits. The average visitation rate for all children aged younger than 6 years changed little, from 1.52 visits per patient per year to 1.59 visits per patient per year comparing periods before and after the policy change.
DISCUSSION
Introduction of free general practice care for all children aged younger than 6 years led to a significant, if predictable, rise in the number of children seen free of charge and a sharp fall in the number paying out of pocket. The out-of-pocket number did not drop to zero, however, as some parents used general practice services before completing the application process for free visits. Overall, 9% and 20% more children attended the daytime and out-of-hours services, respectively, at least once in the year after the policy change.
Number of visits by children aged younger than 6 years increased in both settings by more than 25%. After the granting of free care, the overall visitation rates for children younger than 6 years approached that of those seen free of charge before the policy change. Although both the daytime and out-of-hours services saw more patients of all ages in the period after the policy change, children aged younger than 6 years accounted for a disproportionate increase in service use: 45% and 73% of the additional visits in the year after the policy change to the daytime and the out-of-hours services, respectively, were by children this age.
The birth rate dropped by 3% over the study period8 and numbers of general practitioners employed in each setting were similar throughout the study. In addition, although seasonal variation was seen as usual (Figure 1), there were no notable disease outbreaks in North Dublin during the study period that otherwise might explain increased service use. Further research is needed to establish whether severity of medical issues changed when access was free and whether increased workload had effects on general practitioners and patients.
Demand for general practice services is increasing worldwide, both in daytime settings9,10 and out-of-hours settings.11,12 Equitable access should be a cornerstone of any health care system, but making services available free of charge inevitably increases service use. In the Republic of Ireland, there are already indications that the general practitioner workforce may struggle to meet demand in the near future,13,14 so future plans to extend state-funded general practice care to all groups15 will require careful workforce planning.
Acknowledgments
The authors wish to thank the general practitioners and the out-of-hours cooperative NorthDoc for facilitating analysis of their anonymized visitation data.
Footnotes
Conflicts of interest: authors report none.
- Received for publication June 26, 2017.
- Revision received September 22, 2017.
- Accepted for publication November 22, 2017.
- © 2018 Annals of Family Medicine, Inc.
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- Paediatric attendances of the emergency department in a major Irish tertiary referral centre before and after expansion of free GP care to children under 6: a retrospective observational study
- Childrens unscheduled primary and emergency care in Ireland: a multimethod approach to understanding decision making, trends, outcomes and parental perspectives (CUPID): project protocol
- A real-time measurement of general practice workload in the Republic of Ireland: a prospective study
- In This Issue: Sometimes More is Less