
Abstract
Confidence in hepatitis B seroprotection for US health care workers includes a complete immunization series followed by a hepatitis B surface antigen antibody (anti-HBs) titer ≥10 mIU/mL. We compared standard hepatitis B vaccines to Heplisav-B (Dynavax Technologies Corp) as a single booster for young, healthy, previously vaccinated individuals. Participants (N = 242) had documentation of a single vaccination series and an anti-HBs titer <10 mIU/mL. In this cohort, 1 booster achieved seropositivity for 92.7% (95% CI, 84.8%-97.2%) of the standard hepatitis B vaccine group and 99.4% (95% CI, 96.6%-100.0%) of the Heplisav-B group. Both boosters are likely to produce seropositivity in this population.
INTRODUCTION
Health care workers, particularly trainees, are at increased risk of hepatitis B infection via accidental occupational blood or body fluid exposure.1,2 In the United States, health care workers are considered fully protected after showing a hepatitis B surface antigen antibody (anti-HBs) titer ≥10 mIU/mL drawn ≥30 days after a full vaccination series. For this higher-risk group, both are required.3 Many health care workers were vaccinated in childhood and have never been tested for titer response before entering the workforce.
Recombivax HB (Merck & Co, Inc), Engerix-B (GlaxoSmithKline, Inc), and Twinrix (GlaxoSmithKline, Inc) are the currently available hepatitis B vaccines indicated for use in adults and children in the United States. The most common application is a 3-dose series in childhood. A new vaccine (Heplisav-B [Dynavax Technologies Corp]) that uses an immune adjuvant, synthetic cytosine-phosphate-guanine oligonucleotide (CpG 1018), was approved in 2017 for use in nonpregnant individuals aged >18 years.4 Primary series response rates are greater for Heplisav-B compared with standard vaccines.5 There is some evidence that this vaccine can result in a protective immune response for individuals who have not responded to 2 prior complete vaccination series.6,7 Data on the use of this product as a single-dose booster for health care workers is limited. We therefore investigated the response to a booster dose of either Heplisav-B or standard hepatitis B vaccine in previously vaccinated health care workers.
METHODS
Study Design
We used a retrospective cohort design to evaluate existing health record data. We collected data by chart review for individuals matriculating to the doctor of medicine program at the Uniformed Services University of the Health Sciences for academic years 2019 to 2022. Collected data included only the dates and types of hepatitis B vaccines documented and the results of any anti-HBs tests. To protect student privacy, no individual demographic information was collected, though aggregate demographic data are available for this population. Students were categorized on the basis of their initial postvaccination anti-HBs test as seropositive (≥10 mIU/mL) or potentially susceptible (<10 mIU/mL or qualitative test not positive). Potentially susceptible individuals who had documentation of a full hepatitis B vaccine series were categorized into 2 groups according to the vaccine received as a booster dose. Because Heplisav-B was not on the market until 2017, all individuals’ initial vaccine series would have been standard hepatitis B vaccines. Those who received any additional hepatitis B vaccine before their follow-up anti-HBs titer were not included in the study. Remaining individuals were then categorized as susceptible (<10 mIU/mL) or seropositive (≥10 mIU/mL) according to testing performed ≥30 days after the booster.
The institutional review board for the Uniformed Services University of the Health Sciences approved the protocol (954179). We used χ2 tests to compare proportions between groups. The CIs for individual groups used the Clopper-Pearson calculation. We performed statistical analysis using Stata statistical software (release 18; StataCorp LLC).
RESULTS
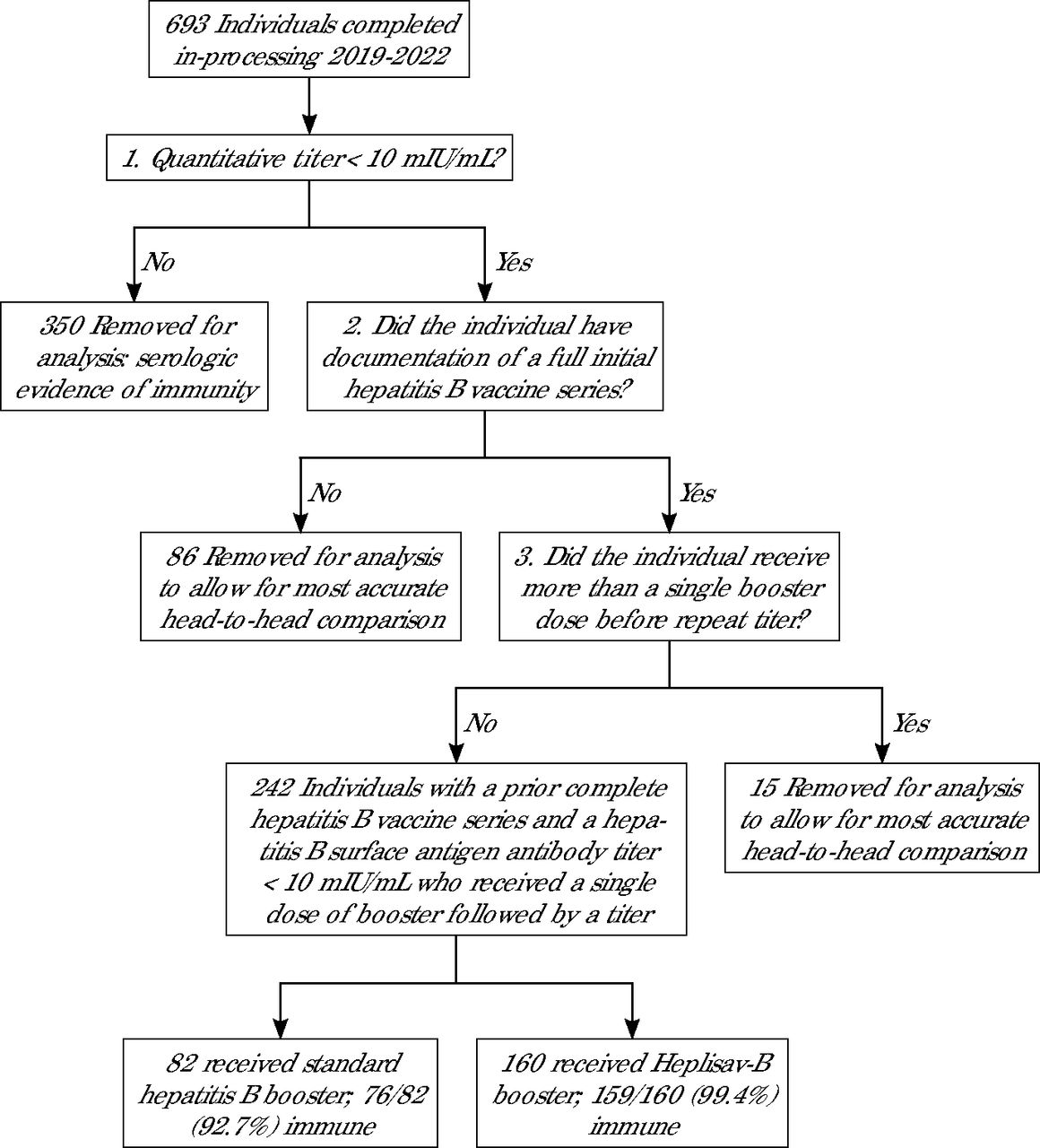
Figure 1 shows the inclusion and exclusion process, resulting in a total of 242 students who tested nonseropositive, had documentation of completing a previous vaccination series, and received a single booster vaccination. The mean age of the 693 students who completed in-processing from 2019 to 2022 was 25 years (range, 20-43 years). The specific characteristics of the 35% of that population who met inclusion criteria are not known.

Data Flowchart for Inclusion Based on Hepatitis B Titer and Vaccine History
The mean time between completion of the initial hepatitis B vaccination series and the first titer was similar for both groups (Table 1). A single booster resulted in 92.7% of individuals in the standard hepatitis B vaccine group and 99.4% in the Heplisav-B group meeting the US Centers for Disease Control and Prevention threshold for protection for health care workers. The percent difference (6.7%) was statistically significant (95% CI, 1.9%-14.5%; P = .003) All 7 individuals who remained at anti-HBs <10 mIU/mL after the booster attained a level ≥10 mIU/mL after additional hepatitis B vaccinations.
Response to Single Booster Dose of Hepatitis B Vaccine in Previously Vaccinated Military Medical Studentsa
Supplemental Figures 1 and 2 contain the post-booster titer distribution. The numerical value of a post-booster titer is less clinically relevant than categorization as seropositive or not. Statistical analysis of these distributions is also complicated by the common lab practice of reporting high end values as >1000 miU/mL rather than their absolute value. contain the post-booster titer distribution. The numerical value of a post-booster titer is less clinically relevant than categorization as seropositive or not. Statistical analysis of these distributions is also complicated by the common lab practice of reporting high end values as >1000 miU/mL rather than their absolute value. contain the post-booster titer distribution. The numerical value of a post-booster titer is less clinically relevant than categorization as seropositive or not. Statistical analysis of these distributions is also complicated by the common lab practice of reporting high end values as >1000 miU/mL rather than their absolute value. contain the post-booster titer distribution. The numerical value of a post-booster titer is less clinically relevant than categorization as seropositive or not. Statistical analysis of these distributions is also complicated by the common lab practice of reporting high end values as >1000 miU/mL rather than their absolute value.
DISCUSSION
Both groups achieved a high level of response to a single booster dose of hepatitis B vaccine. Consistent with our findings, previous studies of health care workers published before the availability of Heplisav-B have shown a 71% to 93% response rate to a single standard booster.8 Our finding of an absolute increase of 6.7% in the proportion at anti-HBs ≥10 mIU/mL after a single booster suggests that vaccinating 15 individuals with Heplisav-B rather than standard vaccine could result in 1 more person being seropositive. This number needed to vaccinate could be as high as 53 or as low as 7, given the CI of 1.9% to 14.5%.
Limitations of this study include the deidentified nature of the data. We were unable to consider factors such as gender, race, or exact age at vaccination. Military members are screened for chronic diseases and therefore might not be representative of other health care worker populations. Adverse event data were not available for this cohort. The 3 types of standard hepatitis B vaccine were grouped in this study. Whereas this is consistent with clinical practice, differences between these vaccines were not assessed. The specific booster vaccine administered was not randomized. The titer values used for analysis were reported by commercial laboratories in the medical records. The characteristics of the test used were not available to the authors.
CONCLUSION
Given the high response rate to a single booster, these data suggest that a single booster is reasonable for young, healthy, health care workers who never showed seropositivity. Heplisav-B was more effective than standard hepatitis B vaccine in this study population; however, further research is needed to determine if the observed effect is replicable in other populations and if the magnitude of that effect justifies the increased per-dose cost of Heplisav-B.
Footnotes
Conflicts of interest: authors report none.
Disclaimer: The opinions and assertions expressed herein are those of the author(s) and do not reflect the official policy or position of the Uniformed Services University of the Health Sciences or the US Department of Defense.
Previous presentation: Presented at the Uniformed Services Academy of Family Physicians 2024 Annual Meeting; March 23-27, 2024; New Orleans, Louisiana.
- Received for publication April 15, 2024.
- Revision received November 7, 2024.
- Accepted for publication November 11, 2024.
- © 2025 Annals of Family Medicine, Inc.
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.