
Abstract
PURPOSE Employment is a key social determinant of health. People who are unemployed typically have worse health than those employed. Illness and disability can result in unemployment and be a barrier to regaining employment. We combined a systematic review and knowledge synthesis to identify both studies of employment interventions in health care settings and common characteristics of successful interventions.
METHODS We searched the peer-reviewed literature (1995–2017), and titles and abstracts were screened for inclusion and exclusion criteria by 2 independent reviewers. We extracted data on the study setting, participants, intervention, methods, and findings. We also conducted a narrative synthesis and iteratively developed a conceptual model to inform future primary care interventions.
RESULTS Of 6,729 unique citations, 88 articles met our criteria. Most articles (89%) focused on people with mental illness. The majority of articles (74%) tested interventions that succeeded in helping participants gain employment. We identified 5 key features of successful interventions: (1) a multidisciplinary team that communicates regularly and collaborates, (2) a comprehensive package of services, (3) one-on-one and tailored components, (4) a holistic view of health and social needs, and (5) prospective engagement with employers.
CONCLUSIONS Our findings can inform new interventions that focus on employment as a social determinant of health. Although hiring a dedicated employment specialist may not be feasible for most primary care organizations, pathways using existing resources with links to external agencies can be created. As precarious work becomes more common, helping patients engage in safe and productive employment could improve health, access to health care, and well-being.
- social determinants of health
- employment
- systematic review
- work
- health care settings
- working conditions
- chronic disease
- vulnerable populations
- primary care
INTRODUCTION
Employment status is a key social determinant of health.1,2 Being employed influences our financial security, sense of self, social connections, and social status. Unemployment is associated with worse physical and mental health at the individual level, and is correlated with poorer health at the community level3–6 and higher mortality rates.7,8 Employment status plays an important mediating role in the strong relationship between income and health.7 Beyond income, a number of individual and contextual factors influence the relationship of employment with health, including gender identity, race and ethnicity, immigration status, and social class.9,10 The relationship between employment and health is bidirectional. Those with chronic health issues are less likely to enter and remain in the workforce, and are more likely to require assistance with attaining employment.11–14
Helping people gain employment is often the role of charitable organizations, government agencies, and in some cases, the private sector; however, the health sector may also have a role.15,16 A number of studies have evaluated employment interventions embedded in health settings, including Vocational Rehabilitation, Supported Employment, and Individual Placement and Support (Table 1).12,17–26 These models emerged in the 1970s from community-based mental health care.27,28
Types of Employment Interventions Within Health Care Settings
More recently, primary care organizations have invested in upstream interventions to address the social determinants of health,29–34 including addressing unemployment. For example, interventions based on the Health Leads model use volunteers to connect patients with community resources, including employment.35 Medical-legal partnerships may assist patients who have been denied wages or fired,36 although they do not typically focus on assisting them in gaining employment.37 No previous review has thoroughly examined employment interventions in health settings or identified successful components of interventions that move patients from unemployment to employment. Our objective was to identify interventions implemented within health care settings that assisted patients with gaining employment, and to ascertain common characteristics of successful interventions, in order to inform new ways to address employment as a social determinant of health.
METHODS
We carried out a systematic review to identify all relevant studies of interventions within health settings that sought to help unemployed patients gain employment, to identify which interventions were successful and to estimate the efficacy of different interventions. We blended this method with a knowledge synthesis to build a conceptual model of how these interventions work, to inform future interventions.
We followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines for systematic reviews.38 Our protocol was registered with the International Prospective Register of Systematic Reviews (PROSPERO, registration: CRD42016049518). We developed a search strategy in consultation with an information specialist. To identify studies that would be most relevant to current employment conditions,4,39 we limited our search of the peer-reviewed literature to articles published since 1995. We searched the following databases: Ovid MEDLINE, PubMed, Embase, EBM Reviews (Cochrane Database of Systematic Reviews, Database of Abstracts of Reviews of Effects, Cochrane Central Register of Controlled Trials, Cochrane Methodology Register, Health Technology Assessment, NHS Economic Evaluation Database), Scopus, CINAHL, Theses Canada Portal, and ProQuest Dissertations and Theses Global (Supplemental Appendix 1, available at http://www.annfammed.org/content/16/5/447/suppl/DC1/).
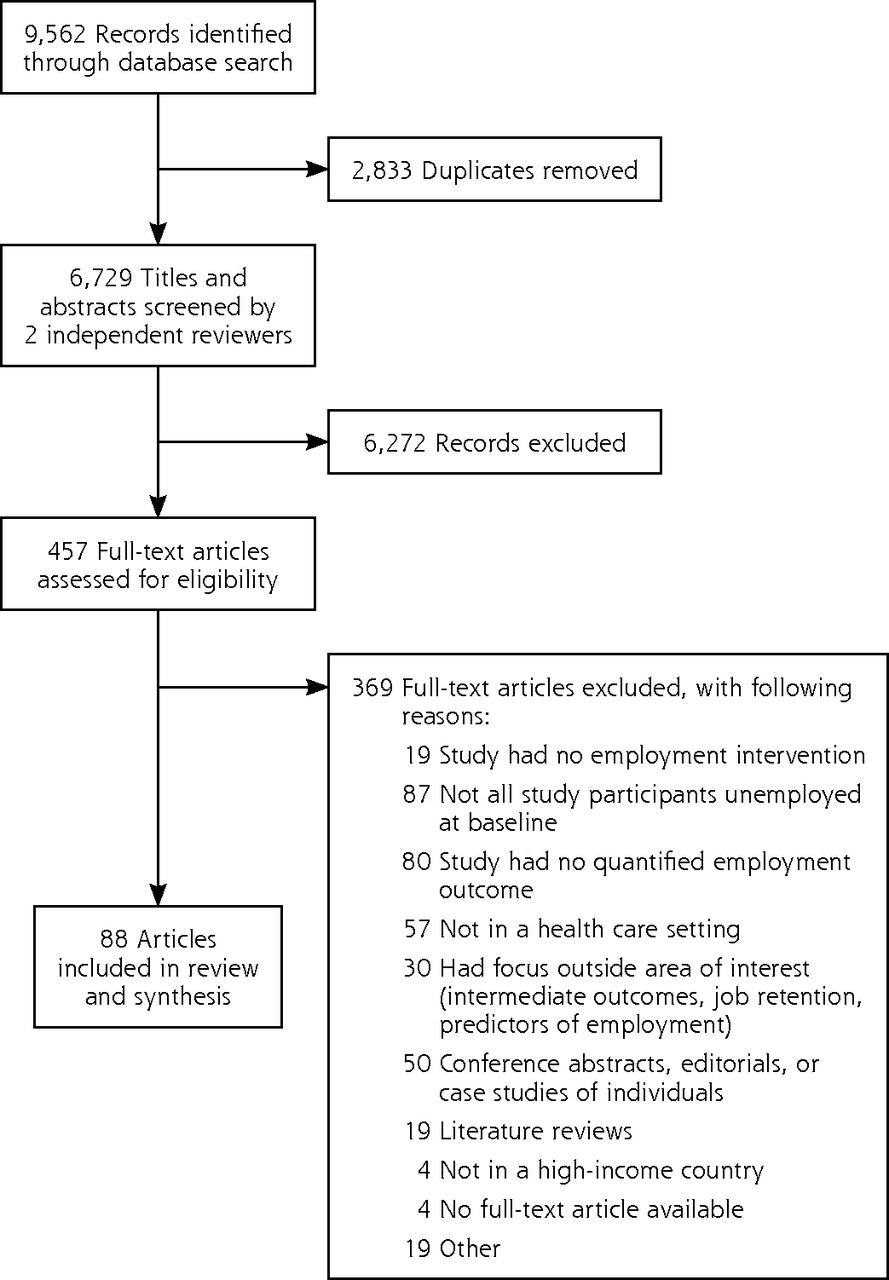
Titles and abstracts were screened by 2 independent reviewers. Exclusion criteria are shown in Figure 1. Health care settings were defined as locations where the main purpose was to deliver health services, including primary care centers, hospitals, emergency departments, community health centers, health centers in prisons, and walk-in clinics. We excluded studies that combined data from both health care and non–health care settings and state Vocational Rehabilitation agencies. An individual was considered to be employed if they had paid work, and unemployed if they did not have paid work, were not on a leave of absence from work, or had no job to return to. We did not exclude articles on the basis of patient characteristics (such as age, sex, or diagnosis). We focused on studies conducted in high-income countries (as defined by the World Bank) because low-and middle-income countries are considerably different contexts in terms of health care settings, economic conditions, and social supports. We did not limit our search by any specific language. The full texts agreed on by both reviewers were screened to determine whether they met inclusion criteria. If there was a disagreement about whether an article should be included, the study team and principal investigator met to jointly make a final decision.

PRISMA flow diagram.
We developed a standardized, pilot-tested data extraction form and used it to extract data from included articles (Supplemental Appendix 2, available at http://www.annfammed.org/content/16/5/447/suppl/DC1/). The quality of individual studies was assessed using standardized tools. Randomized controlled trials were assessed using the Cochrane Collaboration Risk of Bias Tool.40 Observational studies were assessed using a 9-point rigor scale developed by the World Health Organization and Johns Hopkins.41
We anticipated that the studies identified would be heterogeneous with respect to design, employment outcomes, and follow-up time points, which would preclude a meta-analysis on a single end point. We conducted a narrative synthesis, however, to bring together the key components of successful interventions, and defined a positive employment outcome as an individual gaining paid work. Two authors (N.H., A.C-N.) independently read all full-text articles included, inductively developed themes from the studies, and iteratively developed the final categories. A conceptual model was developed and iteratively refined by the entire study team as the reviewers’ understanding of interventions and their components evolved.
RESULTS
Article Characteristics
A total of 88 articles ultimately met our criteria and were included (Figure 1, Supplemental Appendix 2). Forty-eight articles (54%) reported on studies conducted in the United States. Of the total, 48 (54%) described randomized controlled trials, 31 (35%) prospective cohort studies, and 9 (10%) retrospective cohort studies. Across all study types, 58 (66%) had a control or comparison group.
The quality of the 48 randomized controlled trials was moderate, with a low risk of bias with respect to randomization method (34 trials), allocation concealment (32 trials), blinding of outcome assessors (36 trials), incomplete outcome data (37 trials), and selective outcome reporting (27 trials) (Table 2).20,24–26,42–85
Assessment of the Risk of Bias in Randomized Controlled Trials (n = 48)
Of the 40 observational studies, the majority included preintervention and postintervention data (28 studies) and followed a cohort (39 studies), but fewer than one-half of the studies included control or comparison groups (13 studies) or controlled for potential confounders (15 studies) (Table 3).11,23,86–123 In general, randomization was not applicable. The follow-up rate was reported or applicable in only 19 studies and was at least 80% in just 10 of them. The average rigor score was 3 out of 9, suggesting the quality of the observational studies was low.
Assessment of the Rigor of Observational Studies (n = 40)
Most of the 88 articles (89%) focused on patients with mental illness. The type of health setting was known for 81 (92%), with the majority situated in community mental health centers or their equivalent. Only 3 were located in settings that also provided primary care. Two of these studies were carried out in Sweden, one involving mobile teams that integrated primary care and mental health services for people with severe mental illness48 and the other engaging a similar population through outpatient clinics.49 One study took place within a US community health center with a focus on people living with HIV/AIDS.96 All 3 were positive studies, with significantly improved employment outcomes in the intervention groups.
Interventions and Outcomes
Although the 88 articles reported on a variety of interventions, the majority (73%) focused on Supported Employment interventions. Intervention groups ranged in size from 13 to 1,340 participants, with 1 article reporting on 27,408 participants from 17 sites.115 When multiple articles referred to the same study, we counted these participants only once. In total, our review reports on 42,428 individuals who received an employment intervention.
Of the 48 randomized controlled trials, 37 (77%) achieved significantly higher employment outcomes in the intervention group compared with the traditional vocational services or control group. Similarly, 28 (70%) of the 40 observational studies demonstrated positive employment outcomes for study participants. Two employment interventions in the United Kingdom were unsuccessful (ie, did not have significantly increased rates of employment among the study population), and the authors found that the context of the United Kingdom compared with that of the United States contributed to this difference.62,102 Because Individual Placement and Support is not integrated into the mental health system in the United Kingdom, as is typical in the United States, the employment service is often provided by an external agency.62 The United Kingdom also had a lack of incentives for employers to hire employees with mental illnesses, and there were differences in government support.
We examined the success rate at 1 year, or the time point closest to 1 year, excluding a single study that did not report on the success of the intervention.106 Across successful studies, the average increase in any type of employment was 51% (range = 11% to 100%). If we consider only the studies that had comparison groups or controls, the average increase in employment was 28% (range = 11% to 79%).
Key Features of Successful Interventions
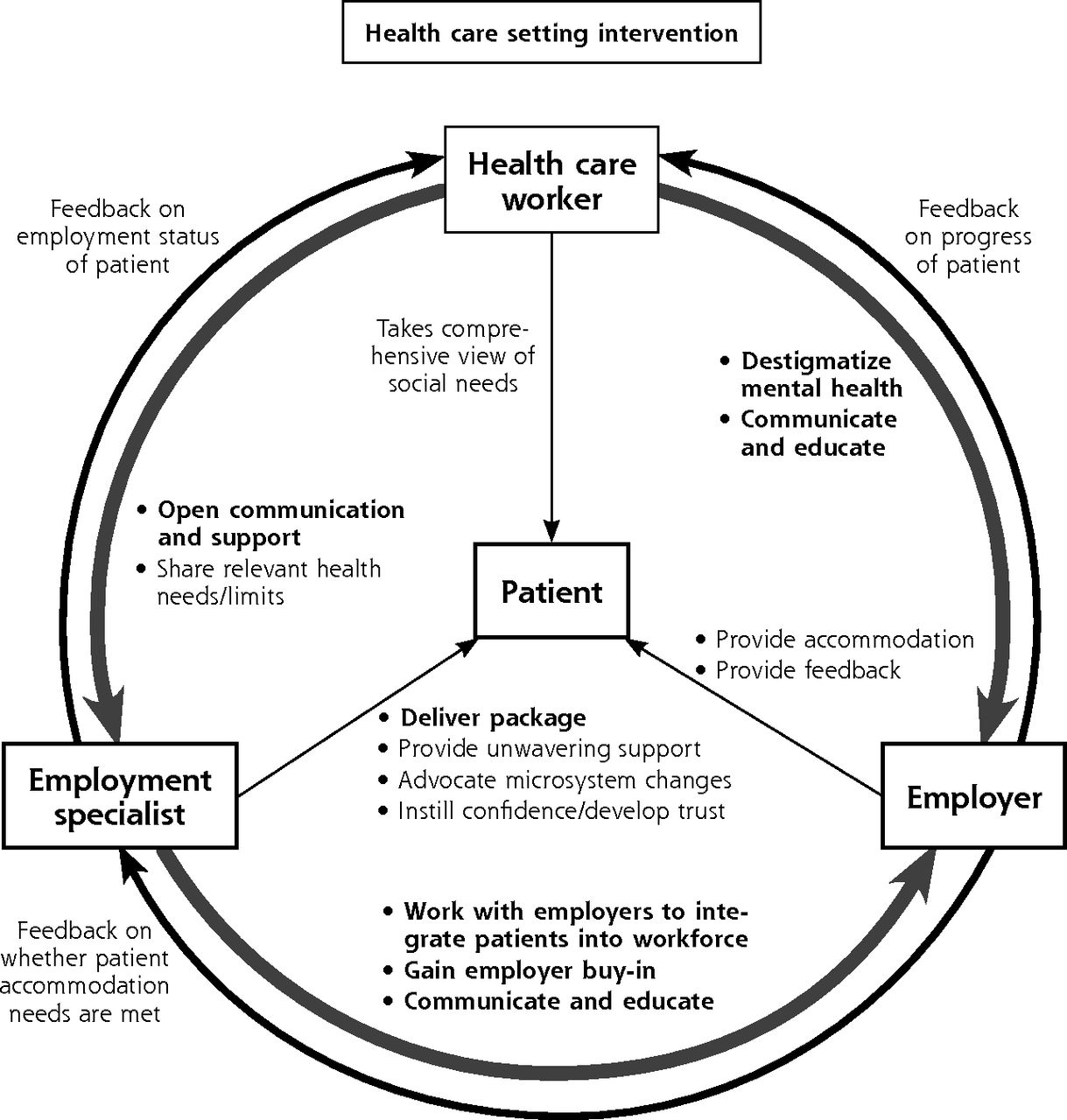
Our synthesis brought together the 5 key features common in successful interventions, with a focus on those that were supported by findings from multiple studies that were rigorous (Supplemental Appendix 3, available at http://www.annfammed.org/content/16/5/447/suppl/DC1/). Although each feature is presented separately, there are certainly areas of overlap and intersection (Figure 2). All of these features were present in the studies of interventions that were delivered in settings that also provided primary care.48–50
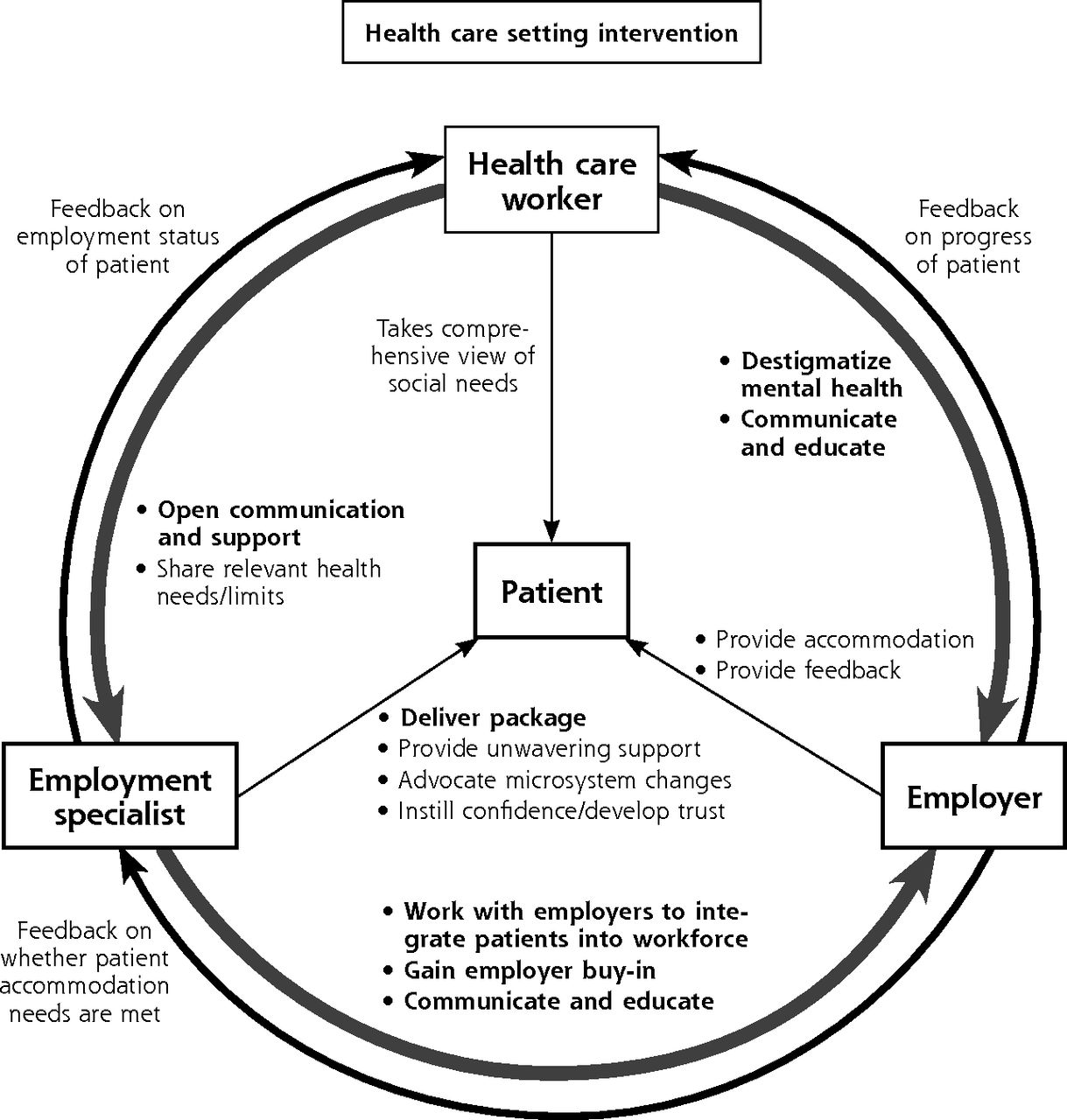
Successful interventions include patient-centered relationships among the health care worker, employment specialist, and employer.
Note: All relationships are focused on the goal of achieving employment for the patient. Bold text denotes features derived from evidence in the systematic review. Nonbold text denotes features not found in the evidence; however, we include them in the model because they were considered important and are supported in other literature.
A Multidisciplinary Intervention Team With Open Communication to Address Patient Needs
Successful interventions were patient centered and engaged a multidisciplinary team, composed of health care workers and employment specialists, who communicated consistently.20,65,76 The majority of articles (61 of 88), including high-quality randomized controlled trials, described how integrated, multidisciplinary, coordinated services were important characteristics of the intervention. Integrating clinical and employment services achieved significantly higher competitive employment rates compared with the control.63 Having the entire team in the same space allowed for better understanding of each other’s roles, responsibilities, and skills across disciplines, which better enabled the patient’s needs to be met.120
Eleven studies described ongoing communication across the multidisciplinary team as a key component of the intervention.* Ongoing communication between health and employment specialists ensured that the patient’s health needs and strengths were considered when looking for potential work and that any challenges were addressed once they secured employment.69
Successful intervention teams were patient centered, focused on helping patients meet their goals and take control of the process. Trust between the employment specialist and the patient helped participants discuss challenges.124 Five successful studies77,78,86,116,118 cited the importance of the patient’s relationship with the physician, while an unsuccessful Individual Placement and Support intervention62 found that mental health professionals did not expect patients to work and had low general expectations of them.
Patients Receive a Package of Services Including Expert Advice, a Job Search, Feedback, Networking, Education and Training, and Peer Mentorship
Successful interventions provided patients with access to advice from an expert (eg, a case manager), a rapid and competitive job search, ongoing feedback and support, networking to employers, education and training, and peer mentor support. Sixty-six studies described having dedicated full-time employment specialists or case managers as a critical component of employment interventions. Job coaches were experienced in the rehabilitation of people with mental illness and had maximum caseloads of 12 participants to ensure that support was provided to each.60 Forty-six studies described how several successful interventions provided rapid competitive job searches and matching. For people with severe mental health illnesses, acquiring employment early or within the first months of an intervention can be important because motivation and confidence may decline later on.75
Fifty-four studies described the importance of ongoing feedback and support in their employment interventions. More specifically, 9 studies found that using positive reinforcement and encouragement, and providing hope to patients was important in successful employment interventions. Positive reinforcement could be provided through certificates, awards, and public recognition.20 Five studies found that networking and providing individuals with access to job contacts were useful.25,88,95,115,120 Forty-seven studies described how education, training on topics such as interview skills, and developing social skills or on-site job training was important and associated with better employment outcomes. Thirteen studies used peer mentors to provide support to individuals through initiatives such as monthly peer support groups to assist with vocational development.114
Services Are One on One and Tailored
Successful interventions provided one-on-one services to individuals that were tailored to their job preferences, skills, education, and previous work experience. Forty studies described how such services enhanced the intervention. A one-to-one interaction allowed for a strong relationship between the employment specialist and each client.51 Fifty studies described how interventions were tailored and individualized to participants. Employment specialists worked with each individual to ensure that they based their search for competitive employment on that individual’s educational background, previous experiences, and preference for a work area.60
Services Are Holistic and Take a Comprehensive View of Social Needs
Successful interventions provided a holistic model of care and addressed social determinants of health aside from employment. Eight studies acknowledged the importance of addressing these other determinants, such as housing and having appropriate clothes to wear to work.23 Integration of the employment specialist into the health care team brought the social determinants of health to the forefront of primary care.23,76,90,102 Having an employment service champion promoted organizational buy-in.102 At health care centers where Supported Employment interventions were provided, the clinical staff were more likely to ask their patients about employment status.76 Employment interventions have been noted to positively influence clinician attitudes, helping them to see the importance of supporting employment outcomes.125
Intervention Team Works With and Engages Employers
In successful interventions, employers were able to receive support, education, and incentives, and in some cases provided accommodation for disabilities. Eight studies described how employers received support from the intervention team. In an intervention for people living with AIDS, staff worked to ensure that the employer was supported in responding to challenges.96 Interventions included providing employers with education from health care professionals, answering questions, and pointing out benefits of hiring those with mental illness, as well as employer training workshops to destigmatize mental illness.95,114 Six studies, including a number of observational studies that were highly rigorous, reported the advantages of employer buy-in and incentives to take on individuals with health concerns as a means of reducing barriers to entering the workforce.60–62,64,95,114 Five studies described how employers provided accommodation to employees, such as individualizing schedules.44,52,64,106,114
DISCUSSION
We identified 88 articles reporting studies of interventions in health settings that aimed to move patients from unemployment to employment. Key features of successful interventions were consistent across multiple studies. Such interventions typically deployed multidisciplinary teams that communicated well and placed patients—and their medical, psychological, and social needs—at the center. They provided a package of employment services and engaged employers proactively. Part of the role of the employment specialist was helping patients navigate different systems having different requirements.126 The impact on health remains unclear, as our review found modest improvements in quality of life, and no studies demonstrating that gaining employment altered functioning or mental health.127,128
Addressing unemployment is one way to tackle an underlying cause of poor health. Having an integrated team with health care workers and employment specialists can help to reduce barriers for patients entering the workforce. Individuals who work in settings that are not stigmatizing can experience improved self-esteem, satisfaction, and sense of empowerment.129 With health issues such as multiple sclerosis and traumatic brain injuries, early referral to an employment intervention was important in ensuring that patients gained employment.130 Our findings suggested that having employment interventions in health care settings integrates these services to best serve patients.
The findings of our study fit with those of other studies that have examined employment interventions, particularly those that focused on people living with mental illness. A previous review confirmed the importance of a tailored approach.131 A Cochrane systematic review of Supported Employment in severe mental illness found this approach was effective, although individual studies had substantial bias, and few examined the durability of the intervention.132 As we found, the overall quality of the evidence in this area, particularly for observational studies, was low.132–135 Variation in outcomes across employment interventions warrants exploration.136
Our study has limitations. Because of publication bias, negative studies may not have been published. Although we conducted a quality assessment of every study, there were instances wherein risk of bias or rigor of the study was unclear. Key features of the successful interventions were extracted, but these features may not be comprehensive. Certain interventions had multiple publications and may be overrepresented in this review. Finally, we could not conduct a meta-analysis because of the heterogeneous nature of the studies.
Our conceptual model can assist with the design and implementation of employment interventions within health care settings. Given that most studies included in this review occurred outside of primary care, further research will be required to evaluate how employment interventions can be integrated within first-contact, team-based, longitudinal care provided to diverse populations. Although hiring a dedicated employment specialist may not be feasible, certain team-based primary care organizations can develop a pathway for patients dealing with unemployment and precarious employment. This pathway could involve raising awareness of employment as a key social determinant of health across the primary care team, training internal staff (eg, social workers, community health workers, or system navigators) to provide support based on the key components we identified, and building relationships with external employment services.
This review is timely given that standard permanent full-time work has been on the decline in favor of part-time, contract, and other unregulated work that increases job insecurity.4 Precarious employment that is not stable and of acceptable quality can be detrimental to workers’ health, and these workers have higher psychological morbidity compared with permanent workers.137–139 We defined a positive employment outcome as gaining employment of any form, yet the quality of employment (eg, wage rate, working conditions, exposure to hazards, psychological stress) that workers experience is important to consider. If the focus is simply on placing people in any job available, there is a high likelihood that these will be low-quality jobs with little security or few benefits.140 Future interventions should assess and report on the quality of jobs in a consistent manner.
Employment is an important social determinant of health, and integrating employment interventions into health care settings presents an innovative way to assist patients. These interventions are complex, and further research is required on screening for unemployment and precarious employment,141,142 and to evaluate the long-term impact of interventions across different health care settings and with diverse patients. The evidence from this systematic review demonstrates that there are key features of successful interventions in health care settings that are useful in informing future interventions. This work contributes to emerging theory that supports addressing the social determinant of health in clinical settings.32,143
Acknowledgments
We appreciate the assistance of Arman Hamidian and Priyanka Chowdhury in reviewing citations and articles for this study. We are grateful to Carolyn Ziegler for her assistance in designing and carrying out the search of databases. Finally, we thank Anne Rucchetto for her assistance in editing this manuscript.
Footnotes
Conflicts of interest: authors report none.
Funding support: This study was supported by a grant from the Atkinson Foundation Decent Work Fund. Dr Pinto receives salary support from the Department of Family and Community Medicine and the Li Ka Shing Knowledge Institute at St Michael’s Hospital, Toronto. Dr Pinto is also supported by a Clinician-Scientist Award from the Department of Family and Community Medicine, Faculty of Medicine, University of Toronto.
Disclaimer: The study funder played no role in the design of the study, data collection, data analysis, interpretation of data, or the writing and editing of this article.
Previous presentation: Findings from this study were presented at the Trillium Research Day; May 31, 2017; Toronto, Ontario, Canada.
Supplemental Materials: Available at http://www.AnnFamMed.org/content/16/5/447/suppl/DC1/.
- Received for publication November 16, 2017.
- Revision received April 30, 2018.
- Accepted for publication May 10, 2018.
- © 2018 Annals of Family Medicine, Inc.
References
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- A Brief Tool to Screen Patients for Precarious Employment: A Validation Study
- Access to family resources by families living with schizophrenia: a qualitative study of primary care workers in urban Beijing, China
- Mise en {oelig}uvre dinterventions sociales en soins de sante primaires
- Vocational interventions to help adults with long-term health conditions or disabilities gain and maintain paid work: an overview of systematic reviews
- Implementing social interventions in primary care
- Should we screen for poverty in primary care?
- In This Issue: Nothing Simple