
Article Figures & Data
Figures
- Figure 1
EvidenceNOW external quality improvement strategies.
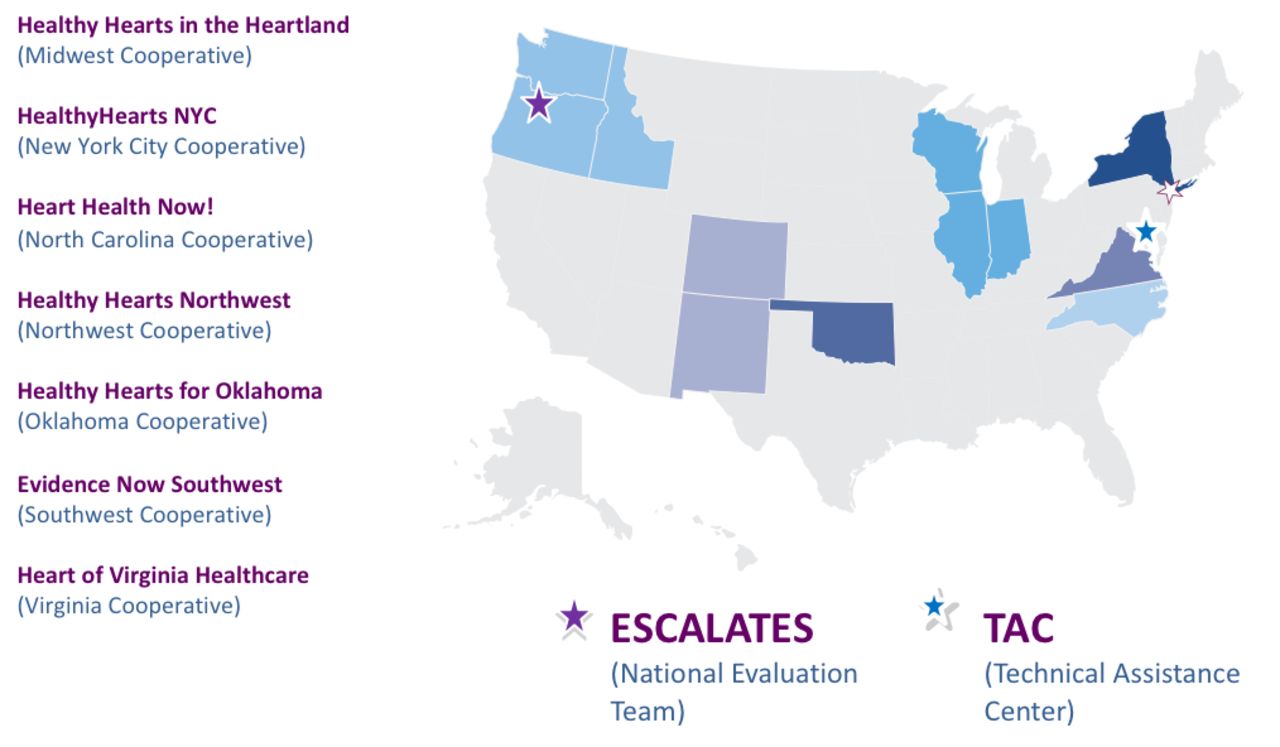
- Figure 2
Geographic reach of EvidenceNOW.
ESCALATES = Evaluating System Change to Advance Learning and Take Evidence to Scale; TAC = Technical Assistance Center.


Tables
Measure Definition A: Aspirin use (Source: CMS164v4) Proportion of patients aged 18 years and older who were discharged alive for acute myocardial infarction, coronary artery bypass graft or percutaneous coronary interventions in the 12 months before the measurement period, or who had an active diagnosis of ischemic vascular disease during the measurement period, and who had documentation of use of aspirin or another antithrombotic during the measurement period B: Blood pressure control (Source: CMS165v4) Proportion of patients aged 18 to 85 years who had a diagnosis of hypertension and whose blood pressure was adequately controlled (<140/90 mm Hg) during the measurement period C: Cholesterol management (Source: PQRS 438) Proportion of the following patients—all considered at high risk of cardiovascular events—who were prescribed or were on statin therapy during the measurement period: Adults aged 21 years and older who were previously diagnosed with or currently have an active diagnosis of clinical atherosclerotic cardiovascular disease, or
Adults aged 21 years and older with a fasting or direct LDL-C level (≥190 mg/dL), or
Adults aged 40–75 years with a diagnosis of diabetes with a fasting or direct LDL-C level of 70–189 mg/dL
S: Smoking cessation (Source: CMS138v4) Percentage of patients aged 18 years or older who were screened about tobacco use 1 or more times within 24 months and who received cessation counseling intervention if identified as a tobacco user CMS = Centers for Medicare and Medicaid Services; EHR = electronic health record; LDL-C = low-density lipoprotein cholesterol; PQRS = Physician Quality Reporting System.
Required Measures Domain(s) Change Process Capacity Questionnaire Practice capacity Measurement of adaptive reserve Practice capacity National Ambulatory Medical Care Survey Electronic Medical Records questionnaire (2010) Internal context (includes practice organization, staffing, and patient population, and an assessment of the degree of EHR adoption of each practice and the ability of the practice to report quality measures) Concurrent practice improvement initiatives External context (for example, QIO/QINs, CMMI, CPCI, and TCPI) Supporting strategies External context (for example, pay-for-performance and public reporting initiatives) Implementation and adaptation of comprehensive approach to quality improvement support Possible aspects to address: acceptability, adoption, appropriateness, feasibility, fidelity, implementation costs, and sustainability Intervention tracking Specific strategies used with individual primary care practices (adaptation to local circumstances was allowed) CMMI=Center for Medicare & Medicaid Innovation; CPCI=Comprehensive Primary Care Initiative; EHR=electronic health record; QIN=Quality Innovation Network; QIO=Quality Improvement Organization; TCPI=Transforming Clinical Practice Initiative.
Domains of measurement Practice capacity, adaptive reserve Leadership and organizational style Quality improvement structures and processes Team-ness Staff satisfaction and burnout
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- What AHRQ Learned While Working to Transform Primary Care
- Declining Participation in Primary Care Quality Improvement Research: A Qualitative Study
- Tailoring Implementation Strategies for Cardiovascular Disease Risk Calculator Adoption in Primary Care Clinics
- How Does Prior Experience Pay Off in Large-Scale Quality Improvement Initiatives?
- Tailoring Implementation Strategies for Cardiovascular Disease Risk Calculator Adoption in Primary Care Clinics
- Improving Delivery of Cardiovascular Disease Preventive Services in Small-to-Medium Primary Care Practices
- How Does Prior Experience Pay Off in Large-Scale Quality Improvement Initiatives?
- Improving Delivery of Cardiovascular Disease Preventive Services in Small-to-Medium Primary Care Practices
- Considerations Before Selecting a Stepped-Wedge Cluster Randomized Trial Design for a Practice Improvement Study
- Improving Quality Improvement Capacity and Clinical Performance in Small Primary Care Practices
- Place Matters: Closing the Gap on Rural Primary Care Quality Improvement Capacity--the Healthy Hearts Northwest Study
- A Taxonomy for External Support for Practice Transformation
- Implementation of Community-Based Resource Referrals for Cardiovascular Disease Self-Management
- Identifying Practice Facilitation Delays and Barriers in Primary Care Quality Improvement
- A Qualitative Analysis of Implementing EvidenceNOW to Improve Cardiovascular Care
- A Randomized Trial of External Practice Support to Improve Cardiovascular Risk Factors in Primary Care
- Facilitating Practice Transformation in Frontline Health Care
- Practice-based Research Network (PBRN) Engagement: 20+ Years and Counting
- The Capacity of Primary Care for Improving Evidence-Based Care: Early Findings From AHRQs EvidenceNOW
- Technical Assistance for Primary Care Practice Transformation: Free Help to Perform Unpaid Labor?
- Engaging Primary Care Practices in Studies of Improvement: Did You Budget Enough for Practice Recruitment?