
Article Figures & Data
Figures
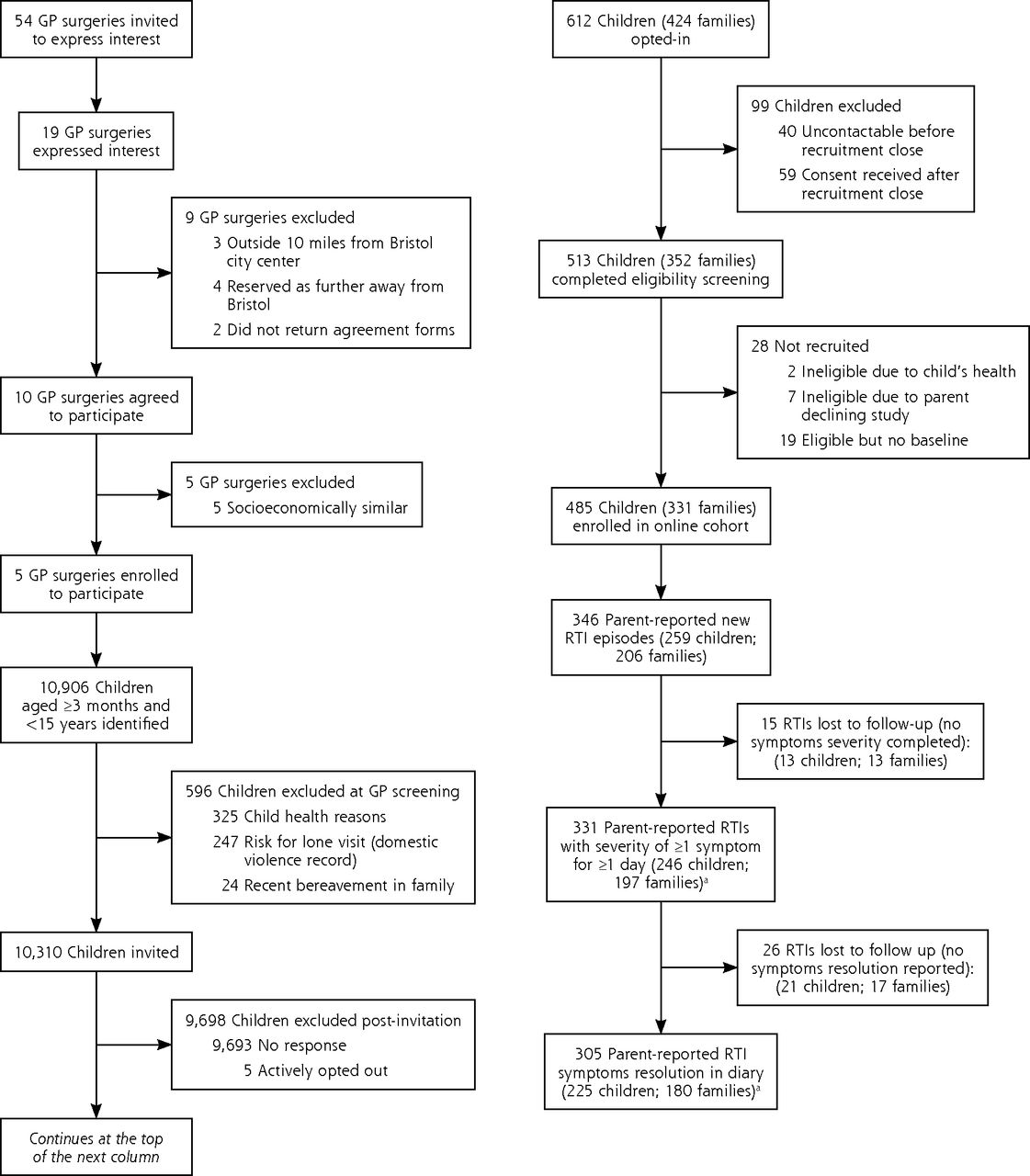
- Figure 1
Flow diagram of participant recruitment.
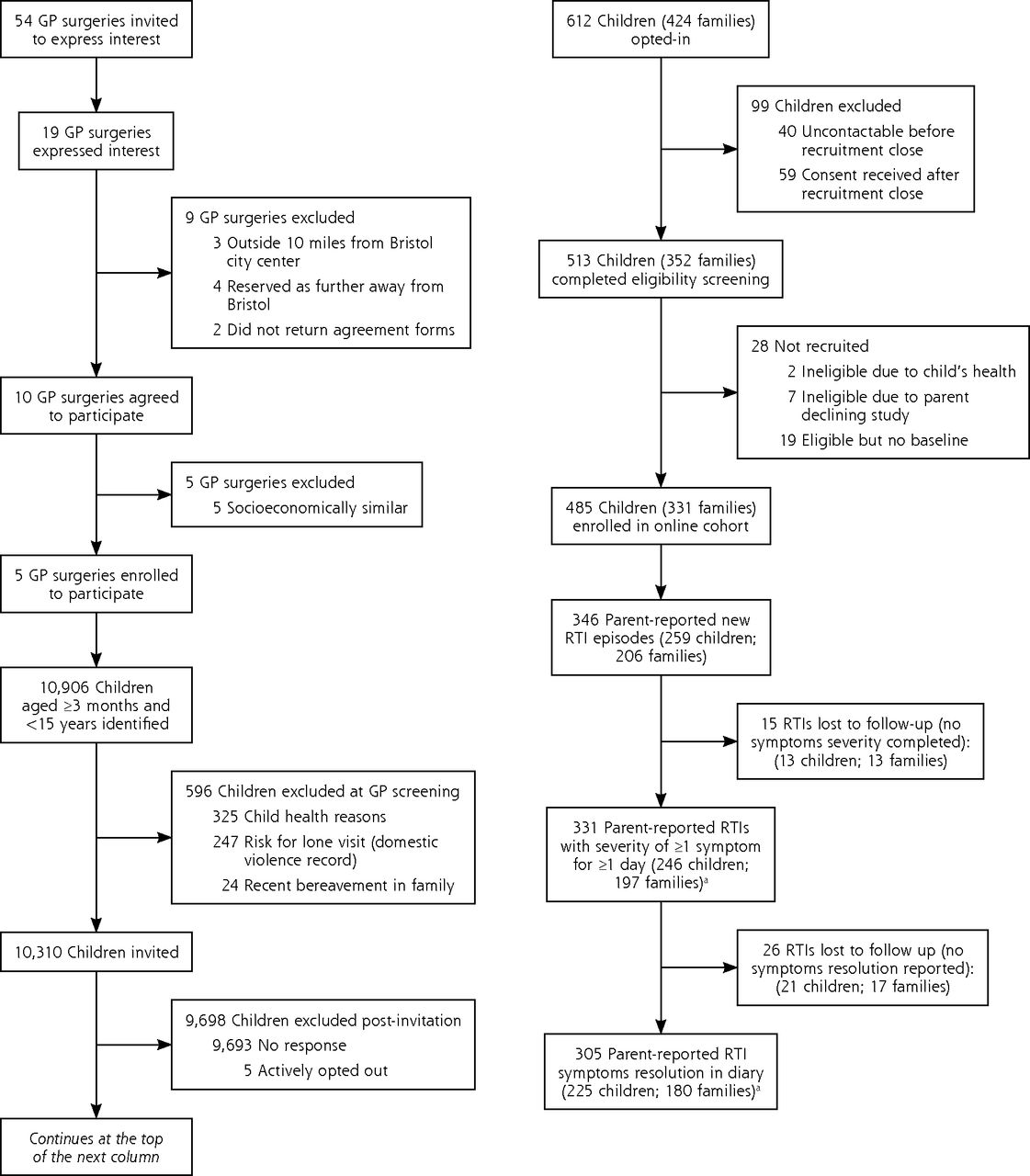
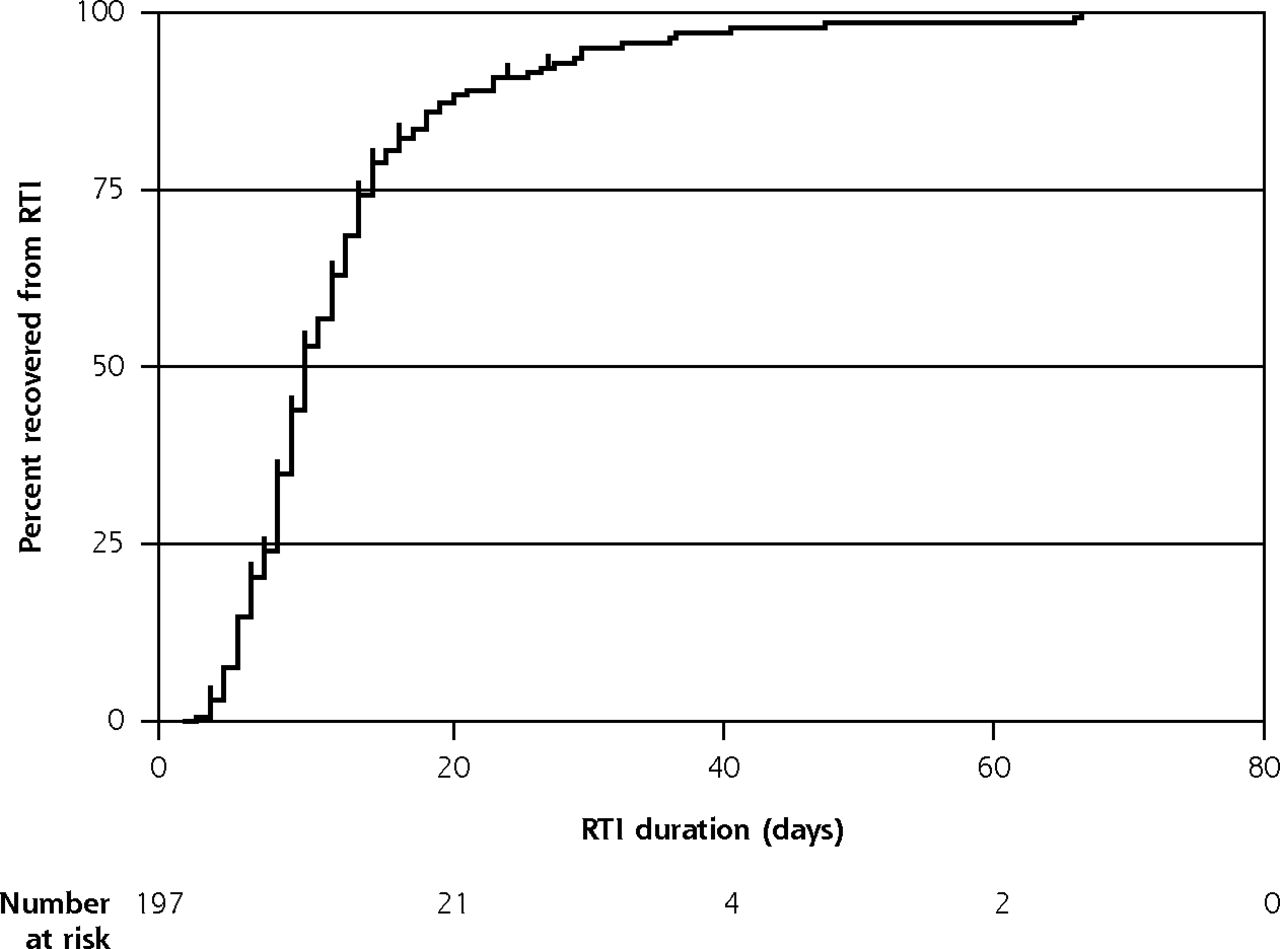
- Figure 2
Kaplan-Meier curve showing time to RTI symptom resolution (with number censored), restricted to the first RTI in a family with illness start date recorded (n = 197).

Tables
- Table 1
Baseline Characteristics of Parents, Children, and Households, According to Whether or Not Symptom End Dates Were Recorded, and Restricted to the First RTI Episodes in a Family (n = 206)
Characteristics First RTI Episodes (n = 206) Symptom End Dates Recorded? No (n = 26) Yes (n = 180) Parents Sex, No. (%) Missing 2 (0.97) Female 193 (93.69) 26 (100.00) 167 (93.82) Male 11 (5.34) 0 (0.00) 11 (6.18) Age, median (IQR), y 38 (34-43) 36 (34-41) 38 (34-43) Ethnicity, No. (%) Missing 9 (4.37) Asian 5 (2.43) 0 (0.00) 5 (2.91) Black 5 (2.43) 2 (8.00) 3 (1.74) Mixed 5 (2.43) 1 (4.00) 4 (2.33) White 182 (88.35) 22 (88.00) 160 (93.02) Employment, No. (%) Missing 9 (4.37) Full-time parent/caregiver 34 (16.50) 4 (16.00) 30 (17.44) In full-time education 2 (0.97) 0 (0.00) 2 (1.16) Not currently employed 8 (3.88) 2 (8.00) 6 (3.49) Working full time 41 (19.90) 7 (28.00) 34 (19.77) Working part time 112 (54.37) 12 (48.00) 100 (58.14) Education, No. (%) Missing 9 (4.37) No official qualification 2 (0.97) 0 (0.00) 2 (1.16) Up to GCSEs/GCEs/O Levels or equivalent 8 (3.88) 4 (16.00) 4 (2.33) A Levels/NVQs/GNVQs or equivalent 9 (4.37) 2 (8.00) 7 (4.07) First degree/diploma/HNC/HND 107 (51.94) 11 (44.00) 96 (55.81) Higher degree (eg, MSc, PhD) 71 (34.47) 8 (32.00) 63 (36.63) Any medical/nursing training, No. (%) Missing 9 (4.37) No 155 (75.24) 22 (88.00) 133 (77.33) Yes 42 (20.39) 3 (12.00) 39 (22.67) Children Age, (median, IQR), y 3 (1-7) 3 (1-6) 3 (1-7) Sex, No. (%) Female 114 (55.34) 15 (57.69) 99 (55.00) Male 92 (44.66) 11 (42.31) 81 (45.00) Ethnicity, No. (%) Asian 6 (2.91) 1 (3.85) 5 (2.78) Black 5 (2.43) 1 (3.85) 4 (2.22) Mixed 11 (5.34) 3 (11.54) 8 (4.44) White 184 (89.32) 21 (80.77) 163 (90.56) Asthma, No. (%) No 187 (90.78) 22 (84.62) 165 (91.67) Yes 19 (9.22) 4 (15.38) 15 (8.33) Eczema, No. (%) No 128 (62.14) 18 (69.23) 110 (61.11) Yes 78 (37.86) 8 (30.77) 70 (38.89) Hay fever, No. (%) No 186 (90.29) 22 (84.62) 164 (91.11) Yes 20 (9.71) 4 (15.38) 16 (8.89) Child receiving any breast milk at 3 months, No. (%) Don’t know 2 (0.97) 1 (3.85) 1 (0.56) No 30 (14.56) 4 (15.38) 26 (14.44) Yes 174 (84.47) 21 (80.77) 153 (85.00) Child attending school, No. (%) No 125 (60.68) 15 (57.69) 110 (61.11) Yes 81 (39.32) 11 (42.31) 70 (38.89) Child (not in school) attending daycare regularly, No. (%) Not relevant (attends school) 81 No 36 (28.80) 6 (40.00) 30 (27.27) Yes (1-2 days per week) 50 (40.00) 6 (40.00) 44 (40.00) Yes (3-5 days per week) 39 (31.20) 3 (20.00) 36 (32.73) Households Bedrooms, No. (%) Missing 9 1 4 (2.03) 2 (8.00) 2 (1.16) 2 47 (23.86) 5 (20.00) 42 (24.42) 3 86 (43.65) 9 (36.00) 77 (44.77) 4 42 (21.32) 6 (24.00) 36 (20.93) 5 14 (7.11) 3 (12.00) 11 (6.40) 6 3 (1.52) 0 (0.00) 3 (1.74) 7 0 (0.00) 0 (0.00) 0 (0.00) 8 1 (0.51) 0 (0.00) 1 (0.58) Resident smoker, No. (%) Missing 9 No 181 (91.88) 22 (88.00) 159 (92.44) Yes 16 (8.12) 3 (12.00) 13 (7.56) Cat/dog in main home, No. (%) Missing 9 No 141 (71.57) 16 (64.00) 125 (72.67) Yes 56 (28.43) 9 (36.00) 47 (27.33) Number of adults resident in child’s main home, No. (%) Missing 9 0 1 (0.51) 0 (0.00) 1 (0.58) 1 15 (7.61) 2 (8.00) 13 (7.56) 2 164 (83.25) 20 (80.00) 144 (83.72) 3 11 (5.58) 0 (0.00) 11 (6.40) 4 5 (2.54) 3 (12.00) 2 (1.16) 8 1 (0.51) 0 (0.00) 1 (0.58) Total number of children in home, No. (%) Missing 9 1 80 (40.61) 8 (32.00) 72 (41.86) 2 103 (52.28) 15 (60.00) 88 (51.16) 3 12 (6.09) 1 (4.00) 11 (6.40) 4 1 (0.51) 0 (0.00) 1 (0.58) 5 0 (0.00) 1 (4.00) 0 (0.00) Age of children in home, median (IQR), y 3 (2-7) 2 (1-6) 3 (2-7) A level = advanced level; GCE = general certificate of education; GCSE = general certificate of secondary education; GNVQ = general national vocational qualification; HNC = higher national certificate; HND = higher national diploma; IQR = interquartile range; MSc = master of science; NVQ = national vocational qualification; O level = general certificate of education ordinary level; PhD = doctor of philosophy; RTI = respiratory tract infection.
- Table 2
Duration and Severity of RTI Symptoms, Restricted to First RTI in a Family With Known Illness Start Date (n = 197)
Group No. RTI Duration by Percentile, d P Valuea 10th 25th 50th 75th 90th All children 197 4 7 9 14 23 Children with and without consultationb Consultation 16 6 9 13 18 37 .06 No consultation 181 4 6 9 13 21 Upper and lower RTI symptomsc,d Exclusively URTI 86 3 5 8 11 15 <.001 Any LRTI 104 6 8 12 18 29.5 Constitutional symptom severity scoree for upper and lower RTI, mean of maximum Upper RTI Lower RTI Fever 0.55 1.07 Fatigue 0.83 1.71 Disruption to sleep 1.15 2.19 Disruption to other activities 0.67 1.43 LRTI = lower respiratory tract infection; NHS = National Health Service; RTI = respiratory tract infection; URTI = upper respiratory tract infection.
↵a Log-rank test for difference between episodes with consultions and those without consultions.
↵b Any NHS primary care attendance according to medical notes.
↵c 7 RTI episodes which did not report any URTI- or LRTI-defining symptoms.
↵d URTI symptoms: earache, sore throat, runny/blocked nose, ear discharge, dry cough or barking/croupy cough. LRTI symptoms: wet/productive cough, breathing faster/shortness of breath, or wheeze/whistling chest.
e Maximum of daily scores in first 21 days, based on Likert scale 0 (normal, no problem) to 6 (as bad as it could be).
- Table 3
Effect of Deprivation/Baseline Characteristics on RTI Symptom Duration and Consultations, Restricted to First RTI in a Family With Illness Start Date (n = 197)
Characteristic No. Consultation, No. (%) P Value Median Duration, d P Value Parent education level No official qualification 2 0 (0.0) 1 GCSE/GCE/O level 6 0 (0.0) 14 A level/NVQ/GNVQ 9 1 (11.1) .93 7 .09 First degree (diploma/HNC/HND) 105 9 (8.6) 10 Higher degree (MSc/PhD) 67 5 (7.5) 9 Missing 8 1 (12.5) 7 Age of child ≥3 years 106 9 (8.5) .87 11 <.01 >3 years 91 7 (7.7) 7 Missing 0 0 (0.0) 0 Household Index ofMultiple Deprivation 1 (most deprived) 74 5 (6.8) 9 2 57 5 (8.8) .83 9 .79 3 (least deprived) 63 6 (9.5) 9 Missing 3 0 (0.0) 23 A level = advanced level; GCE = general certificate of education; GCSE = general certificate of secondary education; GNVQ = general national vocational qualification; HNC = higher national certificate; HND = higher national diploma; MSc = master of science; NVQ = national vocational qualification; O level = general certificate of education ordinary level; PhD = doctor of philosophy; RTI = respiratory tract infection.
- Table 4
Sensitivity Analyses for Overall RTI Duration and Duration Stratified by Child’s Consultation Attendancea
Group No. RTI Duration by Percentile, d P Valueb 10th 25th 50th 75th 90th Primary comparison (reference Table 2) First RTI in a family All 197 4 7 9 14 23 .06 Consultation 16 6 9 13 18 37 Non Consultation 181 4 6 9 13 21 Sensitivity analyses First RTI in a child All 246 4 7 9 14 23 .05 Consultation 18 6 11 13 18 37 Non Consultation 228 4 6 9 14 21 All RTIs All 338 4 7 10 15 26 <.01 Consultation 34 8 13 14 27 28 Non Consultation 304 4 6 9 14 21
Supplemental Appendixes
Supplemental appendixes
Files in this Data Supplement:
- Supplemental data: Appendix - PDF file
The Article in Brief
Respiratory Tract Infections in Children in the Community: Prospective Online Inception Cohort Study
Alastair D. Hay , and colleagues
Background Accurate knowledge of respiratory tract symptoms and their duration is an essential part of self-care, helping patients know when to seek help. This study uses novel online methods to estimate the duration of children's respiratory symptoms and the proportion of parents visiting primary care for those symptoms.
What This Study Found It takes 23 days for 90 percent of children to recover from respiratory tract infection symptoms. Researchers followed 485 children in 331 families in Bristol, England as they fell ill with respiratory tract infections (n=197 respiratory tract infections). Overall, median duration of symptoms was 9 days. For children three years of age or younger, median symptom duration was 11 days compared to seven days for older children. Children whose parents reported lower respiratory tract symptoms (such as wet cough and wheeze) had median symptom duration of 12 days compared to eight days for those who had only upper respiratory tract symptoms (such as runny nose and sore throat). Among children with only upper respiratory tract symptoms, the most persistent symptom was runny nose, while the fastest symptom to resolve was earache. For children with at least one lower respiratory tract symptom, all symptoms persisted for three weeks; runny nose and wet cough were the most severe symptoms. One in 12 parents sought help from their family physician.
Implications
- These findings, the authors suggest, could inform primary care practice, public health interventions, and, ultimately, parents regarding the concerning symptoms for which they should consult their primary care physician.




{kind=link}
{kind=link}