
Article Figures & Data
Figures
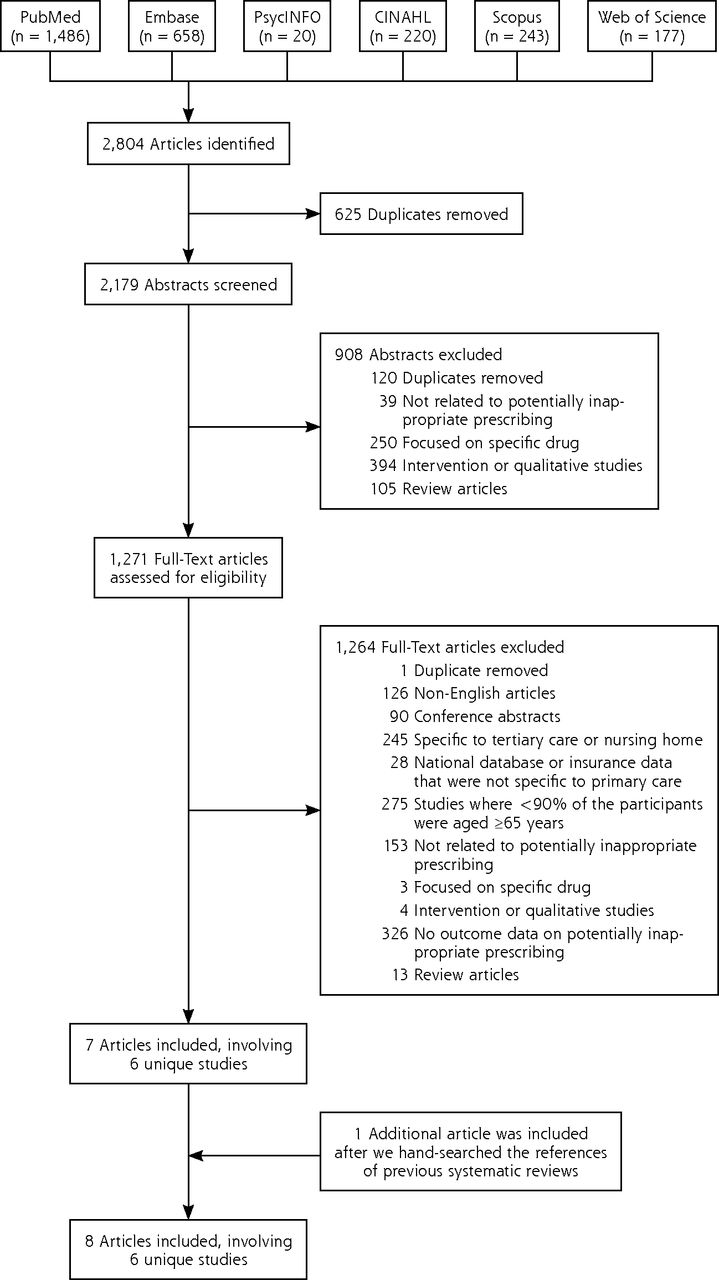
- Figure 1.
Flowchart of the study selection.
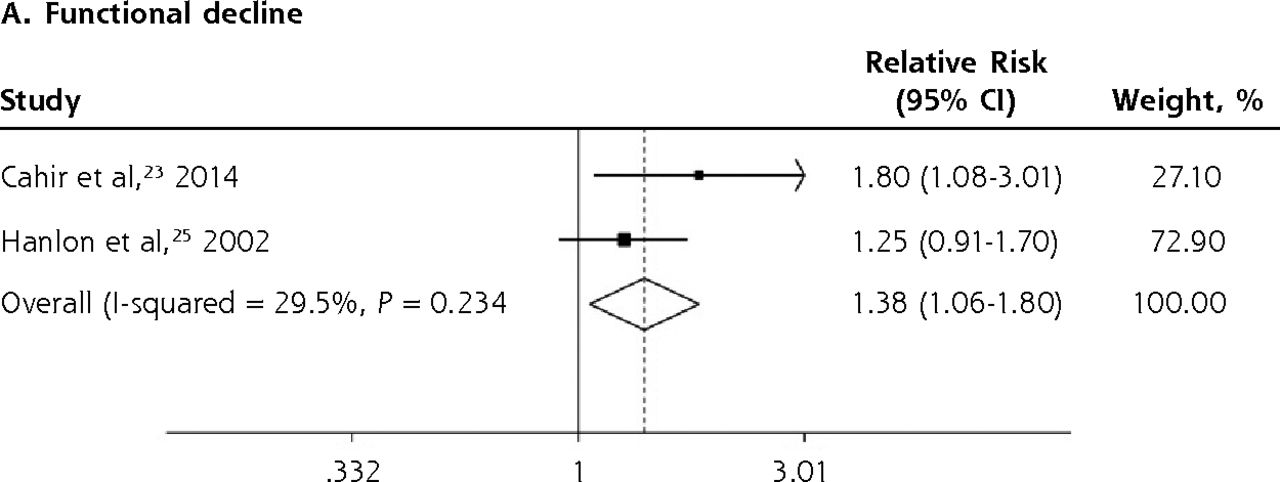
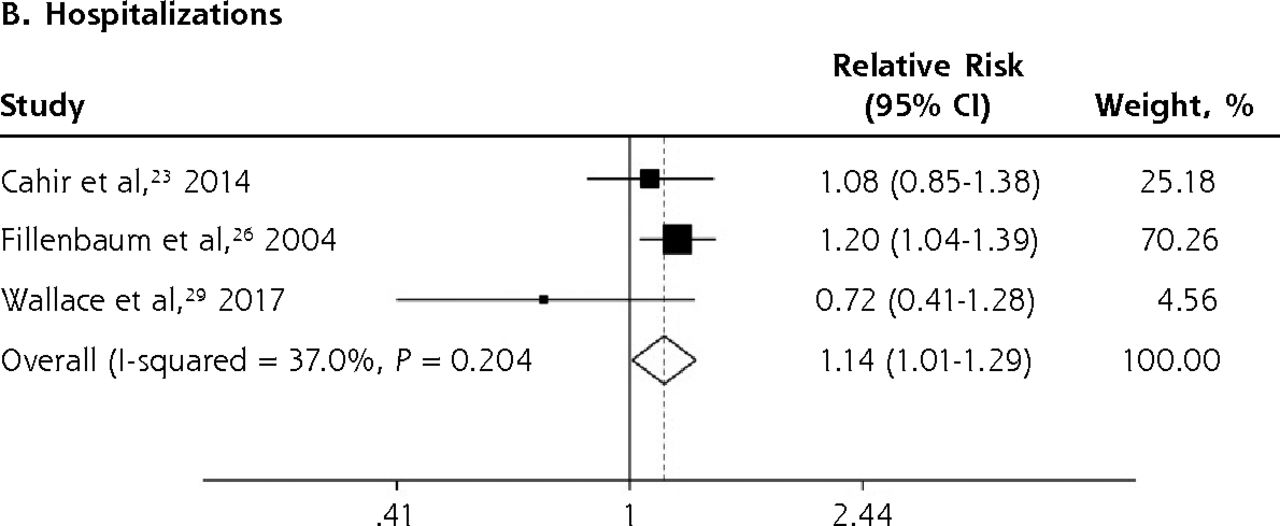
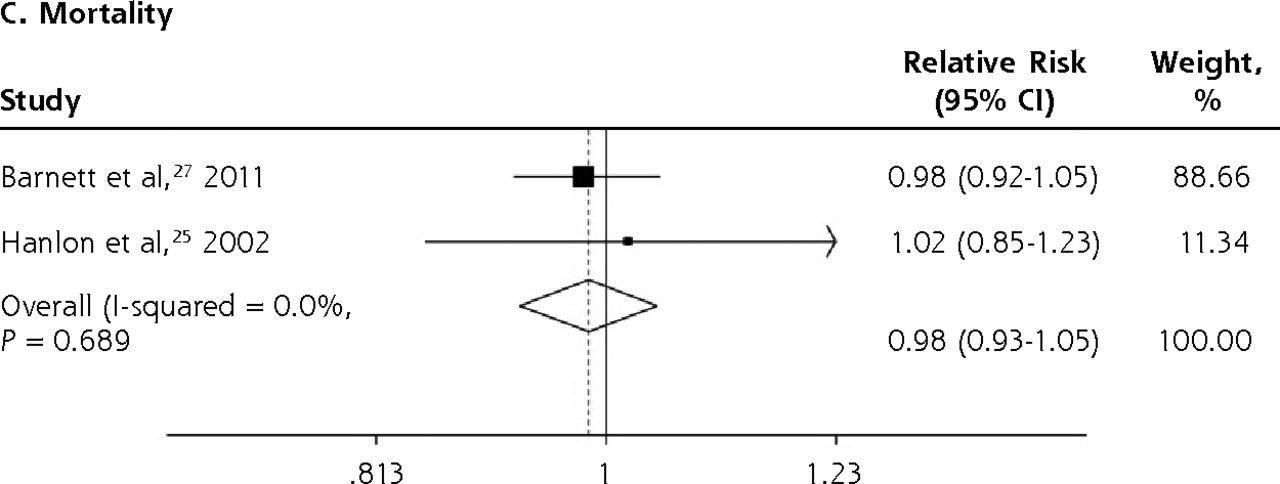
- Figure 2.
Forest plots for the adverse outcomes of potentially inappropriate prescribing based on the Beers Criteria.
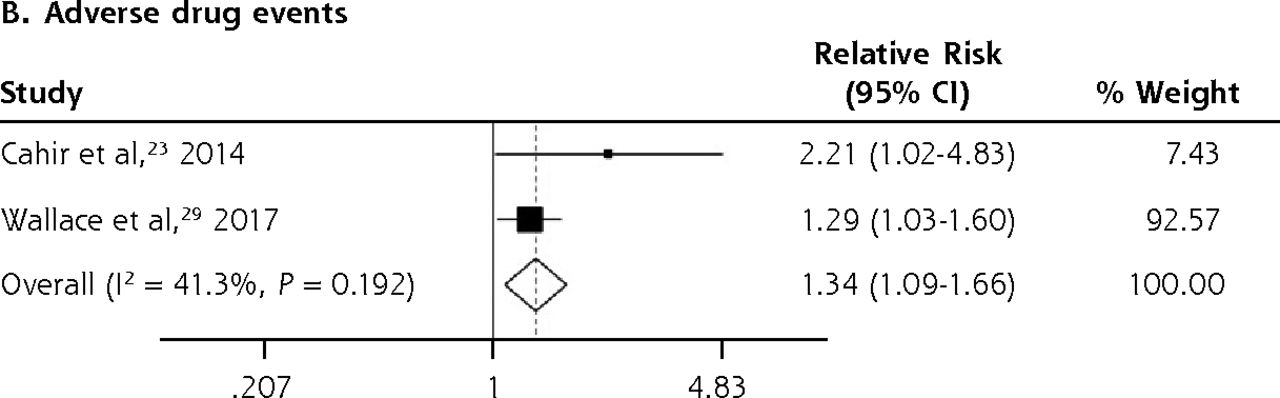
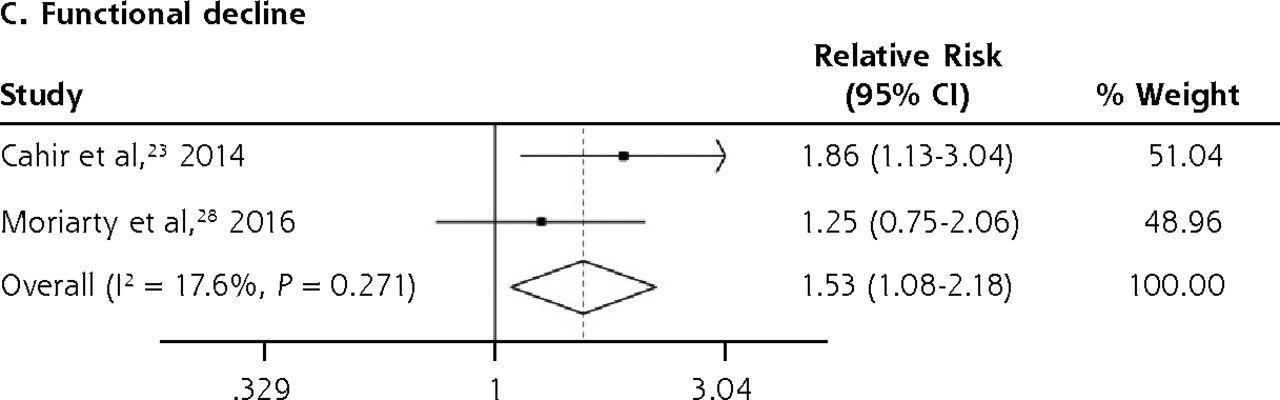
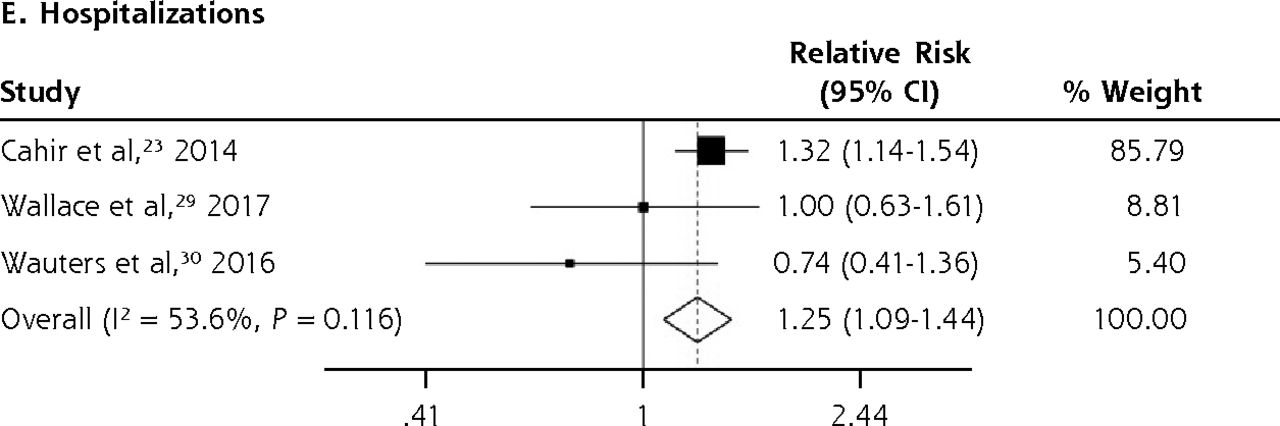
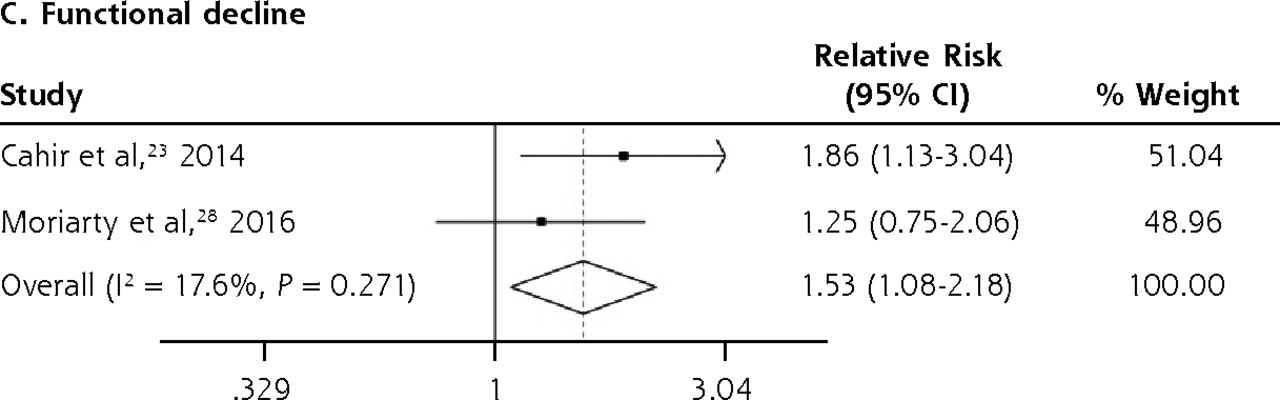
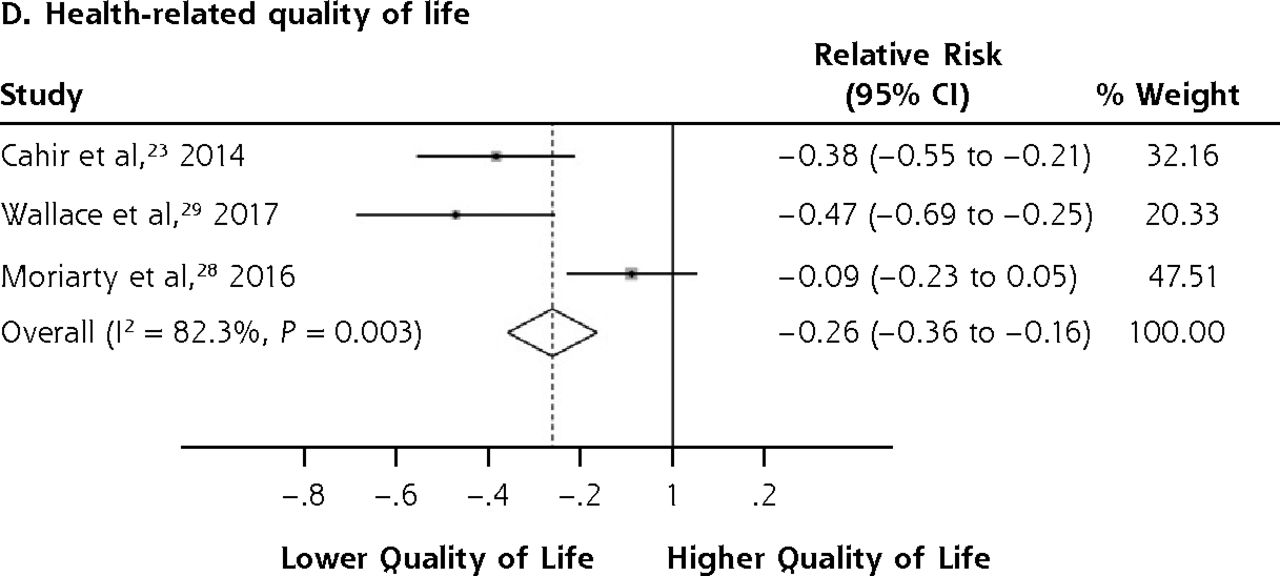
- Figure 3.
Forest plots for the adverse outcomes of potentially inappropriate prescribing based on the STOPP (Screening Tool of Older Persons’ Potentially Inappropriate Prescriptions) criteria.
A&E = accident and emergency department; HRQoL = health-related quality of life.


Tables
Risk of Bias (Newcastle-Ottawa Scale)a Author (Year) Sampling Method Sample Size Age, Years % Female Follow-Up Duration in Years Data Source of PIP Criteria of PIP Data Source of Outcomes Selection (Max 4*) Comparability (Max 2*) Outcome (Max 3*) Barnett et al,27 2011 Whole population registry 70,299 Mean 75.2
SD 6.857.0 2.0 Dispensed prescribing database Beers Criteria 2003 Mortality: Death certification database * * * * * * * * * Cahir et al,25 2014
Cahir et al,24 2014Stratified random sampling 931 Mean 78.0
SD 5.454.0 0.5 Pharmacy claim database Beers Criteria 2012
STOPPADEs, hospitalizations, and A&E visits: Structured interview and medical records
Functional decline: VES scale HRQoL: EQ-5D scale* * * * * * * * * Hanlon et al,25 2002
Fillenbaum et al,26 2004Stratified probability sampling 3,234 65-74 years: 49.1%
75-84 years: 41.1%
≥85 years: 9.8%64.8 3.0 Structured interview Beers Criteria 1997
DURMortality: National Death Index
Functional decline: Combination of Katz ADL, OARS Instrumental ADLs, and abbreviated Rosow-Breslau scale
Hospitalizations: Medicare and Medicaid database
Outpatient visits and nursing home entry: self-or proxy report* * * * * * * * * Moriarty et al,28 2016 Stratified random sampling 1,753 Mean 76.5
SD 6.054.4 1.0 Pharmacy claim database STOPP
STARTA&E visits, GP visits: Structured interview
Functional decline: Difficulty in doing 6 named ADLs HRQoL: CASP-R12 scale* * * * * * * * * Wallace et al,29 2017 Stratified random sampling 904 Median 77
IQR 74-8154.0 2.0 Pharmacy claim databases Beers Criteria 2012
STOPPADEs: Patient interview and medical records
A&E visits and hospitalizations: Medical records HRQoL: EQ-5D scale* * * * * * * * * Wauters et al,30 2016 Whole GP registry and consecutive sampling 503 Mean 84.4 61.2 1.5 Secured record STOPP
STARTMortality: Secured record
Hospitalizations: Secured record* * * * * * * * A&E = accident and emergency department; ADE = adverse drug event; ADL = activity of daily living; CASP-R12 = control, autonomy, self-realization, and pleasure revised 12-item quality of life scale; DUR = drug utilization review; EQ-5D = health-related quality of life states consisting of 5 dimensions; GP = general practitioner; HRQoL = health-related quality of life; IQR = interquartile range; OARS = Older American Resources and Service; PIP = potentially inappropriate prescribing; START = Screening Tool to Alert Right Treatment; STOPP = Screening Tool of Older Persons’ Potentially Inappropriate Prescriptions; VES = Vulnerable Elders Survey.
↵a A star (*) is awarded if a specific criterion in the Newcastle-Ottawa Scale was met, indicating low risk of bias in that criterion. Further details on the Newcastle-Ottawa Scale are available in the supplemental appendix, available at http://www.AnnFamMed.org/content/17/3/257/suppl/DC1/.
- Table 2
Covariates That Were Adjusted for in the Statistical Models of the Included Studies
Adjusted Covariate Adjusted Covariate Author (Year) Age Sex Socioeconomic status Comorbidities Number of Medications Medication Adherence Education Race Functional Status Cognitive Impairment Social Support Prior Healthcare Utilization Mental Health Condition Other Barnett et al,27 2011 ✓ ✓ ✓ – ✓ – – – – – – – – – Cahir et al,23 2014 ✓ ✓ ✓ ✓ ✓ ✓ – – – – ✓ – – Sex of the general practitioner Cahir et al,24 2014 ✓ ✓ ✓ ✓ ✓ ✓ – – – – ✓ – – Sex of the general practitioner Hanlon et al,25 2002 ✓ ✓ ✓ ✓ ✓ – ✓ ✓ ✓ ✓ – – – Body mass index Fillenbaum et al,26 2004 ✓ ✓ ✓ ✓ – – ✓ ✓ ✓ ✓ – ✓ – Marital status, insurance coverage Moriarty et al,28 2016 ✓ ✓ – ✓ ✓ – ✓ – – – ✓ ✓ ✓ Insurance coverage Wallace et al,29 2017 ✓ ✓ ✓ ✓ ✓ ✓ ✓ – – – – ✓ ✓ – Wauters et al,30 2016 – – – – ✓ – – – – – – – – – GRADE Assessment Outcomes Large Effectf/Dose Responseg Pooled Effect Size(95% CI) Certainty of Evidence GRADE Risk of Biasa Inconsistencyb Imprecisionc/Publication Biasd/Indirectnesse Large Effectf/Dose Responseg PIP based on the Beers Criteria Functional decline 4,165 RR 1.38
(1.06-1.80)●●○○○
LowNo downgrade
(NOS = 9)No downgrade
(I2 = 29.5%, P= .234)No downgrade No upgrade Hospitalizations 5,069 RR 1.14
(1.01-1.29)●●○○○
LowNo downgrade
(NOS = 9)No downgrade
(I2 = 37.0%,P = .204)No downgrade No upgrade Mortality 73,533 RR 0.98
(0.93-1.05)●●○○○
LowNo downgrade
(NOS = 9)No downgrade
(I2 = 0.0%, P = .689)No downgrade No upgrade PIP based on the STOPP criteria A&E visits 3,588 RR 1.63
(1.32-2.00)●●○○○
LowNo downgrade
(NOS = 9)No downgrade
(I2 = 0.0%, P = .452)No downgrade No upgrade ADEs 1,835 RR 1.34
(1.09-1.66)●●○○○
LowNo downgrade
(NOS = 9)No downgrade
(I2 = 41.3%, P = .192)No downgrade No upgrade Functional decline 2,684 RR 1.53
(1.08-2.18)●●○○○
LowNo downgrade
(NOS = 9)No downgrade
(I2 = 17.6%, P= .271)No downgrade No upgrade HRQoL 3,588 SMD -0.26
(−0.36 to −0.16)●○○○○
Very lowNo downgrade
(NOS = 9)Downgrade
(I2 = 82.3%, P = .003)No downgrade No upgrade Hospitalizations 2,338 RR 1.25
(1.09-1.44)●●○○○
LowNo downgrade
(NOS = 8)No downgrade
(I2 = 53.6%, P =.116)No downgrade No upgrade A&E = accident and emergency department; ADE = adverse drug event; GRADE = Grading of Recommendations, Assessment, Development and Evaluations; HRQoL = health-related quality of life; NOS = Newcastle-Ottawa Scale; PIP = potentially inappropriate prescribing; RR = relative risk; SMD = standardized mean difference; STOPP = Screening Tool of Older Persons’ Potentially Inappropriate Prescriptions.
↵a We downgraded the GRADE assessment if the risk of bias assessment based on the NOS is <8 in at least one of the studies, suggesting the presence of risk of bias.
↵b We downgraded the GRADE assessment if the Q test P < 0.10 or the I2 > 75%, indicating significantly high levels of heterogeneity in the results.
↵c For RR, we considered a clinically meaningful threshold to be 0.90 or 1.10 and downgraded the GRADE assessment if the RR point estimate is ≥1 and the lower limit of its CI is <0.90, or if the RR point estimate is <1 and the upper limit of its CI is >1.10. For SMD, we considered a clinically meaningful threshold to be ±0.20 and downgraded the GRADE assessment if the point estimate is ≥0 and the lower limit of its CI is <–0.20, or if the point estimate is <0 and the upper limit of its CI is >0.20.
↵d We could not assess for publication bias because there were <10 studies for each of the outcomes. Therefore, we did not downgrade any of the GRADE assessments due to publication bias.
↵e We downgraded the GRADE assessment if the recruited participants were not representative of older persons in the primary care settings.
↵f We upgraded the GRADE assessment if the RR is >2 or <0.5.
↵g We upgraded the GRADE assessment in the presence of dose-response gradient, which provides stronger evidence of the cause-effect relationship.
Supplemental Appendix
PDF file
Files in this Data Supplement:
The Article in Brief
Potentially Inappropriate Prescribing Among Older Persons: A Meta-Analysis of Observational Studies
Tau Ming Liew , and colleagues
Background Potentially inappropriate prescribing (the prescribing or under-prescribing of medications) is a common yet preventable medical error. This study examines whether such prescribing produces adverse outcomes in older primary care patients.
What This Study Found In older adults, inappropriate prescribing in primary care is associated with a wide range of adverse outcomes, but not mortality. An analysis of existing studies looked at potentially inappropriate prescribing in older persons that could cause significant harm. The analysis found that, although potentially inappropriate prescribing did not affect mortality, it was significantly associated with emergency room visits, adverse drug events, functional decline, health-related quality of life, and hospitalizations.
Implications
- According to the authors, the findings highlight the need to address potentially inappropriate prescribing in primary care. They call for further research into effective interventions, and they call on researchers to consider the potential implications of how potentially inappropriate prescribing is operationalized in their work.
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Optimising prescribing in older adults with multimorbidity and polypharmacy in primary care (OPTICA): cluster randomised clinical trial
- Optimizing Prescribing in Older Adults with Multimorbidity and Polypharmacy in Primary Care: A Cluster Randomized Clinical Trial (OPTICA Trial)
- Prevalence and predictors of potentially inappropriate prescribing in middle-aged adults: a repeated cross-sectional study
- In This Issue: Changing Prescriptions for Change