
Article Figures & Data
Figures
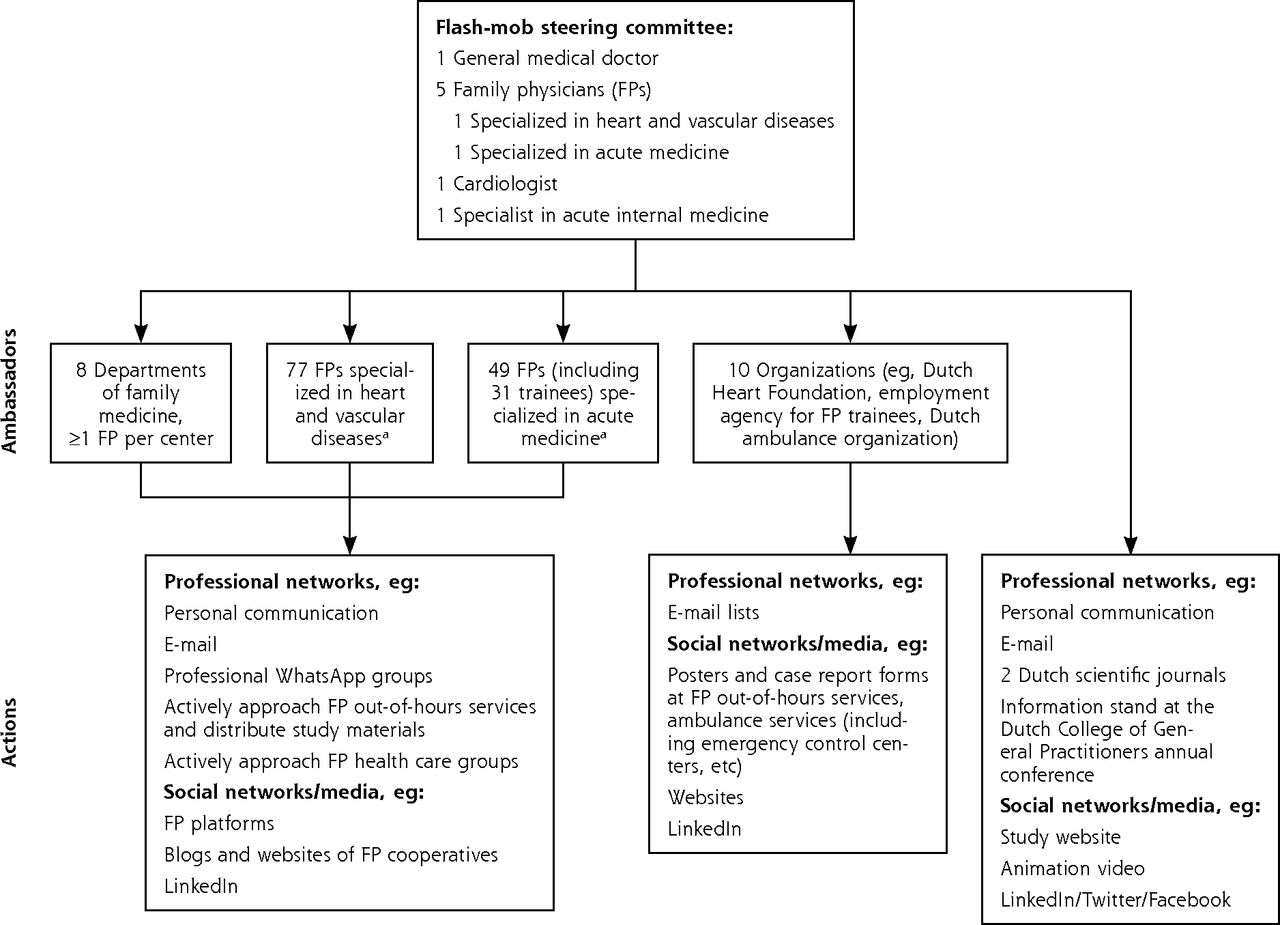
- Figure 1
Implementation of the flash-mob method in the present study.
a Specialized FPs receive a special 2-year training in heart and vascular disease or acute medicine.
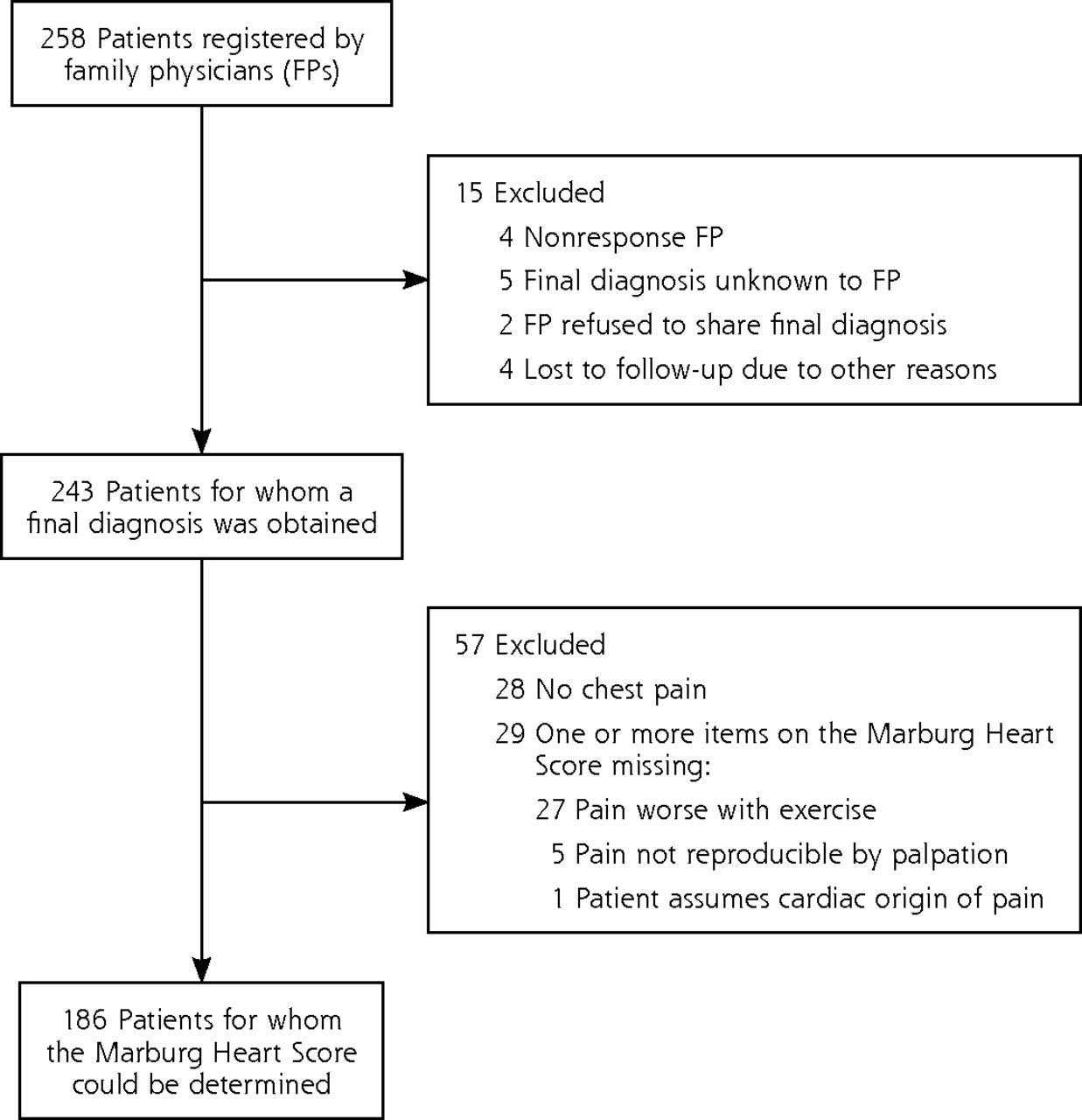
- Figure 2
Patient inclusion and follow-up.
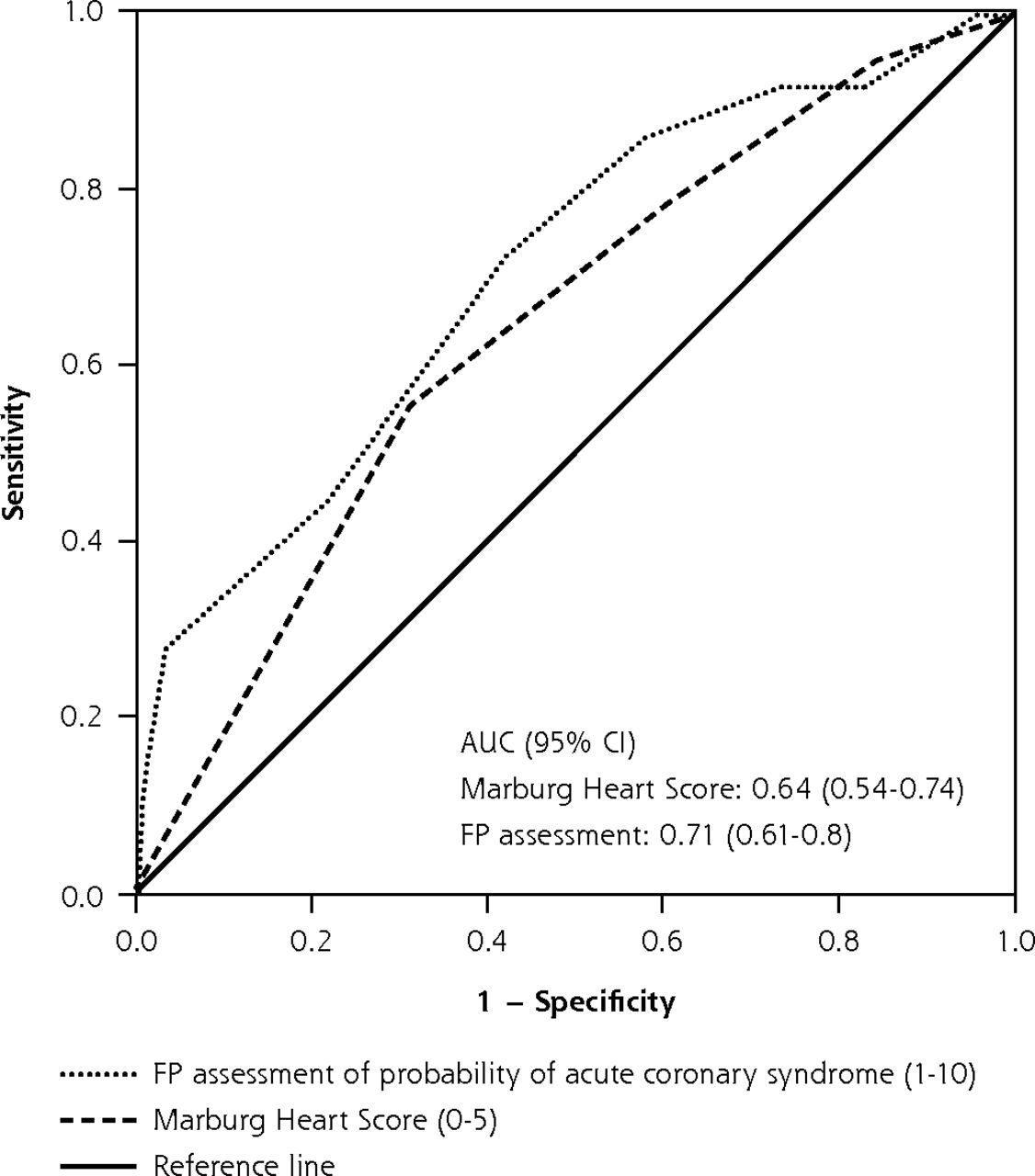
- Figure 3
ROC curves for FP assessment of ACS probability and the Marburg Heart Score in patients referred for suspected ACS (n = 186).
ACS = acute coronary syndrome; AUC = area under the curve; FP = family physician; ROC = receiver operating characteristic.


Tables
Score Component Assigned Points Age/sex (female aged ≥65 y, male aged ≥55 y) 1 Known clinical vascular diseasea 1 Patient assumes cardiac origin of pain 1 Pain worse with exercise 1 Pain not reproducible by palpation 1 ↵a Including coronary heart disease, cerebrovascular disease, or peripheral artery disease.
Note: 1 point is assigned to each score variable; 3 different risk categories are derived (low risk = 0-2 points; intermediate risk = 3 points; high risk = 4-5 points).
- Table 2
Patient Characteristics, Investigated Predictors, and Univariate Analyses of Possible ACS Predictors
Total ACS No ACS Odds Ratio (95% CI) P Value Mean age, y (SD) 64 (13.3) 67 (12.6) 63 (13.3) Male, n/N (%) 127/243 (52.3) 34/45 (75.6) 93/198 (47.0) 3.49 (1.67-7.28) <.01 Sex-adjusted age; female aged ≥65 y, male aged ≥55 y, n/N (%)a 153/243 (63.0) 36/45 (80.0) 117/198 (59.1) 2.77 (1.27-6.06) .01 Duration of symptoms, n/N (%) <1 h 23/243 (9.5) 3/45 (6.7) 20/198 (10.1) 1-24 h 138/243 (56.8) 23/45 (51.1) 115/198 (58.1) >24 h 82/243 (33.7) 19/45 (42.2) 63/198 (31.8) FP immediately suspected a serious condition, n/N (%) 120/243 (49.4) 26/45 (57.8) 94/198 (47.5) 1.51 (0.79-2.91) .21 History of clinical vascular disease, n/N (%)a 106/243 (43.6) 22/45 (48.9) 84/198 (42.4) 1.30 (0.68-2.48) .43 Patient assumes cardiac origin of pain, n/N (%)a 136/242 (56.2) 28/45 (62.2) 108/197 (54.8) 1.36 (0.70-2.64) .37 Chest pain, n/N (%) 215/243 (88.5) 39/45 (86.7) 176/198 (88.9) 0.81 (0.31-2.14) .67 Pain worse with exercise, n/N (%)a 86/188 (45.7) 17/36 (47.2) 69/152 (45.4) 1.08 (0.52-2.23) .84 Pain feels like pressure, n/N (%) 185/212 (87.3) 31/39 (79.5) 154/173 (89.0) 0.48 (0.19-1.19) .11 Pain not reproducible by palpation, n/N (%)a 179/210 (85.2) 36/39 (92.3) 143/171 (83.6) 2.35 (0.68-8.16) .17 ECG performed, n/N (%) 115/239 (48.1) 23/44 (52.3) 92/195 (47.2) ECG shows ischemic changes, n/N (%) 37/115 (32.2) 17/23 (73.9) 20/92 (21.7) 10.20 (3.55-29.28) <.01 FP assessment of ACS probability, median (IQR) 6 (3) 7 (3) 6 (3) Marburg Heart Score,b median (IQR) 3 (2) 4 (2) 3 (2) Variable ACS No ACS Total MHS using a cut-off value of ≤2 MHS >2 27 84 111 MHS ≤2 9 66 75 Total 36 150 186 Sensitivity: 75.0% (95% CI, 57.5-87.3) Incidence ACS: 19.4% (95% CI, 14.1-25.9) Specificity: 44.0% (95% CI, 36.0-52.3) Incidence No ACS: 80.6% (95% CI, 74.1-85.9) PPV: 24.3% (95% CI, 16.9-33.6) OR: 2.36 (95% CI, 1.04-5.35) NPV: 88.0% (95% CI, 78.0-94.0) χ2: 0.04 MHS using a cut-off value of ≤1 MHS >1 34 126 160 MHS ≤1 2 24 26 Total 36 150 186 Sensitivity: 94.4% (95% CI, 80.0-99.0) Incidence ACS: 19.4% (95% CI, 14.1-25.9) Specificity: 16.0% (95% CI, 10.7-23.1) Incidence No ACS: 80.6% (95% CI, 74.1-85.9) PPV: 21.3% (95% CI, 15.4-28.6) OR: 3.24 (95% CI, 0.73-14.39) NPV: 92.3% (95% CI, 73.4-98.7) χ2: 0.11 FP probability assessment using a cut-off value of ≤5 FP probability assessment high (>5) 39 116 155 FP probability assessment low (≤5) 6 82 88 Total 45 198 243 Sensitivity: 86.7% (95% CI, 72.5-94.5) Incidence ACS: 18.5% (95% CI, 14.0-24.1) Specificity: 41.4% (95% CI, 34.5-48.6) Incidence No ACS: 81.5% (95% CI, 75.9-86.0) PPV: 25.2% (95% CI, 18.7-32.9) OR: 4.60 (95% CI, 1.86-11.36) NPV: 93.2% (95% CI, 85.2-97.2) χ2: <0.01 Combined approach using the MHS and the FP assessments of probability MHS + FP probability assessment, 1-2a 36 115 151 MHS + FP probability assessment, 0b 0 35 35 Total 36 150 186 Sensitivity: 100% (95% CI, 88.0-100) Incidence ACS: 19.4% (95% CI, 14.1-25.9) Specificity: 23.3% (95% CI, 17.0-31.1) Incidence No ACS: 80.6% (95% CI, 74.1-85.9) PPV: 23.8% (95% CI, 17.5-31.6) NPV: 100% (95% CI, 87.7-100) ACS = acute coronary syndrome; FP = family physician; MHS = Marburg Heart Score; NPV = negative predictive value; OR = odds ratio; PPV = positive predictive value.
↵a Either the MHS, the FP assessment, or both were positive using an MHS cut-off value of ≤2 and an FP assessment cut-off value of ≤5.
↵b Both the MHS and the FP assessments were negative.
The Article in Brief
A Nationwide Flash-Mob Study for Suspected Acute Coronary Syndrome
Jochen W.L. Cals , and colleagues
Background The dual aim of this study was to evaluate the Marburg Heart Score, a clinical decision rule, and/or develop an adapted clinical decision rule for family practitioners to safely rule out acute coronary syndrome in patients referred to secondary care for suspected ACS; and also to evaluate the feasibility of using a "flash mob" method, an innovative new study design, for large scale research in family medicine.
What This Study Found This study finds that, in emergency care, acute coronary syndrome cannot be safely ruled out using the Marburg Heart Score or the family physicians' clinical assessment. In a period of only 2 weeks, researchers at Maastricht University collected data on 258 ACS-suspected patients by mobilizing 1 in 5 family physicians throughout the Netherlands to participate in the study. This mobilization was done by enlisting ambassadors among the FP community in the Netherlands who then spread the word through traditional professional and social networks. The study found that among 243 patients receiving a final diagnosis, 45 (18.5%) were diagnosed with acute coronary syndrome. Sensitivity for the FP rating was 86.7% and sensitivity for the MHS was 94.4%.
Implications
- While large, prospective studies can be time consuming and costly, this innovative flash mob method of research, named after the large-scale public collaborations/gatherings driven by social media, allowed for the fast investigation of one simple question on a large scale in a short timeframe.
In this issue




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Chest Pain in Primary Care: A Systematic Review of Risk Stratification Tools to Rule Out Acute Coronary Syndrome
- Ruling out acute coronary syndrome in primary care with a clinical decision rule and a capillary, high-sensitive troponin I point of care test: study protocol of a diagnostic RCT in the Netherlands (POB HELP)
- Prehospital risk assessment in patients suspected of non-ST-segment elevation acute coronary syndrome: a systematic review and meta-analysis
- Performance of risk scores for coronary artery disease: a retrospective cohort study of patients with chest pain in urgent primary care
- The Next Generation of Connectivity in Family Medicine Research