
Article Figures & Data
Figures
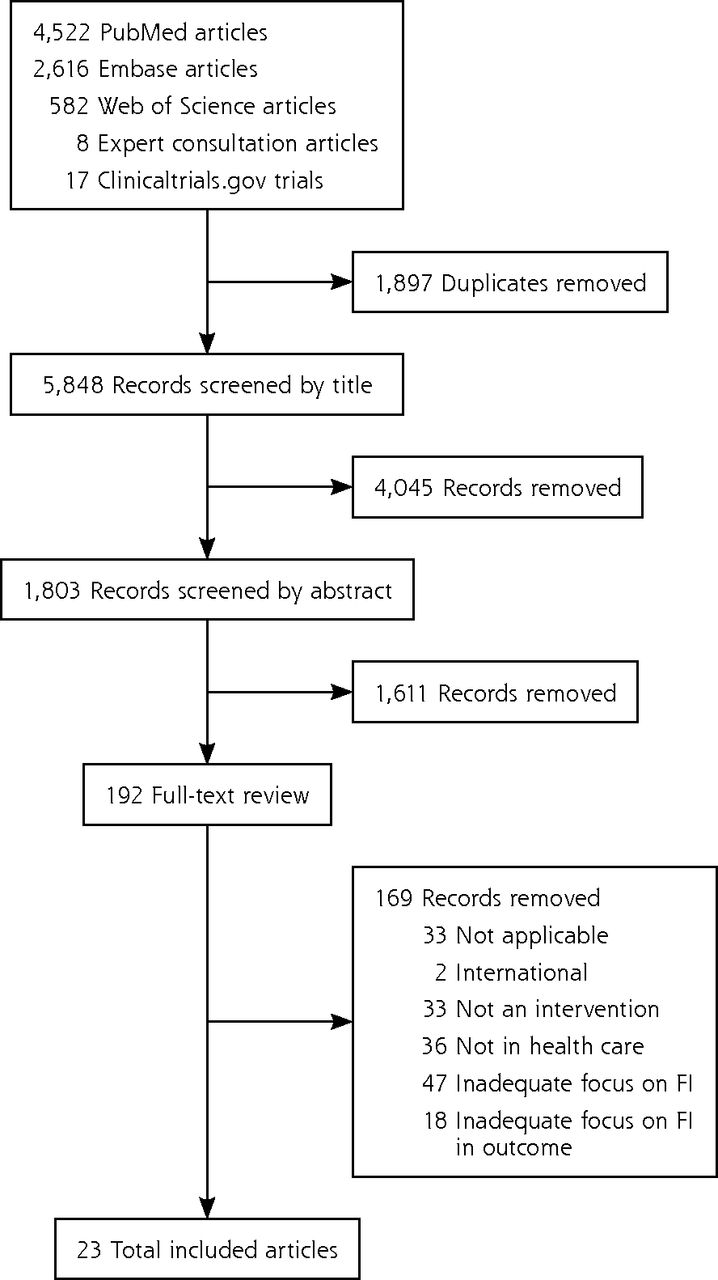
- Figure 1
Study selection flow diagram.
FI = food insecurity.
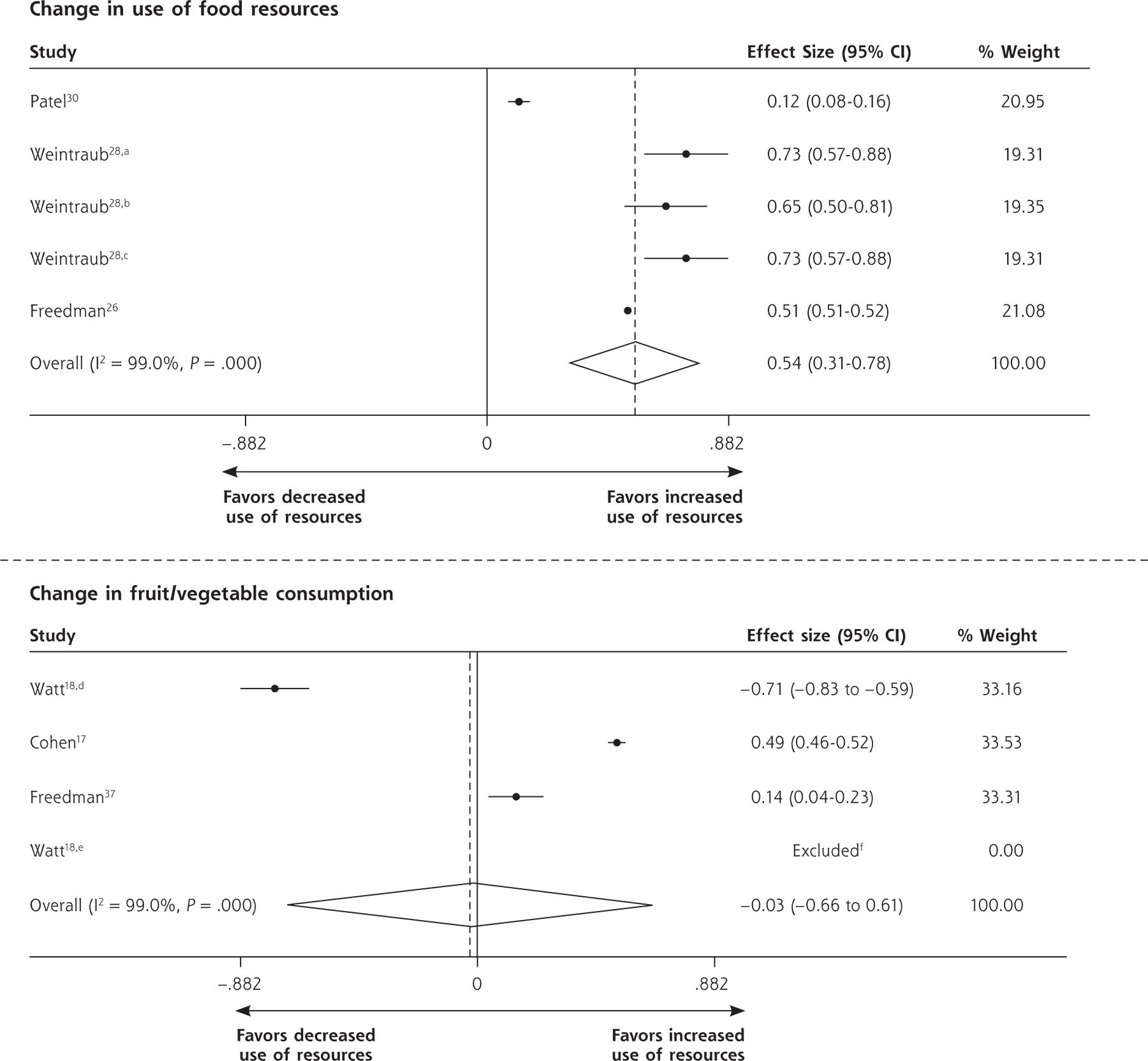
- Figure 2
Forest plots for individual and pooled SMDs by study outcomes using random effects models.
CalWORKS = Californial work opportunities and responsibilities to kids program; SMD = standard mean difference; WIC = women, infants, and children supplemental nutrition assistance program.
aChange in receipt of WIC.
bChange in receipt of CalWORKS.
cChange in receipt of food stamps.
dChange in vegetable consumption.
eChange in fruit consumption.
f95% CI and variance not calculable as mean gain for control group was zero. Note: Weights are from random effects analysis.

Tables
- Table 1
Types of Food Insecurity Interventions and Quality Scores for Included Studies (N = 23)
Study Screened for FI? Y/N (Screening Tool)a Type of Intervention Quality (GRADE) Referral Food Education & Passive Navigation & Active Food Vouchers Food Beck,31 2014 Y (2-item Hunger VS) ✔ ✔ Low Berkowitz,23 2018 N ✔ Moderate Bryce,32 2017 N ✔ ✔ Low Cavanagh,25 2017 N ✔ ✔ Moderate Cohen,17 2017 Y (1-item screener) ✔ ✔ Low Fleegler,35 2007 Y (TOA: 6-item USDA FSS) ✔ Very low Fox,29 2016 Y (2-item Hunger VS) ✔ ✔ Very low Freedman,33 2013 Y ✔ ✔ Very low Freedman,26 2014 Y (1-item screener) ✔ ✔ Low Gany,38 2015 Y (18-item USDA FSS) ✔ ✔ ✔ Very low Garg,16 2007 Y (WE CARE: 1-item screener) ✔ Moderate Garg,22 2015 Y (WE CARE: Baseline 18-item USDA FSS; F/U 1-item screener) ✔ Moderate Hassan,37 2015 Y (TOA: age specific USDA FSS) ✔ ✔ Low Knowles,34 2018 Y (2-item Hunger VS) ✔ ✔ Very low Martel,40 2018 Y (2-item Hunger VS) ✔ Very low Morales,24 2016 Y ✔ ✔ Moderate Nguyen,27 2016 N ✔ Very low Patel,30 2018 N ✔ Low Saxe-Custack,36 2018 N ✔ ✔ ✔ Very low Sege,21 2015 Y (SEEK: 2-item screener) ✔ ✔ Moderate Smith,39 2017 Y (6-item USDA FSS) ✔ ✔ ✔ b Very low Watt,18 2015 N ✔ ✔ Very low Weintraub,28 2010 N ✔ ✔ Low FI = food insecurity; F/U = follow up; GRADE = Grading Recommedations Assessment Development and Evaluation; N = no; SEEK = Safe Environment for Every Kid49; TOA = The Online Advocate (now known as HelpSteps)48; 2-item Hunger VS = 2-item Hunger Vital Sign; USDA FSS = United States Department of Agriculture-Food Security Survey; WE CARE = Well Child Care, Evaluation, Community Resources, Advocacy, Referral, Education16; Y = yes.
↵a Type of food insecurity screening tool used, if noted in manuscript.
↵b Only a subset of participants, those with diabetes mellitus, were eligible for food.
- Table 2
Process Outcomes of Interventions to Address Food Insecurity in Health Care Settings (N = 17)
Study Design Population Sample Intervention Process Outcomes Statistics Intervention type: referrals Garg,16 2007 RCT Caregivers of pediatric patients aged 2 months to 10 years at well-child visits 98 intervention, 95 control Intervention caregivers screened with 10-item questionnaire for social needs in waiting room before well-child visits Referral to food resource (pantry, foods stamps, WIC) 1.42 (0.28-2.56), 0.34a Garg,22 2015 Cluster RCT Adult caregivers of pediatric patients aged ≤6 months at well-child visits in 8 urban community health centers 336 mothers (168 per study arm) Intervention familes screened with WE CARE tool for referral to social resources Enrollment in community resources
Referral to food resourcesFood assistance program: 0.14 (–0.30 to 0.58), 0.05a
Food pantry: 0.40 (–0.38 to 1.17), 0.16a
0.67 (0.25-1.09), 0.05aFleegler,35 2007 Cross-sectional Families of children aged 0-6 years who attended well-child visits at 2 urban pediatric clinics 205 parents (68 with FI) Families screened with computer-based questionnaire for referrals to resources Referral to food resources Frequency of contacting referral agency 35% (24/68) of FI patients referred 67% (16/24) contacted food resource; 94% (15/16) deemed referral helpful Fox,29 2016 Pre-/post-intervention, pilot New patients at a pediatric weight management clinic 116 patients Intervention to partner clinic with Second Harvest Heartland food bank with SNAP enrollment outreach Enrollment in SNAP 34% (40/116) eligible for referral; 75% (30/40) accepted; 20% (3/15) completed enrollmentb Hassan,37 2015 Prospective observational Patients aged 15-25 years at an urban adolescent/young adult clinic 401 youth Web-based screening and referral tool Frequency of contacting any referral agency (not food specific) 40% (104/259) Knowles,34 2018 Mixed methods Caregivers of pediatric patients aged <5 years eligible for benefits 103 families Integrated clinic-based referral intervention Enrollment in SNAP 42% (43/103) eligible completed 85 applications; 32% (27/85) approved; 8% (7/85) denied; 60% (51/85) unknown 63% (12/19) enrolled Martel,40 2018 Retrospective observational Patients of urban county hospital/emergency department 1,519 patients Clinic parntership with Second Harvest Heartland food bank Frequency of contacting referral agency Enrollment in SNAP 74% (1,129/1,519) successfully contacted; 63% (954/1519) accepted; 92% (878/954) connected with >1 food resource 76% (338/446) of SNAP eligible completed applications Morales,24 2016 Retrospective observational cohort with propensity score matching Pregnant patients with food insecurity at obstetrical clinic 145 adult female patients Integrated screening and referral to Food for Families; program for referral to food resources Enrollment in benefits 67% (97/145) enrolled Nguyen,27 2016 Retrospective observational, pre-/post-intervention, pilot Self-identified Hispanic patients aged ≥60 years with DM, at FQHC 18/28 participants followed up at 3 months Referrals from clinic integrated Health Connector Program Frequency of contacting referral agency 33% (6/18) requested food referral; 22% (4/18) contacted food resources Patel,30 2018 Pre-/post-intervention, pilot Adult patients with DM at endocrinology clinic with access to telephone and documented financial difficulties 104 patients Financial burden resource tool Increase in use of farmers markets, groceries that accept food assistance 0.12 (–0.16 to 0.40), 0.02a Sege,21 2015 RCT Families with newborns aged <10 weeks at pediatric primary care clinic 167 intervention, 163 control Intervention group was paired with a trained family specialist who provided support (including home visits) and direct assistance accessing resources Food resource use 0.18 (–0.08 to 0.43), 0.02a Weintraub,28 2010 Prospective cohort Pediatric patients at Peninsula family advocacy program 109 participants of family advocacy program, 102 enrolled, 54 completed follow-up Integrated clinic- and hospital-based legal services Increase in use of food support WIC: 0.73 (0.18-1.28), 0.08a; CalWORKS: 0.65 (0.11-1.20), 0.08)a; Food stamps: 0.73 (0.18-0.28), 0.08a Intervention type: referrals & food Beck,31 2014 Observational Families with infants aged <1 year with FI that stretched formula or infants with failure-to-thrive at large, urban, academic pediatric primary care clinic 1,042 families Supplemental formula and educational materials for as-needed referrals were provided directly (eg, to social workers, MLP, or food pantries) Use of social resources (social work and MLP) 0.11 (0.05-0.16), <0.01a Cohen,17 2017 Quasi-experimental; pre-/post-intervention SNAP-enrolled adult primary care patients 177 patients Brief clinic-based intervention associated with increase in uptake of SNAP incentive program Double-up food bucks use Unadjusted OR 9.2 (95% CI, 6.1-13.8); Adjusted OR 19.2 (95% CI, 0.3-35.5) Freedman,26 2014 Pre-/post-intervention Adult patients of FQHCs with farmers markets 336 patients enrolled in Shop N Save (financial incentive for farmers market) Intervention to increase use of clinic-based farmers market and government food resources Farmers market revenue Use of government food assistance Increased from $14,285.60 to $15,719.73 (P <.001) Use of all forms food assistance: 0.51 (0.44-0.59), <0.01a; Senior farmers market nutrition program: 0.76 (0.65-0.86), <0.01a; SNAP: 0.64 (0.48-0.81), 0.01a Gany,38 2015 Nested cohort, observational Hospital-based food pantries at 5 cancer clinics 351 adult patients Use of hospital-based food pantry after enrollment in program Repeat use of food pantry Median return visits = 2; mean = 3.25 (SD = 3.07) Smith,39 2017 Cross-sectional Student-run free clinic 463 adult patients Integrated FI screening and intervention at free clinic Use of onsite food boxes, off-site food pantry, and SNAP enrollment 43% (201/463) receiving monthly boxes of food; 14% (66/463) using off-site food pantry; 14% (64/463) enrolled in SNAP CalWORKS = Calif. work opportunities and responsibilities to kids program; DM = diabetes mellitus; FI = food insecurity; FQHC = Federally Qualified Health Center; MLP = medical-legal partnership; OR = odds ratio; RCT = randomized controlled trial; SD = standard deviation; SMD = standardized mean difference; SNAP = supplemental nutrition assistance program; WE CARE = Well Child Care, Evaluation, Community Resources, Advocacy, Referral, Education; WIC = women, infants, and children supplemental nutrition assistance program.
↵a Statistical results for standard mean differences are shown in format with SMD, (95% CI), varience.
↵b Follow-up available for only 15 participants.
- Table 3
Non-Process Outcomes of Interventions to Address Food Insecurity in Health Care Settings (n = 11)
Study Design Population Sample Intervention or Experimental Condition Outcomes Effect Size: SMD, (95% CI), variancea Intervention type: referrals Hassan,37 2015 Prospective observational Patients aged 15-25 years at an urban adolescent/young adult clinic 401 youth Web-based screening and referral tool Food security: Complete resolution of food as priority problem 58% (7/13) Nguyen,27 2016 Retrospective observational, pre-/post-intervention, pilot Self-identified Hispanic patients aged ≥60 years with DM at FQHC 18/28 participants followed up at 3 months Referrals from clinic integrated Health Connector Program Self-efficacy: Change in mean scores on the Stanford Diabetes Self-efficacy Scale
Diabetes self-efficacyDiet/healthy eating plan: –0.14, (–0.79 to 0.51), 0.11
Physical activity: –0.07, (–0.73 to 0.58), 0.11
Diabetes self-efficacy: 0.30, (–0.35 to 0.96), 0.11
General self-efficacy: 0.13, (–0.52 to 0.79), 0.11Morales,24 2016 Retrospective observational cohort with propensity score matching Pregnant patients with FI at obstetrical clinic 145 adult female patients enrolled; 145 matched not referred Integrated screening and referral to Food for Families; program for referral to food resources Health: Blood glucose Health: SBP Health: DBP 0.10, (–0.13, to 0.33), 0.01 0.33, (0.09-0.56), 0.01 0.27 (0.04-0.51), 0.01 Intervention type: referrals & food/food vouchers Beck,31 2014 Observational Families with infants aged <1 year with FI that stretched formula or infants with failure-to-thrive at large, urban, academic primary care clinic 1,042 families with infants Supplemental formula and educational materials for as-needed referrals were provided directly (eg, to social workers, MLP, or food pantries) Utilization: Completed preventative care
Utilization: ED visitsCompleted lead test and ASQ: 0.09, (0.04-0.15), <0.01
Received full set of well-infant visits by 14 months: 0.11, (0.05-0.16), <0.01
0.11, (0.05-0.16), <0.01Bryce,32 2017 Pre-/post-intervention Adult, non-pregnant patients with type 2 DM and HbA1c >6.5 in last 3 months referred by medical provider 65 patients Voucher for fruits and vegetables, and health education/coaching at health center-based farmers market Health: Weight change Health: SBP change Health: DBP change Health: Drop in HbA1c –0.08, (–0.30 to 0.13), 0.01 –0.04, (–0.26 to 0.17), 0.01 0.15, (–0.06 to 0.37), 0.01 0.39, (0.17-0.60), 0.01 Cavanagh,25 2017 Retrospective matched cohort; pre-/post-intervention Adult low-income patients with obesity, hypertension, and/or type 2 DM 54 intervention, 54 matched controls Voucher (prescription coupon) for weekly mobile produce market Health: BMI change –0.11, (–0.18 to –0.05), <0.01 Cohen,17 2017 Quasi-experimental, pre-/post-intervention SNAP-enrolled adult primary care patients 177 patients Brief clinic-based intervention associated with increase in use of SNAP incentive program Health behavior: Increased fruits/vegetable consumptionb 0.49, (0.25-0.73), 0.01 Freedman,33 2013 Pre-/post-intervention, pilot Adult patients of FQHCs with farmers markets with DM 41 patients Community-based participatory research approach for onsite farmers market; financial incentive program to purchase food at market Health behavior: Increased fruits/vegetable consumptionc 0.41, (–0.02 to 0.85), 0.05 at 2-3 months 0.15, (–0.28 to 0.58), 0.05 at 5 months Saxe-Custak,36 2018 Qualitative Adult caregivers of pediatric patients at an urban pediatric clinic 32 caregivers Provided vouchers for farmers market or bag of food when market closed; cooking/nutrition classes Acceptability
Health behavior: Increased fruits/vegetable consumption
Food securityAppreciated convenience of clinic within farmers market building
Preferred prescription vouchers over food bags Reported increased
Improved food security and access to healthy foodsWatt,18 2015 Quasi-experimental prospective Adult Hispanic pregnant women at low-income Texas primary care clinic 32 intervention, 29 control Prenatal care-based nutrition education, food resources education, and farmers market vouchers Health behavior: Increased fruits/vegetable consumptiond
Health: Depression (mean gain PHQ2 score)
Health: Excess maternal weight gain Health: Breastfeeding at age 6 months
Health: Pass ASQ screeningFruits: d = 0.47e,f
Vegetables: –0.71, (-1.19 to -0.22), 0.06 d-0.34,(–0.91 to 0.22), 0.08f
–0.19, (–0.80 to 0.41), 0.09
0.64, (–0.06 to 1.34), 0.13
0.71, (–0.05 to 1.48), 0.15Intervention type: food only Berkowitz,23 2018 Matched cohort Adult patients with dual Medicaid/Medicare eligibility; members of Common-wealth Care Alliance Medically tailored meals program: 133 intervention, 1,002 matched controls. Nontailored food program: 624 intervention, 1,318 matched controls Provided food: impact of medically tailored meal delivery and Meals on Wheels Utilization: ED visits, inpatient admissions, use of ET
Cost: Medical spendingMedically tailored: ED visits: –0.26, (–0.4 to –0.10), 0.01; Inpatient admissions: –0.09, (–0.27 to 0.09), 0.01; Use of ET: –0.15, (–0.34 to 0.03), 0.01
Non-medically tailored: ED visits: –0.15, (–0.25 to –0.06), <0.01; Inpatient admissions: –0.03, (–0.13 to 0.06), <0.01; Use of ET: –0.07, (–0.17 to 0.02), <0.02
Medically tailored: lower medical spending; net savings $220 per participant
Nontailored: lower medical spending: Net savings $10 per participantASQ = Ages and Stages Questionnaire; BMI = body mass index; DBP = diastolic blood pressure; DM = diabetes mellitus; ED = emergency department; ET = emergency transportation; FI = food insecurity; FQHC = Federally Qualified Health Center; HbA1c = glycated hemoglobin; MLP = medical-legal partnership; PHQ2 = Patient Health Questionnaire-2; SBP = systolic blood pressure; SMD = standard mean differences; SNAP = supplemental nutrituion assistance program.
↵a Effect sizes are presented as standardized mean differences (d) unless sufficient alternatives were provided in the reviewed manuscripts (eg, Odds Ratios [ORs]). Effect sizes were not calculated when a plausible control/comparison group was not available to compare with the intervention group and/or if insufficient details were provided in the manuscript and we did not receive responses to requests for further information from study authors.
↵b Increase in fruit/vegetable consumption (servings/day) at 5-month follow-up (n = 138).
↵c Servings/day.
↵d Reported as change from less than 3 servings to 3 or more servings per day; raw data unavailable to adjust results to report as servings per day, as would need to adjust standard deviation.
e 95% CI and varience not calculable as mean gain for control group = 0.
↵F Author provided additional data points to enable effect size calculation.
Supplemental Appendixes
Supplemental appendixes
Files in this Data Supplement:
- Supplemental data: Appendixes - PDF file
The Article in Brief
Interventions Addressing Food Insecurity in Health Care Settings: A Systematic Review
Emilia De Marchis , and colleagues
Background Many health care settings are exploring ways to address social determinants of health, including the reduction of patient food insecurity. Health systems have begun experimenting with providing interventions to address food insecurity as a strategy to improve health; however, the impacts of such interventions on food security, patient health and health behaviors, and health care utilization and cost are unclear.
What This Study Found A systematic review of articles covering food insecurity interventions in health care settings from 2000-2018 found that interventions that included either referrals or direct provision of food or vouchers both suffered from poor follow-up, a general lack of comparison groups, and limited statistical power and generalizability. Of the twenty-three studies included in analysis, 74% were rated low or very low quality. In studies of referral-based interventions, there were moderate increases in process outcome--like food program referrals (Standardized Mean Differences: 0.67 95% CI 0.36 to 0.98; 1.42 95% CI 0.76 to 2.08) and resource use (pooled SMD: 0.54 95% CI 0.31 to 0.78). In studies of direct food or voucher interventions, outcomes were mixed, with changes in fruit and vegetable intake averaging to no impact when pooled (-0.03 95% CI -0.66 to 0.61). Studies were limited in their evaluation of health or utilization outcomes, with generally small but positive effects.
Implications
- This review revealed limitations in growing literature on health care-based food insecurity interventions. Low quality and lack of studies examining health or health care outcomes limit inferences about their impacts. More rigorous evaluation of food insecurity interventions is needed that includes health and utilization outcomes to better understand roles for the health care sector in addressing food insecurity.
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Clusters of Health-Related Social Needs Among Adult Primary Care Patients
- Doctors have an ethical obligation to ask patients about food insecurity: what is stopping us?
- Mise en œuvre dinterventions sociales en soins de sante primaires
- Implementing social interventions in primary care
- Utilization Patterns of a Food Referral Program: Findings from the Mid-Ohio Farmacy
- Food Insecurity Is an Independent Risk Factor for Depressive Symptoms in Survivors of Digestive Cancers
- Does the effect of lifestyle intervention for individuals with diabetes vary by food insecurity status? A preplanned subgroup analysis of the REAL HEALTH randomized clinical trial
- Do Patients Want Help Addressing Social Risks?