
Abstract
PURPOSE We describe the results of a practice transformation project conducted within a national cohort of optometry practices participating in the Southern New England Practice Transformation Network.
METHODS Participants were 2,997 optometrists in 1,706 practices in 50 states. The multicomponent intervention entailed curriculum dissemination through a preexisting network of optometrists supported by specialized staff and resources, and data collection through a web portal providing real-time feedback. Outcomes included practices reporting data, urgent optometry visits for target conditions, and projected cost savings achieved by reducing emergency department (ED) use through increased provision of urgent care for conditions amenable to management in optometry practices.
RESULTS Over 13 months, 69.9% of practices reported data for a mean of 6.7 months. Beginning with the fourth month, the number of urgent optometry visits increased steadily. Among reporting practices, the total cost savings were estimated at $152 million (176,703 ED visits avoided at an average cost differential of $860 per visit). Monthly projected cost savings per optometrist were substantially greater in rural vs urban practices ($10,800 vs $7,870; P <.001).
CONCLUSIONS Technical assistance to promote practice transformation can be provided remotely and at scale at low per-practice cost. Through the provision of timely, easily accessed ambulatory care, optometrists can improve the patient experience and reduce ED use, thereby reducing costs. The cost savings opportunities are immense because of the large volume and high expense of ED visits for ocular conditions that might otherwise be managed in ambulatory optometry practices.
- optometry
- practice transformation
- health care utilization
- urgent care
- cost savings
- quality improvement
- health information technology
- practice-based research
INTRODUCTION
Over the past 15 years, practice transformation programs and initiatives have become increasingly common and largely if not exclusively directed toward primary care practices. Other clinical specialists, such as optometrists, however, have not been specifically invited to participate in such efforts. Meanwhile, there is increasing pressure for all health care professionals to deliver value-based care, and in 2015, the Centers for Medicare & Medicaid Services (CMS) sought to promote inclusivity through the creation and funding of the Transforming Clinical Practices Initiative (TCPI).1 This program funded 29 Practice Transformation Networks (PTNs) and challenged them to engage more than 140,000 clinicians in practice transformation activities that would prepare them to succeed in an evolving practice environment that emphasizes value-based care, population health, and patient and family engagement. CMS promoted the participation of many types of clinicians, and there were numerous reasons to include optometrists.
Healthy People 2020 articulates a goal to improve the visual health of the nation through prevention, early detection, treatment, and rehabilitation.2 In 3,500 of the 6,500 communities in the United States where optometrists practice, they are the only eye care health professionals.3 Access is noted to be an important constraint to the goals set forth by the US Department of Health and Human Services.
Unfortunately, the competence and efficiency of optometrists over a broad scope of care is often undervalued, even by clinical colleagues, such as primary care physicians (PCPs).4 Optometry practices tend to operate as small businesses, and with a growing push toward consolidation into larger systems, the advent of the CMS Quality Payment Program, and the creation of Accountable Care Organizations, many optometrists feel vulnerable in this rapidly evolving market.
Like many clinical specialists, optometrists focus on a single function and body area, namely, vision and the eyes. At times, they are the first clinician to identify a condition that reaches well beyond the eyes, such as diabetes or hypertension. Because of their broad geographic distribution, it seems likely that interventions with optometrists at scale could have a considerable impact on the experience, cost, and quality of health care.
We report results of a multicomponent practice transformation and quality improvement (QI) intervention among optometry practices enrolled in the Southern New England Practice Transformation Network (SNE-PTN), as part of TCPI. Mindful of the triple aim (better care, better population health, and lower costs), we sought to increase diabetic retinopathy screening rates and to improve use of optometry practices by patients with urgent eye conditions, thereby reducing the total cost of care. As optometrists provide the only source of specialized vision care in more than one-half of the communities in which they practice,3 we sought to compare cost savings in urban vs rural locations. Herein we describe the process of practice transformation conducted remotely and at scale, and the results of the cost-savings efforts.
METHODS
Participants
We invited a large group of optometrists to participate in TCPI through SNE-PTN. The opportunity to participate in a large-scale, highly visible CMS program designed to prepare clinicians for success under future payment models appealed to optometrists, and initially, 4,108 optometrists (working in 2,426 practices), almost all of whom participate in a single network of private practices (Vision Source), enrolled. Participating practices receive CMS-funded technical assistance, delivered at no cost to the practices. Practices that failed to engage with SNE-PTN by submitting a transformation plan were eventually disenrolled. These practices are excluded from this report, which includes 2,997 optometrists working in 1,706 practices distributed across all 50 states.
Intervention Design
Our approach was informed by the elements identified as essential for strategic improvement by the Institute for Healthcare Improvement: will, ideas, and execution.5 Optometrists are trained to provide thorough and complete care (exclusive of major surgery) for most eye conditions. To increase value, we worked with enrolled optometry practices to promote provision of urgent eye care to reduce use of health care in more expensive settings such as emergency departments (EDs) of hospitals. This goal aligns strongly with TCPI aims, which include reduction of hospital use and generation of cost savings.
Within SNE-PTN, we have developed extensive knowledge, experience, and capacity to facilitate practice transformation with local practices, that is, those geographically proximate to our staff. We trained and deployed a workforce of quality improvement advisors (QIAs), who consult with practices and guide them through standard QI methods, such as assessing practices, establishing goals, and implementing iterative plan-do-study-act (PDSA) cycles to achieve data-driven improvement.
We promoted a networkwide transformation agenda that focused on diabetic eye examinations and ED avoidance with our national optometry cohort. Acute eye conditions that are amenable to evaluation and management in an ambulatory optometry practice and are commonly seen in hospital EDs (eg, conjunctivitis, hordeolum, corneal abrasion) were identified through a process of consultation with leaders in optometry. Working with a small number of engaged local optometrists, we developed protocols and tools for promoting and tracking the provision of ambulatory care for such conditions and pilot-tested the approach.
The goal of achieving practice transformation with 1,706 optometry practices in all 50 states with an average practice size of 1.8 clinicians presented substantial challenges with respect to communication, engagement, and reporting. To address these challenges, we developed and adopted the methods listed in Table 1. Best-practice protocols for ED avoidance included techniques for tracking urgent care episodes, interventions to increase urgent care capacity (open scheduling and implementation or expansion of after-hours/on-call availability and triage services) and informing patients of urgent care availability within the practice (education of staff and patients, supported by marketing and educational materials developed by SNE-PTN). The data portal featured enhanced functionality, including the ability to automatically remind practices to submit data, query them on their progress, and provide real-time feedback, including run charts and progress reports. This multicomponent intervention was initiated in October 2017.
Components of the SNE-PTN Transformation Intervention
Measures and Data Collection
Urgent care optometry visits for the target conditions were logged by staff in each optometry office. Beginning in October 2017, the number of such services provided were reported through our data portal. Each such visit was considered to represent an avoided ED visit.
Average cost savings per ED visit avoided ($860) were calculated by subtracting the cost of office-based care from the ED-associated costs, weighted by frequency and cost per condition according to previous reports (Table 2).6–8 Costs of medications and follow-up examinations were excluded from the calculation of average cost.
Weighted Average Cost Savings for Ambulatory Optometry Visits vs ED Visits for Common, Nonemergent Eye Conditions
Data Analysis
Practices were stratified into urban and rural locations using a national data set of ZIP+4 codes provided by the Health Resources and Services Administration.9 Monthly cost savings were computed for each practice using the previously noted methodology, and results were stratified from least to most savings for urban and rural practices, respectively. We aggregated practices in each setting into deciles (bottom 10% to top 10% of savings) and calculated the mean cost savings of each decile to visualize the difference between urban and rural practices across performance levels. Cost savings were compared between rural and urban settings, and a P value was calculated using a 2-tailed t test assuming unequal variances in Excel version 1812 (Microsoft Corp).
RESULTS
A total of 2,997 optometrists working in 1,706 practices in all 50 states were enrolled to participate in the SNE-PTN. By location, 1,131 practices (66.3%) were classified as urban and 575 were classified as rural. Nearly all were organized in small private practices that are members of a national network.
From October 2017 through October 2018, a total of 1,193 practices (69.9%) reported ED avoidance data for a mean of 6.72 ± 4.41 months (95% CI, 6.49-6.96 months). Calculated total cost savings were $152 million (176,703 ED visits avoided at a weighted average cost of $860 per visit) over 13 months, an average monthly savings of more than $11.6 million.
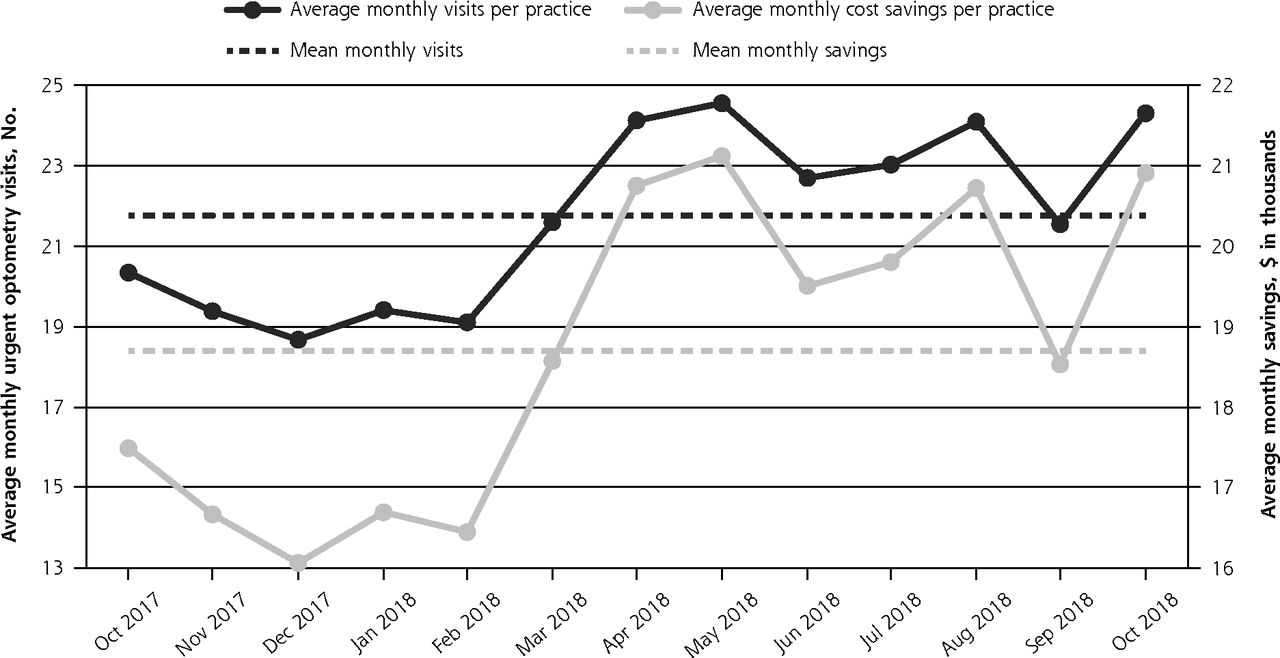
Sustained improvement trends were observed over many months for the process measure of practices reporting (Figure 1) and the outcome measures of urgent visits provided and cost savings projected (Figure 2). After the first few months, substantial rises in the rates of urgent visits provided and cost savings per reporting practice were observed, and these improvements have been sustained over time (Figure 3).
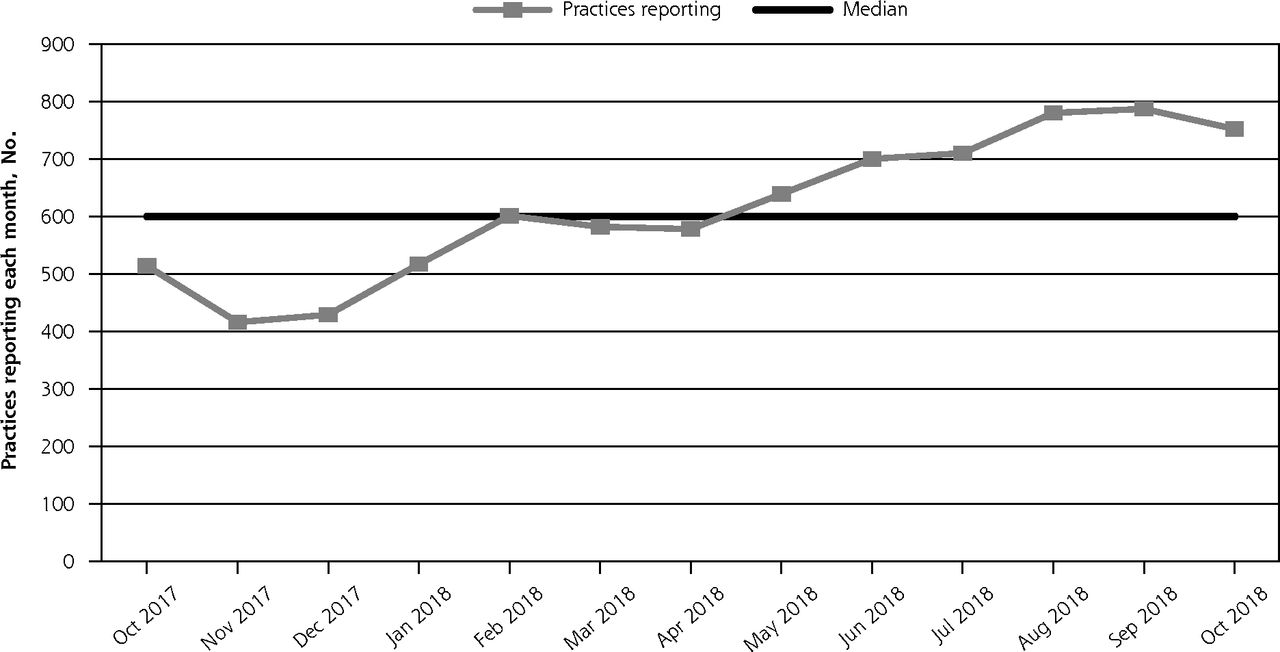
Practices reporting ED avoidance data, per month.
ED = emergency department.
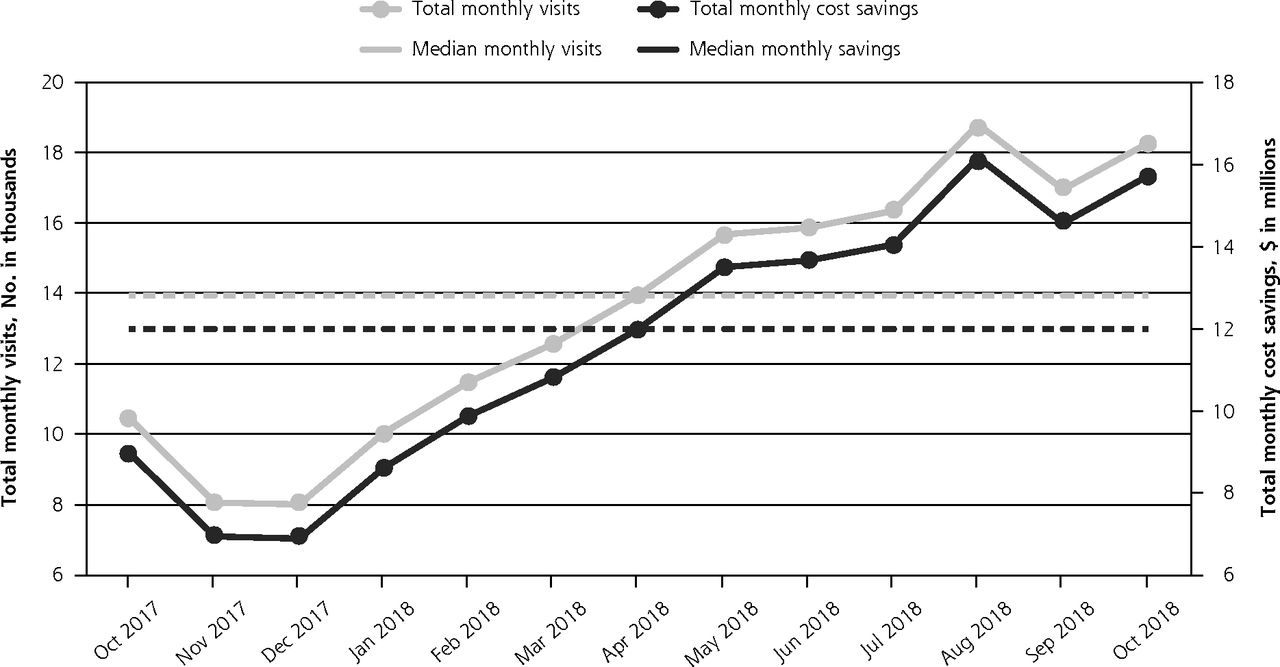
Total monthly visits and cost savings reported.

Average monthly urgent optometry visits and cost savings per practice.
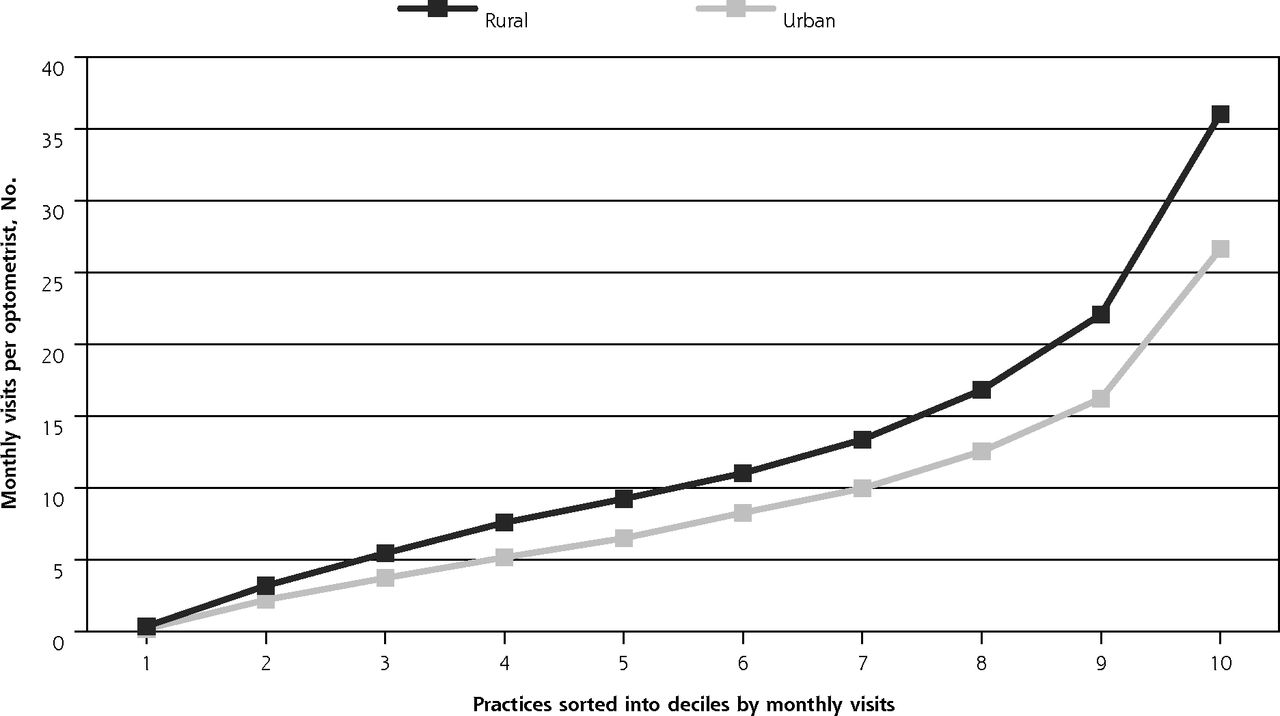
On average, there were 10.36 monthly visits per optometrist. Analysis by practice setting revealed a higher rate among those in rural settings (12.56 ± 10.53 visits, 95% CI, 11.55-13.56) compared with urban settings (9.15 ± 8.06 visits, 95% CI, 8.58-9.72) (P <.001) and a corresponding difference in cost savings between the rural group ($10,800 ± $9,054; 95% CI, $9,933-$11,666) and the urban group ($7,870 ± $6,932; 95% CI, $7,380-$8,360 (P <.001). This difference was present at nearly all performance levels (Figure 4).

Average monthly visits per ever-reporting optometrist by practice setting.
DISCUSSION
Key Findings
Our experience with this group of optometry practices reveals important lessons for PCPs, many of whom fail to appreciate the breadth and depth of services provided by optometrists.4 Because optometrists are so widely distributed, often located in rural areas, they represent an ideal health care workforce for collaboration with PCPs, who may underuse optometrists within their referral networks.
The cost savings suggested in this report (more than $152 million) are remarkably large, especially when considering the relatively brief time frame and incomplete practice engagement, with only 69.9% of enrolled practices reporting on this measure. Clearly, a key driver of cost savings is the large cost discrepancy between managing acute eye conditions in EDs as opposed to optometry offices. This finding underscores the wisdom from CMS to reduce hospital use as a specific aim of TCPI. National data indicate that ED management of nonemergent eye conditions is remarkably common and costly. We acquired ED use data from the Healthcare Cost and Utilization Project’s (H-CUP) National Emergency Department Samples from 2014 through 2016 (the most recent years available). These data confirm that the 6 ambulatory-sensitive ocular conditions selected for reporting in this project are commonly treated in EDs across the country.10 The 2015 data set, extrapolated from its sampling frame, indicates that there were more than 1.2 million ED visits in which the 6 selected conditions were the primary diagnosis, representing more than $1.2 billion in paid claims. The average claims cost in this data set was $977. This amount correlates well with the cost savings in the present project: $860, after subtracting the cost of ambulatory care provided by the optometrist.
The marked difference in cost savings between rural and urban settings likely reflects easier access to EDs for patients in urban settings. We postulate that with greater challenges accessing hospital care in rural areas, patients are more willing to wait until the optometry office reopens.
Optometrists in our project implemented practice-level protocols and provided and reported increasing numbers of urgent care services for ocular conditions that are often managed in more expensive, less efficient settings. Many other clinician types could replicate this ED avoidance approach, namely, increase practice capacity to provide urgent care, educate and inform patients that this service is available for a specified scope of urgent problems, and then track the number of such visits provided. The proof of concept provided here may inspire practices to increase such efforts and to promote the virtues of such work in value-based payment environments.
To address some of the logistic challenges inherent to providing practice transformation support remotely and at scale, we prioritized our focused efforts on cost savings produced through ED avoidance. In a conventional on-site practice-coaching model, each QIA would manage a panel of 10 to 20 practices. To accommodate the scale of this project, the ratio was 200 to 250 practices per coach; therefore, direct, on-site contact with every clinician or practice was impossible. To address this potential gap, we leveraged the existing leadership of the partner optometry organization and relied on remote communication strategies, such as e-mail, webinars, newsletters, and interactive digital tools. We also created a secure portal to facilitate remote data submission. As a result of the above approach, the transformation support cost per practice was substantially lower than that in most practice transformation programs, which tend to be smaller scale and geographically localized, and to emphasize greater on-site activities.
At nearly every stage, we encountered the well-known diffusion of innovations theory, first described in 1962.11 We gained initial traction with the innovators and early adopters, but struggled to engage others, despite their expressed will to pursue practice transformation. This phenomenon has been well described in other practice transformation programs,12 and we observed it in our initiative. Funding limitations did not permit a rigorous evaluation of rates of diffusion or factors associated with those rates.
Although we have not directly demonstrated so, it seems likely that other types of clinicians could achieve successful practice transformation through the application of similar interventions, especially when there is an infrastructure that can facilitate data management and dissemination of proven protocols. Within our PTN, for example, physical therapists and dentists have expressed interest.
A wide variety of organization types, including regional or national specialty associations, commercial networks, and independent practice associations, could provide the infrastructure for dissemination of protocols and best practices and for data management. Leveraging the power of professional group identity and the attendant expectations can promote engagement and performance. Organizations that strive to promote practice transformation should consider identifying such opportunities and collaborating with appropriate clinical partners. Similarly, clinical entities, professional associations, and professional societies with practice transformation needs should consider partnering with organizations capable of providing technical assistance and practice transformation support remotely and at scale.
Limitations
Our work was designed and funded as a practice transformation and QI enterprise, not as a research study. We therefore did not identify a control group, and we allowed practices considerable latitude in the timing of the implementation of interventions and initiation of data reporting, so we cannot report on baseline data or preintervention-postintervention comparisons.
The cost savings we report were not directly measured, but rather calculated from practice-reported volume data and published estimates of the cost of care. We did not account for several factors in our cost savings calculations; if accounted for, some of these factors would diminish the calculated cost savings, whereas others would amplify them. Our analysis of the H-CUP data validates quite precisely our estimate of the average paid cost of an eye care visit rendered in an ED.
We have assumed in our calculations that patients seen for urgent eye conditions in the offices of optometrists would have alternatively sought care in hospital EDs. In fact, it seems likely that in some cases, if the optometrist were not available, patients may have chosen to not seek care at all; when true, this would mean that an urgent office visit did not actually avoid an ED visit, and may in fact have increased costs. We are not able to determine the frequency with which this behavior may have occurred. In a study of retail clinics, 58% of retail clinic visits for low-acuity conditions represented additional use rather than avoidance of ED visits.13 We do not believe that the same phenomenon occurred at substantial frequency in our optometry practices because the urgent care provided occurred only after patients communicated with the practice. This communication typically led to a process in which patients were triaged to the ED, an urgent ambulatory optometry visit, or home-based care without any health care professional visit. The last category achieves even more substantial cost savings but was not captured by our methods. Because of the triage process, urgent optometry office visits were more likely to represent indicated care than patients presenting to retail clinics on self-referral for low-acuity conditions.
Finally, our formula for calculating cost differences did not account for the common scenario in which ED visits are concluded with advice to the patient to follow-up with their PCP or eye doctor. Including this and other downstream costs associated with many ED visits would substantially amplify the cost savings realized.
Conclusions
Given appropriate circumstances, technical assistance to promote practice transformation can be provided remotely and at scale at relatively low per-practice costs. Through the provision of timely, easily accessed ambulatory care, optometrists can improve the patient experience and reduce ED use, thereby reducing costs for ambulatory-sensitive ocular conditions. The cost savings opportunities are immense because of the large volume and high expense of ED visits for ocular conditions that might otherwise be managed in ambulatory optometry practices. Because optometrists are widely distributed, including in underserved areas, and provide timely and cost-effective care for acute ocular conditions, they can be valued members of a comprehensive care team, whether in an Accountable Care Organization or a medical neighborhood.
Acknowledgment
The authors would like to thank Sai Cherala, MD for her contributions to establishing the cost estimate for avoided ED visits.
Footnotes
Conflicts of interest: authors report none.
To read or post commentaries in response to this article, see it online at http://www.AnnFamMed.org/content/17/Suppl_1/S33.
Funding support: The quality improvement work described herein was supported by CMS.
Disclaimer: The views expressed are those of the authors.
- Received for publication August 31, 2018.
- Revision received January 23, 2019.
- Accepted for publication February 27, 2019.
- © 2019 Annals of Family Medicine, Inc.




{kind=link}
{kind=link}
{kind=link}
{kind=link}