
Article Figures & Data
Figures
- Figure 1.
Description of identified buprenorphine care delivery models.
NCM = nurse care manager; OBOT = office-based opioid treatment.
- Figure 2.
Differences in long-term (after Year 1) minimum net revenue increase with variations in the no-show rate for induction and maintenance, across practice types and alternative approaches for office-based opioid treatment with buprenorphine.
FQHC = federally qualified health center; MD = medical doctor; OBOT-B = office-based opioid treatment with buprenorphine; RN = registered nurse; SH = shared; SO=solo.
Note: Results take into account variation in prevalence of opioid use disorder among different practice types. These terms were defined as follows: FQHC: federally qualified health centers and look-alikes; Urban: non-FQHC in high-poverty urban ZIP Code (≥20% of households below poverty threshold); Rural: non-FQHC in high-poverty rural ZIP Code (≥20% of households below poverty threshold); Other: practice in lower-poverty ZIP Code; MD: OBOT-B with physician-led visits4; RN: OBOT-B with nurse-led visits28; SH: OBOT-B with shared visits28; SO: OBOT-B with solo provider30.
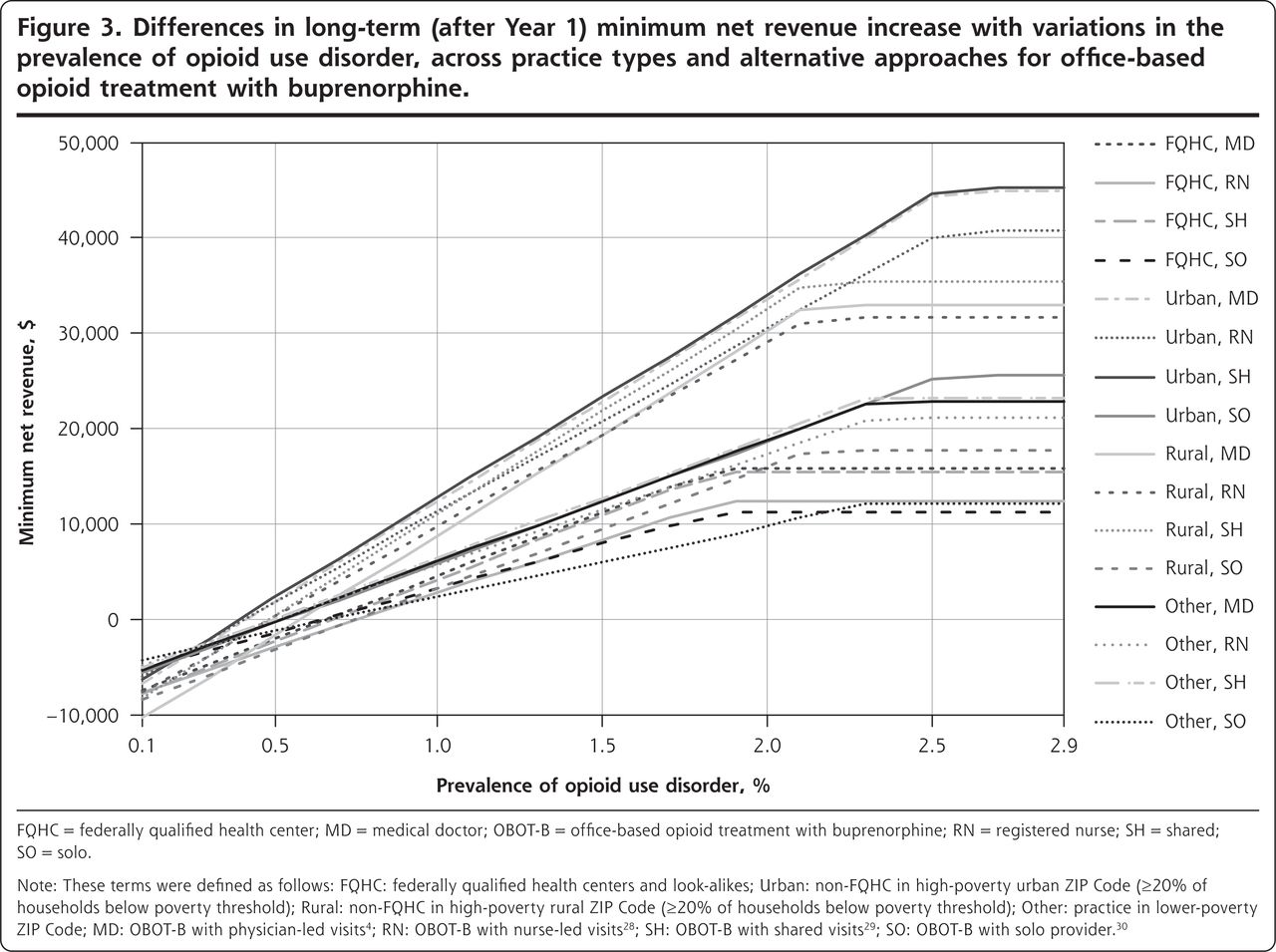
- Figure 3.
Differences in long-term (after Year 1) minimum net revenue increase with variations in the prevalence of opioid use disorder, across practice types and alternative approaches for office-based opioid treatment with buprenorphine.
FQHC = federally qualified health center; MD = medical doctor; OBOT-B = office-based opioid treatment with buprenorphine; RN = registered nurse; SH = shared; SO=solo.
Note: These terms were defined as follows: FQHC: federally qualified health centers and look-alikes; Urban: non-FQHC in high-poverty urban ZIP Code (≥20% of households below poverty threshold); Rural: non-FQHC in high-poverty rural ZIP Code (≥20% of households below poverty threshold); Other: practice in lower-poverty ZIP Code; MD: OBOT-B with physician-led visits4; RN: OBOT-B with nurse-led visits28; SH: OBOT-B with shared visits29; SO: OBOT-B with solo provider30.


Tables
- Table 1.
Input Data and Descriptive Details for Alternative Approaches for Office-Based Opioid Treatment With Buprenorphine
OBOT-B With Physician-Led Visits4 OBOT-B With Nurse-Led Visits34 OBOT-B With Shared Visits35 OBOT-B With Solo Provider36 Visit frequency (per patient per year), based on interviews, No. Initial medical evaluation (99204/G0466a) 1 1 1 1 Follow-up medical evaluation, Level 3 (99213/G0467) 15 1 18 16 Follow-up medical evaluation, Level 4 (99214/G0467) 1 4 0 1 Follow-up nursing visit (99211) 0 13 1 0 Behavioral health intake assessment (90791/G0469; combined with initial medical evaluation) 1 1 1 0 Group psychotherapy (90853), 12 patients per group 19 19 18 0 Urine drug screen (80305/G0477) 19 19 20 18 Staff time, based on interviews Physician hours (SD), per patient per year 4.8 (1.2) 2.0 (0.5) 2.9 (0.7) 5.2 (1.3) Nurse care manager hours (SD), per patient per year 1.1 (0.3) 4.0 (1.0) 4.0 (1.0) Behaviorist hours (SD), per patient per year 2.4 (0.7) 2.5 (0.8) 3.0 (0.8) Year 1 additional physician hours (SD) 16.0 (5.0) 16.0 (5.0) 16.0 (5.0) 32.0 (10.0) Year 1 nurse and behaviorist additional setup hours (SD) 40.0 (10.0) 40.0 (10.0) 40.0 (10.0) Hours (SD) worked per full-time equivalent employee per year37 2,087.0 (96.0) 2,087.0 (96.0) 2,087.0 (96.0) 2,087.0 (96.0) OBOT-B = office-based opioid treatment with buprenorphine.
Note: For insurance rates, we sampled from the probability distribution of Medicare payer prevalence. If a simulated individual was not selected to have Medicare, we sampled from the Medicaid prevalence. If the simulated individual was not selected to have Medicaid, we sampled from the private insurance prevalence. If the individual was not selected to have private insurance, they were assigned as self-pay/uninsured. Payment rates were log-transformed before sampling to adjust for skew and were determined from the Medicare Physician Fee Schedule Look-up Tool, publicly available state Medicaid fee schedules, and the Collective Health database of commercial payment rates.42-44 Appropriate billing codes for OBOT-B were determined in consultation with interviewed primary care practice representatives and informed by guidance from the Centers for Medicare & Medicaid Services, Substance Abuse and Mental Health Services Administration, and National Association of Community Health Centers.36-38
↵a Current Procedural Terminology (CPT) visit codes.
FQHC or FQHC Look-Alike Non-FQHC in High-Poverty Urban ZIP Code (≥20% of Households Below Poverty Threshold) Non-FQHC in High-Poverty Rural ZIP Code (≥20% of Households Below Poverty Threshold) Practice in Lower-Poverty ZIP Code Demand for therapy Prevalence of opioid use disorder, % (SD)38 1.3 (0.2) 1.3 (0.2) 1.6 (0.4) 0.8 (0.3) Screening tool sensitivity, % (SD)39 100.0 (0) 100.0 (0) 100.0 (0) 100.0 (0) Screening tool specificity, % (SD)39 73.5 (1.8) 73.5 (1.8) 73.5 (1.8) 73.5 (1.8) Proportion of patients accepting therapy when offered, based on interviews, % (SD) 80.0 (2.5) 80.0 (2.5) 80.0 (2.5) 80.0 (2.5) No-show rate, % (SD)26 22.0 (5.0) 20.0 (5.0) 25.0 (5.0) 20.0 (5.0) Practice characteristic Panel size, all patients per full-time physician, No. (SD)40 2,040 (551) 1,480 (316) 1,760 (357) 1,620 (337) Payer prevalence, Medicare, % (SD)40 11 (3) 27 (7) 20 (5) 22 (6) Payer prevalence, Medicaid, % (SD)40 57 (14) 20 (5) 18 (5) 13 (3) Payer prevalence, private, % (SD)40 10 (3) 48 (12) 48 (12) 60 (15) Payer prevalence, uninsured/self-pay, % (SD)40 22 (6) 5 (1) 14 (4) 5 (1) Salary and overhead costs26,40,41 Nurse care manager salary per year, $ (SD) 65,683 (8,624) 73,101 (7,418) 57,059 (8,624) 81,724 (8,623) Behaviorist salary per year, $ (SD) 50,713 (9,321) 58,266 (7,553) 41,392 (9,321) 67,957 (9,691) Overhead rate, % (SD) 47 (14) 47 (14) 47 (14) 47 (14) FQHC = federally qualified health center; OBOT-B = office-based opioid treatment with buprenorphine.
Note: For insurance rates, we sampled from the probability distribution of Medicare payer prevalence. If a simulated individual was not selected to have Medicare, we sampled from the Medicaid prevalence. If the simulated individual was not selected to have Medicaid, we sampled from the private insurance prevalence. If the individual was not selected to have private insurance, they were assigned as self-pay/uninsured. Payment rates were log-transformed before sampling to adjust for skew and were determined from the Medicare Physician Fee Schedule Look-up Tool, publicly available state Medicaid fee schedules, and the Collective Health database of commercial payment rates.42-44 Appropriate billing codes for OBOT-B were determined in consultation with interviewed primary care practice representatives and informed by guidance from the Centers for Medicare & Medicaid Services, Substance Abuse and Mental Health Services Administration, and National Association of Community Health Centers.36-38
Visit Type Medicare $ (SD) Medicaid $ (SD) Private $ (SD) Uninsured/Self-Pay $ (SD) Initial medical evaluation (99204/G0466a) 158.80 (22.80) 106.60 (31.40) 222.70 (2.40) 106.60 (31.40) Follow-up medical evaluation, Level 3 (99213/G0467) 68.00 (13.80) 45.50 (12.70) 111.10 (0.90) 45.50 (12.70) Follow-up medical evaluation, Level 4 (99214/G0467) 101.70 (18.20) 68.60 (21.20) 156.70 (1.20) 68.60 (21.20) Follow-up nursing visit (99211) 17.40 (7.60) 10.80 (6.20) 46.80 (1.80) 10.80 (6.20) Behavioral health intake assessment (90791/G0469) 142.60 (11.70) 73.10 (6.00) 126.40 (2.70) 73.10 (6.00) Group psychotherapy (90853), 12 patients per group 28.00 (2.20) 14.40 (1.10) 151.90 (21.30) 14.40 (1.10) Urine drug screen (80305/G0477) 13.50 (2.80) 11.90 (2.50) 55.00 (27.30) 11.90 (2.50) OBOT-B = office-based opioid treatment with buprenorphine.
Note: For insurance rates, we sampled from the probability distribution of Medicare payer prevalence. If a simulated individual was not selected to have Medicare, we sampled from the Medicaid prevalence. If the simulated individual was not selected to have Medicaid, we sampled from the private insurance prevalence. If the individual was not selected to have private insurance, they were assigned as self-pay/uninsured. Payment rates were log-transformed before sampling to adjust for skew and were determined from the Medicare Physician Fee Schedule Look-up Tool, publicly available state Medicaid fee schedules, and the Collective Health database of commercial payment rates.42-44 Appropriate billing codes for OBOT-B were determined in consultation with interviewed primary care practice representatives and informed by guidance from the Centers for Medicare & Medicaid Services, Substance Abuse and Mental Health Services Administration, and National Association of Community Health Centers.36-38
↵a Current Procedural Terminology (CPT) visit codes.
- Table 4.
Primary and Secondary Outcomes in the First Year of Buprenorphine Treatment Implementation (Year 1) and in Each Subsequent Year (After Year 1 for Each of 10 Years) Across 4 Approaches for Office-Based Opioid Treatment With Buprenorphine, and Among the Different Simulated Practice Types
Gross Revenue $ (95% CI) Opportunity Costs $ (95% CI) New Personnel and Overhead Costs $ (95% CI) Net Revenue $ (95% CI) Year 1 FQHC Physician-led 41,769 (17,408-73,092) 6,395 (2,517-12,393) 6,514 (3,508-10,647) 28,859 (9,247-54,294) Nurse-led 35,857 (15,013-63,183) 3,240 (1,438-5,964) 9,746 (4,929-16,344) 22,870 (6,258-45,087) Shared 41,942 (17,390-73,618) 4,081 (1,716-7,573) 9,193 (4,700-15,475) 28,668 (9,026-55,032) Solo 29,656 (12,298-52,300) 7,880 (3,374-14,569) 0 21,776 (7,964-40,045) Urban Physician-led 59,641 (27,589-104,484) 7,508 (3,471-13,481) 6,364 (3,632-9,832) 45,769 (17,812-85,568) Nurse-led 54,576 (24,983-96,817) 3,996 (2,014-6,793) 8,974 (5,062-14,234) 41,606 (15,280-79,472) Shared 59,046 (27,545-103,358) 4,931 (2,429-8,497) 8,521 (4,810-13,509) 45,593 (17,826-85,198) Solo 35,112 (16,659-61,275) 9,552 (4,779-16,355) 0 25,560 (10,299-47,435) Rural Physician-led 85,035 (34,078-157,980) 10,027 (4,086-19,218) 5,642 (2,966-9,378) 69,366 (24,814-134,442) Nurse-led 77,939 (30,947-146,822) 5,041 (2,317-9,133) 8,575 (4,285-14,885) 64,323 (22,021-126,578) Shared 84,142 (34,404-155,899) 6,368 (2,838-11,789) 8,092 (4,091-14,110) 69,682 (24,761-134,089) Solo 49,895 (20,589-92,754) 12,299 (5,549-22,553) 0 37,596 (13,617-73,853) Other Physician-led 45,677 (10,184-97,483) 5,976 (2,115-12,076) 6,302 (3,338-10,049) 33,399 (2,990-79,070) Nurse-led 42,193 (9,386-91,756) 3,399 (1,506-6,194) 8,296 (4,168-14,212) 30,499 (2,065-75,037) Shared 45,116 (10,211-96,573) 4,078 (1,696-7,662) 7,929 (3,949-13,301) 33,108 (2,651-79,258) Solo 26,085 (5,935-55,506) 7,944 (3,303-14,887) 0 18,141 (1,702-42,051) Year 2+ FQHC Physician-led 41,769 (17,408-73,092) 5,519 (1,779-11,327) 3,234 (1,159-6,404) 33,016 (13,567-58,589) Nurse-led 35,857 (15,013-63,183) 2,357 (749-4,925) 6,455 (2,345-12,448) 27,044 (10,820-49,205) Shared 41,942 (17,390-73,618) 3,204 (1,024-6,509) 5,903 (2,108-11,579) 32,835 (13,388-59,298) Solo 29,656 (12,298-52,300) 6,119 (1,979-12,547) 0 23,538 (9,683-41,899) Urban Physician-led 59,641 (27,589-104,484) 6,153 (2,333-12,012) 2,660 (1,145-5,016) 50,828 (22,860-90,418) Nurse-led 54,576 (24,983-96,817) 2,631 (977-5,113) 5,257 (2,237-9,696) 46,688 (20,264-84,319) Shared 59,046 (27,545-103,358) 3,575 (1,358-6,884) 4,806 (2,053-8,917) 50,664 (23,090-90,283) Solo 35,112 (16,659-61,275) 6,829 (2,576-13,015) 0 28,283 (12,938-50,689) Rural Physician-led 85,035 (34,078-157,980) 8,716 (2,901-17,783) 3,671 (1,337-7,339) 72,649 (28,513-137,390) Nurse-led 77,939 (30,947-146,822) 3,721 (1,228-7,608) 5,786 (2,116-11,413) 68,432 (26,186-130,898) Shared 84,142 (34,404-155,899) 5,058 (1,703-10,353) 5,305 (1,945-10,692) 73,779 (29,224-138,600) Solo 49,895 (20,589-92,754) 9,664 (3,263-19,592) 0 40,231 (16,037-76,726) Other Physician-led 45,677 (10,184-97,483) 4,512 (1,107-7,623) 2,080 (427-4,650) 39,085 (8,650-85,210) Nurse-led 42,193 (9,386-91,756) 1,923 (371-4,339) 4,058 (860-9,042) 36,212 (7,785-80,774) Shared 45,116 (10,211-96,573) 2,615 (503-5,939) 3,695 (813-8,171) 38,806 (8,649-84,639) Solo 26,085 (5,935-55,506) 5,000 (983-11,455) 0 21,086 (4,697-45,406) FQHC = federally qualified health center.
Note: The 4 approaches were (1) buprenorphine therapy via prescriber-led visits, which involved prescribers leading routine visits for medication management with a nurse care manager providing program coordination, intake visits, telephone outreach, and induction management, (2) buprenorphine therapy via nurse-led visits, which involved a nurse care manager leading patient visits and care management and prescribers meeting the patient every 3 months after induction for medication management, (3) buprenorphine therapy via shared medical appointments, which involved the prescribers leading a weekly group visit (including medication titration) in concert with a behaviorist and nurse care manager, and (4) buprenorphine therapy via a solo prescriber, which involved the physician prescribing buprenorphine without major structural support from auxiliary staff. The 4 practice types were (1) FQHCs and FQHC look-alikes, (2) non-FQHC practices in high-poverty urban areas by Census definition (>20% of households within the ZIP Code having an income below the federal poverty threshold after adjustment for household size), (3) non-FQHC practices in high-poverty rural areas by Census definition (>20% of households within the ZIP Code having an income below the federal poverty threshold after adjustment for household size), and (4) practices outside of high-poverty areas.
Supplemental Appendix & Table
Supplemental Appendix & Table
Files in this Data Supplement:
- Supplemental data: Appendix & Table - PDF file
In this issue




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.