


Abstract
BACKGROUND We wanted to evaluate the benefits and harms of screening children in primary health care settings for abuse and neglect resulting from family violence by examining the evidence on the performance of screening instruments and the effectiveness of interventions.
METHODS We searched for relevant studies in MEDLINE, PsycINFO, CINAHL, ERIC, Cochrane Controlled Trials Register, and reference lists. English language abstracts with original data about family violence against children focusing on screening and interventions initiated or based in health care settings were included. We extracted selected information about study design, patient populations and settings, methods of assessment or intervention, and outcome measures, and applied a set of criteria to evaluate study quality.
RESULTS All instruments designed to screen for child abuse and neglect were directed to parents, particularly pregnant women. These instruments had fairly high sensitivity but low specificity when administered in high-risk study populations and have not been widely tested in other populations. Randomized controlled trials of frequent nurse home visitation programs beginning during pregnancy that address behavioral and psychological factors indicated improved abuse measures and outcomes. No studies were identified about interventions in older children or harms associated with screening and intervention.
CONCLUSIONS No trials of the effectiveness of screening in a health care setting have been published. Clinician referrals to nurse home visitation during pregnancy and in early childhood may reduce abuse in selected populations. There are no studies about harms of screening and interventions.
- Domestic violence/prevention and control
- child abuse
- child neglect
- review, academic
- evidence-based medicine
INTRODUCTION
Child abuse and neglect has been defined as “any recent act or failure to act on the part of a parent or caretaker which results in death, serious physical or emotional harm, sexual abuse or exploitation, or an act or failure to act which presents an imminent risk of serious harm.”1 Approximately 1 million children are identified as abused in the United States each year.2 In 1999, reported abuse rates were 1,180 per 100,000 children with the highest rates for children age 3 years and younger.3 An estimated 1,100 children died of abuse and neglect that year, approximately 1.62 deaths per 100,000 children.3 Reported abuse likely captures only a fraction of all cases.4 A large survey of adults indicated that 11% experienced psychological abuse, 11% physical abuse, and 22% sexual abuse during childhood.5
Frequently cited factors associated with child abuse and neglect include low income,6–,9 low maternal education,6–,8 nonwhite ethnicity,6,9 large family size,6,8 young age of the mother,6 single-parent status,6 parental psychiatric disturbance,10 and presence of a stepfather,6 among others.6,11 As the number of risk factors increases, the proportion of children maltreated also increases.6
Many health problems are associated with abuse and neglect. These problems include acute trauma, including death, unwanted pregnancy, and long-term physical and mental problems, such as depression, post-traumatic stress disorder, somatization, suicide, and substance abuse.5,12–,21 Children who witness intimate partner violence are at risk for developmental delay, school failure, and a variety of psychiatric disorders including depression and oppositional defiant disorder,22,23 and violence against others.24 Children experiencing sexual or physical abuse have a higher risk of intimate partner abuse as adults.25–,28
The clinician’s role in identification and intervention is considered a professional responsibility by physician and nursing organizations.29,30 Ongoing child abuse is evidenced as multiple and recurrent injuries, injury histories inconsistent with physical findings, and injuries inconsistent with children’s abilities to sustain them on their own. Identification and reporting of abuse are inconsistent and highly dependent on the clinician’s awareness and training. Reporting child abuse to protective services is mandatory in almost all states, although statutes mandating reporting vary. Nineteen states require that any person who suspects child abuse or neglect must report; the majority of states limit mandatory reporting to professionals working with children.31 Hospitals are also required to address abuse for accreditation.32
Many children experiencing abuse do not show obvious evidence of abuse. Whether screening all children leads to a decline in abuse is unknown, protocols for screening are lacking, and few clinicians routinely screen patients who do not have apparent injuries.33–,38 The evidence for how to intervene effectively once problems are identified is limited.
In 1996, the US Preventive Services Task Force (USPSTF) concluded that there was insufficient evidence to recommend for or against the use of specific screening instruments to detect family violence for children, but it recommended that clinicians ask questions about abuse if it is suspected.39 This report is an update on the current literature on family violence focusing on studies of the performance of screening instruments designed for the health care setting and the effectiveness of clinical-based interventions for children. A separate report on screening for family violence in women and elderly adults is available elsewhere.40
METHODS
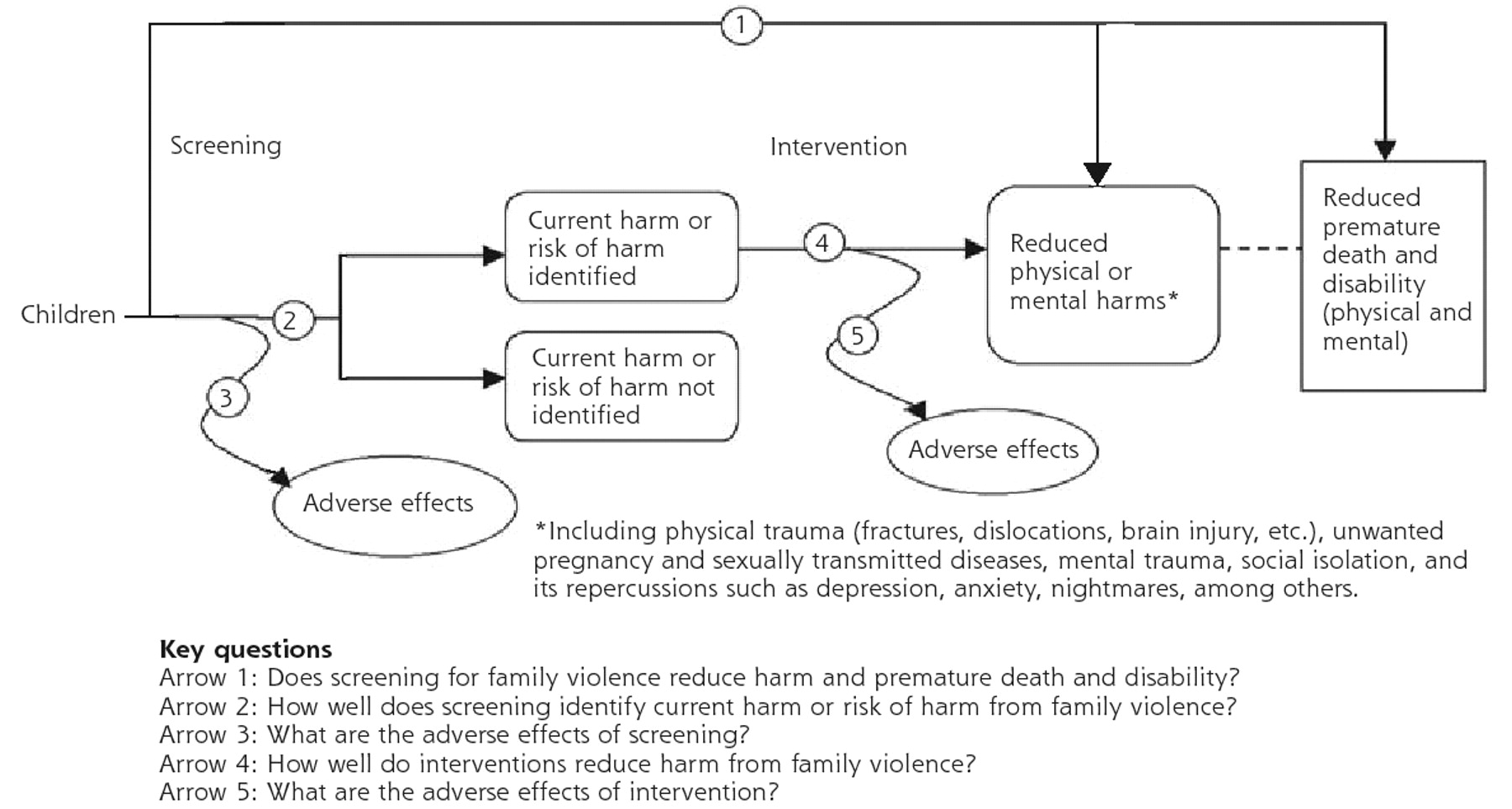
The analytic framework and key questions guiding this systematic review are detailed in Figure 1⇓. Relevant studies were identified from multiple searches of MEDLINE (1966 to December 2002), PsycINFO (1984 to December 2002), CINAHL (1982 to December 2002), ERIC (1989 to December 2002), and the Cochrane Controlled Trials Register (search strategies are available as supplemental data in Appendix 1, which can be found online at http://www.annfammed.org/cgi/content/full/2/2/161/DC1). We reviewed references listed in a review of early childhood home visitation for the prevention of violence for the US Task Force on Community Prevention Service,41 the Prevention of Child Maltreatment Update from the Canadian Task Force on Preventive Health Care,42 and Violence in Families: Assessing Prevention and Treatment Programs.43 Additional articles were obtained by reviewing reference lists of pertinent studies, reviews, and editorials, and by consulting experts.
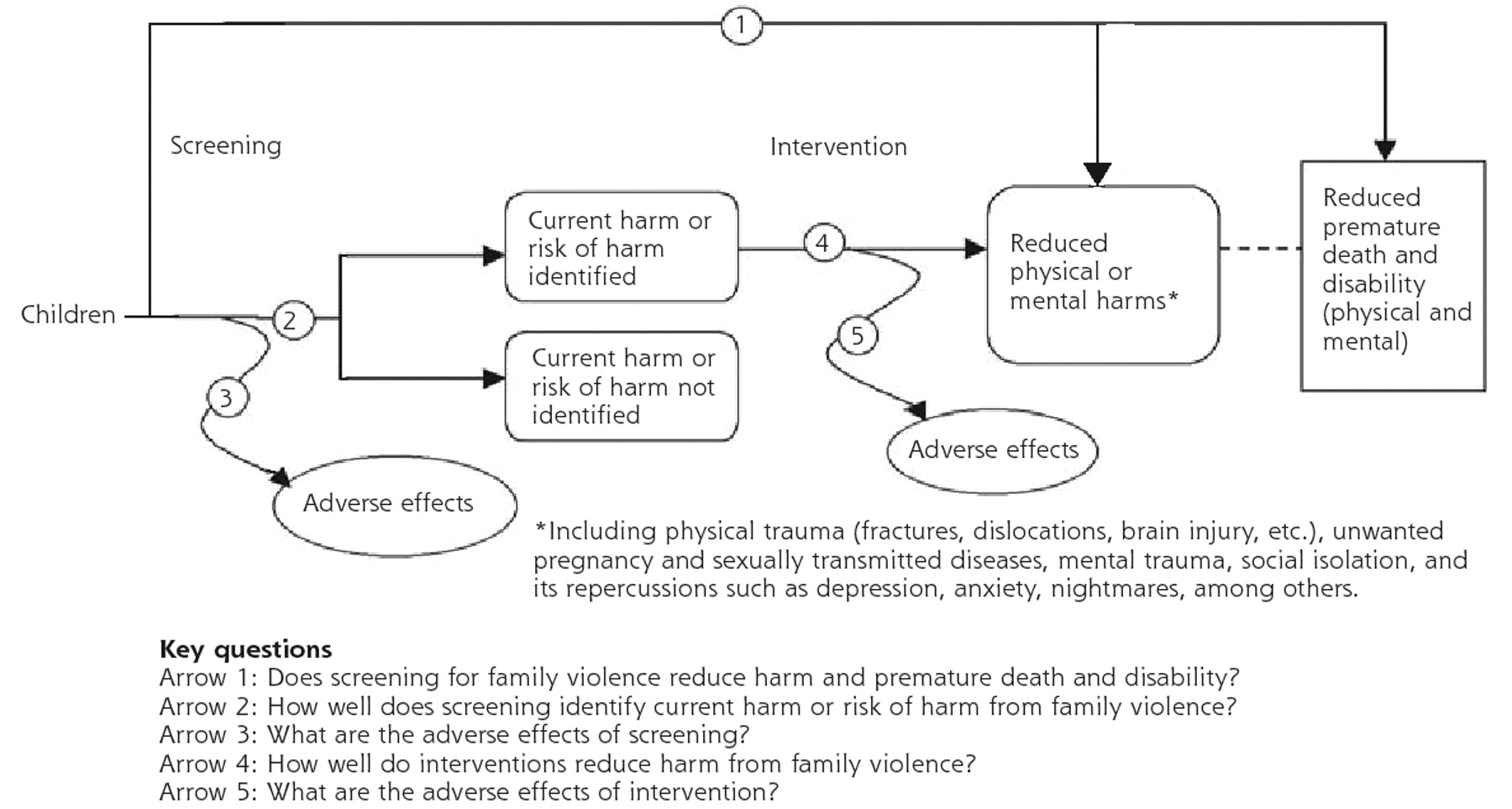
Analytic framework and key questions.
We defined screening as assessment of current harm or risk of harm from family violence in asymptomatic persons in a health care setting. Universal screening means assessing everyone; selective screening indicates only those who meet specific criteria are assessed. The target population for this review was children as victims of abuse or neglect directed toward them by family members, caretakers, or others with similar relationships.
Studies included in this review had English-language abstracts, were applicable to US clinical practice, described abuse and neglect against children, were conducted in or linked to primary care (family practice, pediatrics), obstetrics and gynecology, or emergency department settings, and included a physician or other health provider in the process of assessment or intervention. We excluded studies about patients with trauma.
Studies about assessment were included if they evaluated the performance of verbal or written questionnaires or other assessment procedures, such as physical examinations, that were brief and applicable to the primary care setting. Included studies described the study sample, the screening instrument or procedure, the abuse or neglect outcome, and the collection of data. Outcomes included indicators of physical abuse, neglect, emotional abuse or sexual abuse, and any reported related health outcomes (ie, depression).
Studies about interventions were included if they measured the effectiveness of an intervention in reducing harm from family violence compared wth comparison groups. We excluded studies that tested effectiveness of interventions to educate health care professionals about family violence or to increase screening rates in institutions. We also excluded studies about mandatory reporting laws, descriptions of programs, the accuracy of physician diagnosis and reporting of abuse, and physician factors related to reporting.
From each included study, we abstracted the study design, number of participants, setting, length and type of interventions, length of follow-up, outcomes, methods of outcome measurement, and study duration, among others. Two reviewers independently rated the quality of each study using criteria specific to different study designs developed by the USPSTF (study quality rating criteria are available as supplemental data in Appendix 2, which can be found online at http://www.annfammed.org/cgi/content/full/2/2/161/DC2). When reviewers disagreed, a final score was reached through consensus.
RESULTS
Screening
We identified and reviewed 1,808 abstracts and retrieved 65 articles for further review. Six studies met eligibility criteria. Additional details of these studies are provided in Table 1⇓,44–,50 and as supplemental data in Appendix 3,44–,68 which can be found online at http://www.annfammed.org/cgi/content/full/2/2/161/DC3.
Studies of Child Abuse Screening Instruments
No studies meeting eligibility criteria directly addressed the effectiveness of screening in reducing harm and premature death and disability. A limited number of studies described the performance of screening methods, such as self-administered questionnaires, clinical staff-directed interviews, and clinical observation. All studies primarily assessed parents, rather than children directly, and none utilized specific physical examination protocols for screening. Instruments and scoring procedures included in these studies are described in Appendix 4,49,51–,53 which can be found online as supplemental data at http://www.annfammed.org/cgi/content/full/2/2/161/DC4.
Few studies evaluated the performance of these approaches in predicting child abuse and neglect outcomes. Screening instruments had fairly high sensitivity but low specificity when administered in the study populations. Best results were achieved when screening involved a 2-step method; however, these strategies have not been widely tested in other populations and have not been evaluated for feasibility in the primary care setting.
Self-administered Questionnaires
The Kempe Family Stress Inventory (KFI)53 was used in 3 studies meeting eligibility criteria (Table 1⇑).44–47,52 Study populations included predominantly young, single women with low socioeconomic indicators. A retrospective cohort study found that a high score on the KFI was the only statistically significant predictor of maltreatment at 1 and 2 years and, when compared with a low score, was associated with more clinic visits during the first year and hospital admissions during the first 6 months.44 Other studies used the KFI in a 2-step screening process that began with the 15-item Hawaii Risk Indicators Screening Tool.45–47,52 The 2-step process had 89% sensitivity and 28% specificity when compared with responses on the Child Abuse Potential (CAP) inventory, a 160-item instrument,45,46,52 and 97% sensitivity and 21% specificity when compared with maltreatment rates in another study.47,52
Clinical Staff-administered Questionnaires
The Maternal History Interview (MHI-2) utilizes open-ended questions and subscales to evaluate parenting skills, personality, discipline philosophy, life stress, and others to determine risk for child abuse.48 Mothers determined to be high-risk by the MHI-2 had a higher incidence of reported child abuse than low-risk mothers in a study of young pregnant women.48 The Parenting Profile Assessment (PPA) is a 21-item nurse interview designed for the primary care setting.49 Responses on the PPA were compared with self-reports about past episodes and indicated 75% sensitivity and 86% specificity.49
Other Techniques: Clinician Observation
In a retrospective cohort study, nurses referred patients and their newborns to the hospital’s child abuse committee from the postpartum unit after determining them to be at high risk for abuse based on a number of nonstandardized criteria.50 When compared with low-risk patients, high-risk patients had a significantly greater rate of subsequent hospitalizations for medical and psychosocial reasons.
Interventions
We found and reviewed 1,748 abstracts. Seventeen studies, utilizing 13 unique populations, met inclusion criteria,47,48,54–,68 including 9 randomized controlled trials. All studies evaluated interventions for pregnant and postpartum women and their infants and are described in Table 2⇓47,48,54–,68 and Appendix 344–,68 (http://www.annfammed.org/cgi/content/full/2/2/161/DC3).
Summary of Intervention Studies
A randomized controlled trial with a 15-year follow-up indicated that nurse home visits during the prenatal period and for 2-years postpartum for low-income women can improve short-term and long-term abuse and neglect outcomes for children.54–,58 Nurse visits included parent education, support systems for the mother, and engagement of family members with other health and social services. Results at 2 years showed that high-risk women who had nurse visits were less likely to commit acts of child abuse and neglect than high-risk women without visits (P = .07).57 At 3- and 4-year follow-up observations, there were no differences between groups for child abuse and neglect outcomes.54,55 At the 15-year follow-up, children in the nurse-visited group were less likely to have reports of child maltreatment of any kind (P <.05).58 Mothers in the nurse-visited group were less likely to be perpetrators of child abuse and neglect than mothers without nurse visits 15 years after the intervention (P <.001).56
Six trials of fair quality evaluated home visitation programs linked to prenatal clinics or hospital care.59–,64 Studies varied in the types and duration of interventions. All but 1 study62 used inclusion criteria based on an assessment of risk for child abuse and neglect, although no study used standardized or validated instruments. Studies generally considered positive responses to criteria, such as social or demographic risk factors (unmarried, low level of education, unemployed),59,63 drug use during pregnancy,61 low birth weight,64 or a history of other risk factors (human immunodeficiency virus infection, homelessness, substance use),60 among others. Follow-up ranged from 2 to 24 months after delivery, and abuse outcomes were determined by a number of methods.
None of these studies described significantly fewer reports of abuse and neglect in intervention groups compared with control groups, although not all studies were designed for this outcome.63 Five of the studies reported other significant intervention effects related to abuse and neglect, such as medical care utilization, parent-child interactions, punishment, stressful life events, parental mental illness, and drug use.59–61,63,64
Harms of Screening and Interventions
No studies were identified that provide data about adverse effects of screening or interventions. False-negative tests may hinder identification of those who are truly at risk. False-positive tests could lead to inappropriate labeling and punitive attitudes. Additional possible harms include psychological distress, escalation of abuse and family tension, loss of personal residence and financial resources, erosion of family structure, loss of autonomy for the victim, and lost time from work. Children could lose contact with established support systems including neighbors, siblings, school contacts, and peer groups.
There has been concern that patients may feel uncomfortable or threatened if asked questions about family violence. Although most women bringing their children to a pediatric emergency department believed screening for family violence was appropriate, many indicated that their willingness to disclose might be affected by fear of being reported to child protective services.69 Clinicians in the study indicated that they would feel obligated to report a child to protective services if violence were present in the home.
DISCUSSION
Detection of child abuse and neglect by clinicians could potentially reduce serious harms to children. Screening for abuse or risk of abuse, however, poses unique challenges. Determining performance characteristics of screening instruments, such as sensitivity and specificity, is difficult because there is no reference standard for detecting actual episodes of abuse. Screening instruments require high sensitivity and specificity, because falsely implicating a parent as an abuser may have serious consequences. For children, mandatory reporting requires that documentation of abuse exists, but reported abuse likely captures only a fraction of all cases. In a recent survey of nurses and physicians, 71% of respondents rated the identification of maltreatment as rather difficult or difficult.70 Work pressure, unfamiliarity, and awkwardness were cited as barriers.
Existing instruments to detect child abuse are not designed for direct administration to the child, missing opportunities to screen older children in the context of usual health care. Screening for abuse in the primary care setting can involve a variety of techniques, including physical examination as well as questionnaires. History from the child has been stated as the most important diagnostic feature in determining child sexual abuse.71 Findings during a routine physical examination suggestive of abuse and neglect, such as burns, bruises, and repeated suspect traumatic injury, have been described.39,72 Many professional medical organizations, including the American Academy of Pediatrics, the American Medical Association, and the American Academy of Family Physicians, recommend that physicians remain alert for the signs and symptoms of child abuse and neglect in the medical visit.
Even if current screening methods correctly identified children at risk of abuse, optimal interventions are not clearly established or widely available. Studies of interventions for prevention of child abuse focused on the prenatal, postpartum, and early childhood periods.73 Both the US Task Force on Community Preventive Services41 and the Canadian Task Force on Preventive Health Care42 recommend this service. Interventions for older children have not yet been shown to be effective.
There are many gaps in the evidence for screening children for abuse, and future research should address these needs. Definitions and measures of abuse, neglect, severity, and chronicity need to be standardized across studies. Existing screening instruments require more testing and validation in various health care settings, as well as modification of those that are too long or complex for medical practice. Instruments require validation in languages other than English.
Studies need to consider the influence of observer or surveillance bias.26,41,55 In studies of child abuse, families in the intervention group are often observed more closely than those in the control group and may be more likely to have abuse detected.65,66 Results could be misrepresented. Interventions are dissimilar between studies and often inadequately described. Programs that deviate from tested models may have different results.
Screening and intervention studies are generally confined to certain high-risk populations while overlooking others, such as special cultural groups and military families. Broader applications would show whether results are generalizable. More research is required to better understand pregnancy-related violence, such as the course of violence during pregnancy and postpartum, health implications, the role of violence on reproductive decision making, and determination of what screening and intervention strategies are most effective for this population.73
Evaluations of the feasibility of screening procedures and interventions in health care settings must consider costs, time, resources, clinician consistency, barriers, and patient compliance. Evaluations of strategies enlisting health systems and community programs are needed. Studies of the effectiveness of treatment programs for abused victims, as well as for perpetrators, would provide needed evidence that identification and intervention can lead to improved health outcomes. These outcomes should include not only measures of reduced violence, but also associated health outcomes, such as improved quality of life, mental health,74 social support, self-esteem, productivity, and others.
Despite the prevalence of child abuse and neglect and its impact on health, there are few studies providing data on its detection and management to guide clinicians. As a result, clinicians have difficulty fulfilling their role in prevention and treatment of the harms of family violence.
Acknowledgments
Agency staff and USPSTF members participated in the initial design of the study and reviewed interim analyses and the final manuscript. Additional reports were distributed for review to content experts and revised accordingly before preparation of this manuscript. The authors thank members of the USPSTF and reviewers of the evidence report for their contributions to this project. We are grateful to Kim Villemyer and Miranda Norbraten for their assistance with preparation of this manuscript.
Footnotes
-
Conflicts of interest: none reported
-
Requests for single reprints: Reprints are available from the Agency for Healthcare Research and Quality Web site (http://www.preventiveservices.ahrq.gov) and through the Agency for Healthcare Research and Quality Publications Clearinghouse (telephone, 800-358-9295).
-
Funding support: This study was conducted by the Oregon Evidence-based Practice Center under contract to the Agency for Healthcare Research and Quality Contract #290-97-0018, Task Order Number 2, Rockville, Md, to support the work of the USPSTF.
-
Disclaimer: The authors of this article are responsible for its contents, including clinical or treatment recommendations. No statement in this article should be construed as an official position of the Agency for Healthcare Research and Quality or the US Department of Health and Human Services.
- Received for publication June 27, 2003.
- Revision received November 12, 2003.
- Accepted for publication November 30, 2003.
- © 2004 Annals of Family Medicine, Inc.





{kind=link}