
Article Figures & Data
Figures
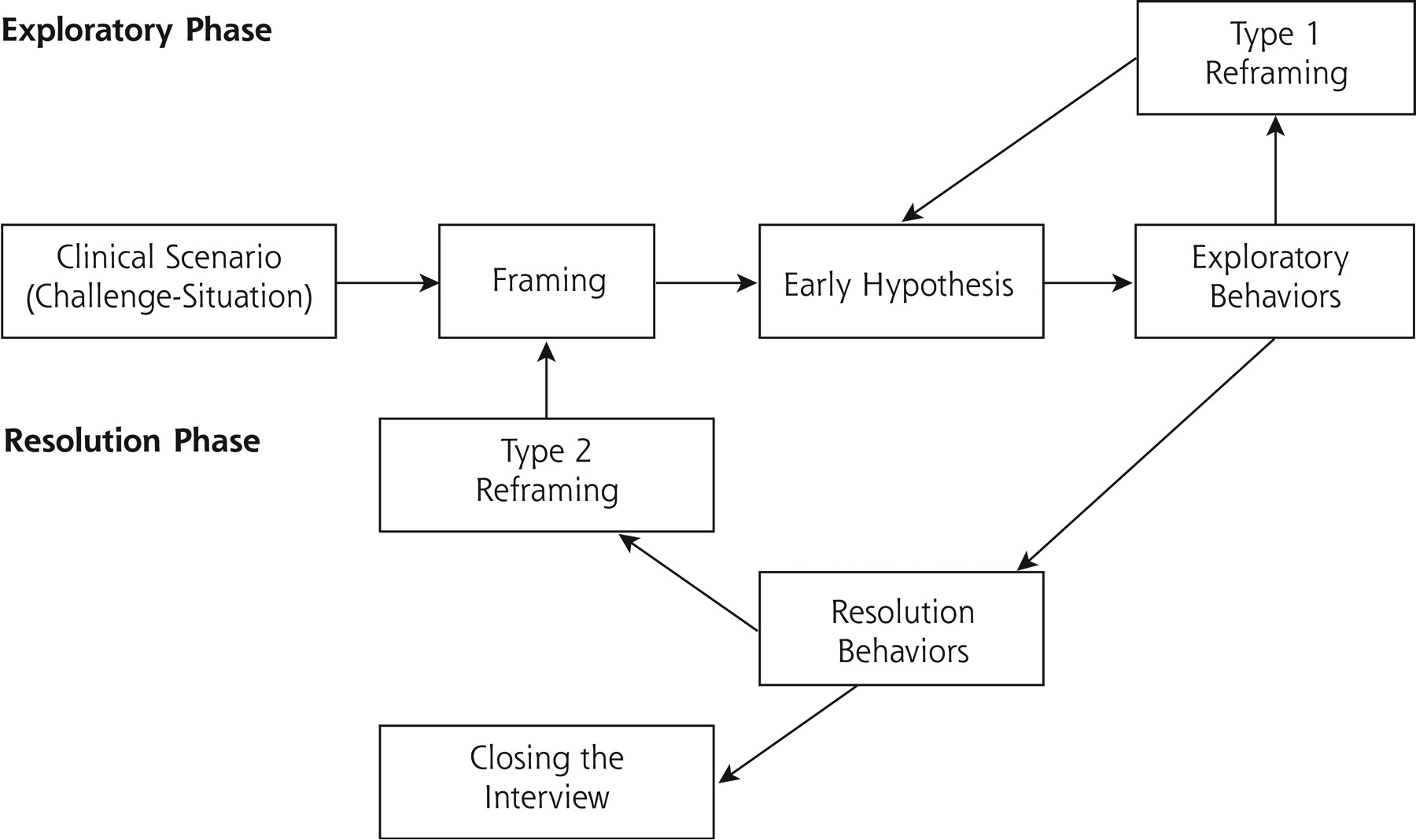
- Figure 1.
Rational-emotive model.
Framing consists of responding to the question: “What is it that I am supposed to do in this particular scenario?” After framing, there automatically appears an early hypothesis that the physician tries to verify. When findings do not fit the hypothesis, other hypotheses might be considered (type 1 reframing), sometimes even global reframing (type 2 refram-ing), such as, for example, “I am not dealing with a shoulder pain, I should consider domestic violence.”
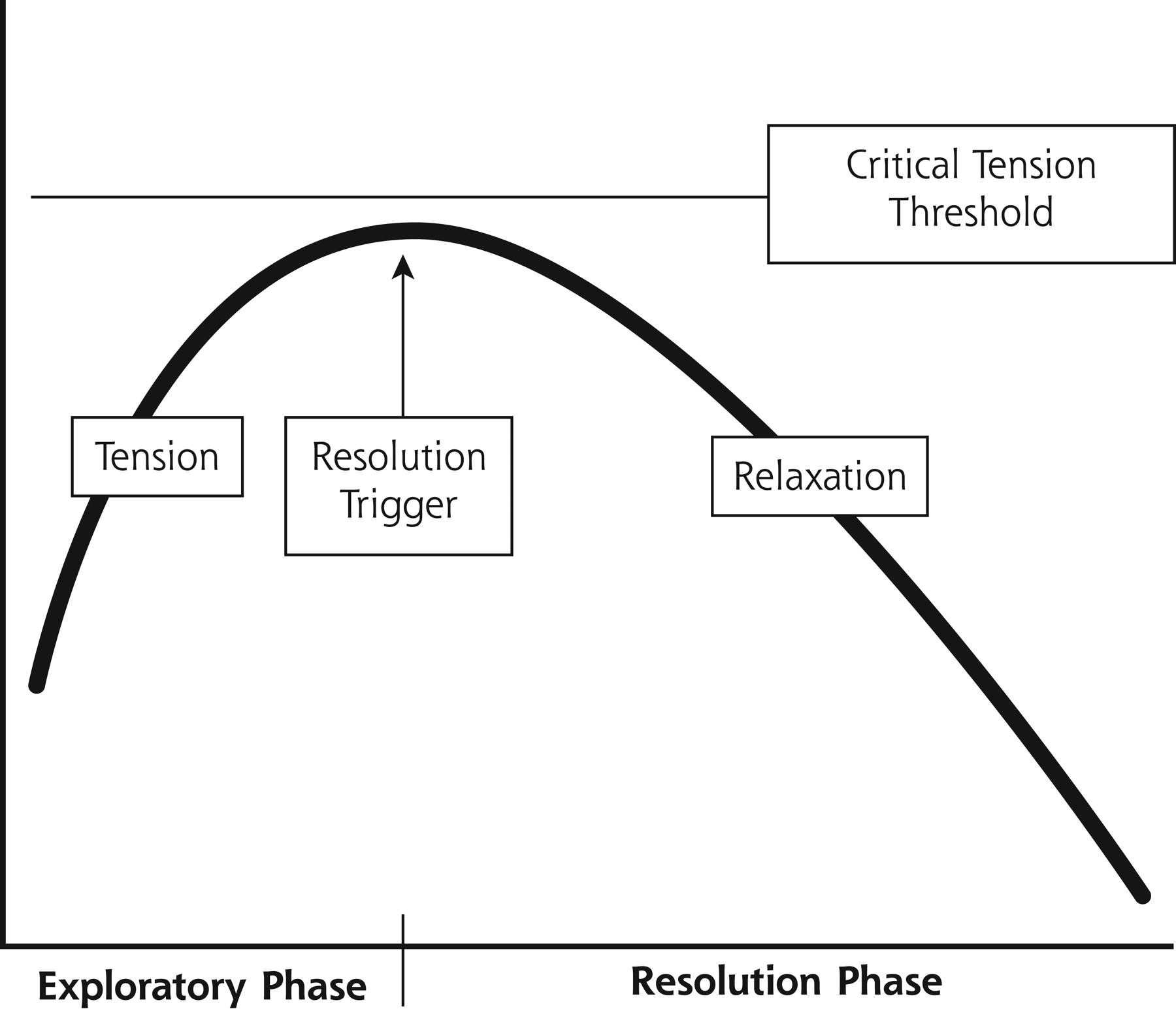
- Figure 2.
Clinical tension.
Trigger resolution consists of saying to oneself: “Stop asking or exploring the patient, I know the diagnosis or what to do.” Sometimes the physician needs more time to achieve a diagnosis, but the tension of not knowing what to do is so important that the physician achieves critical tension, and the resolution trigger is activated. At this point the physician can accept as a good diagnosis an early hypothesis that does not fit well with the case.
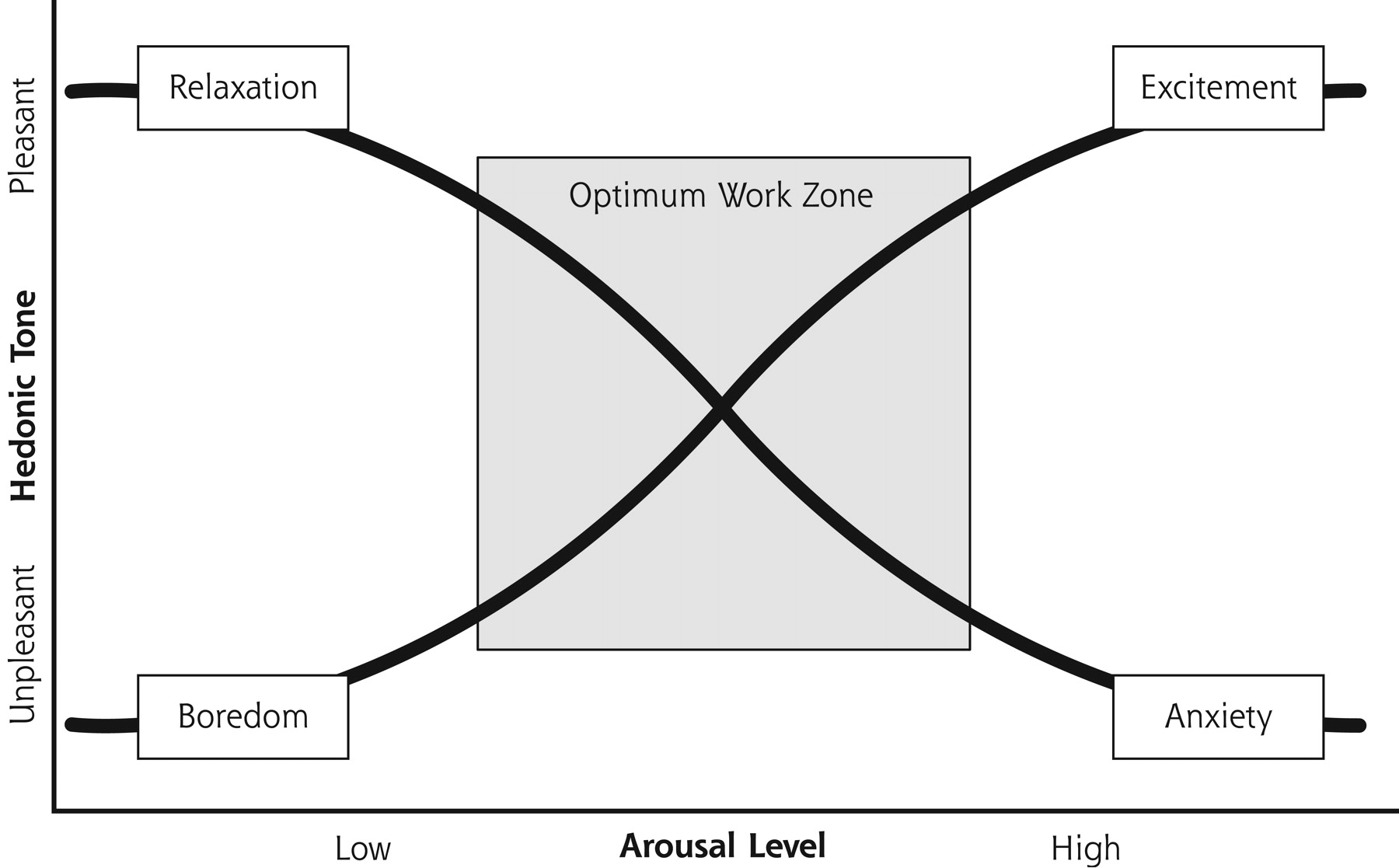
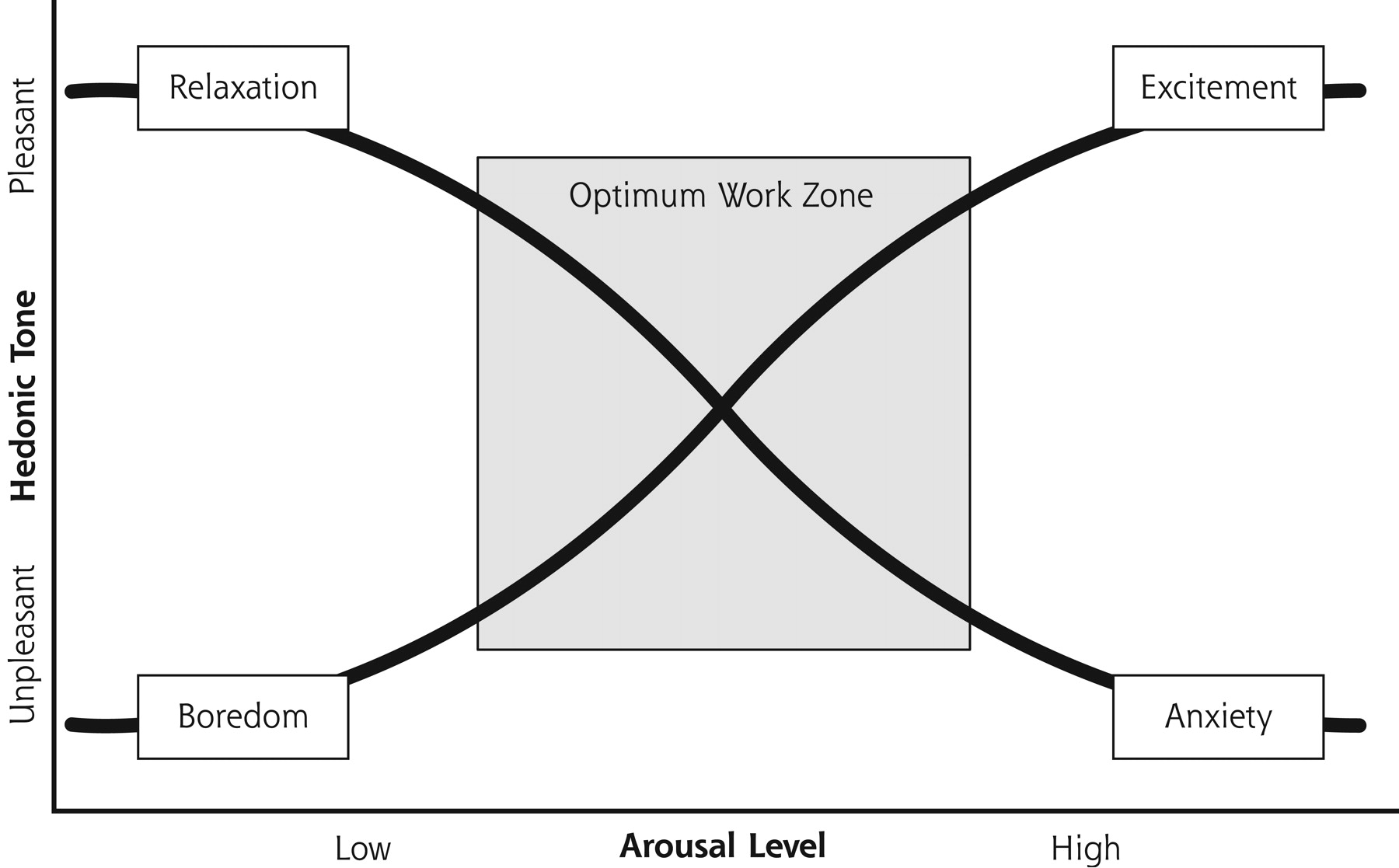
- Figure 3.
Apter’s model of emotional reversal theory.
The optimum work zone avoids extreme values in arousal and hedonic (pleasure) tone. Extreme positions make cognitive processes difficult.
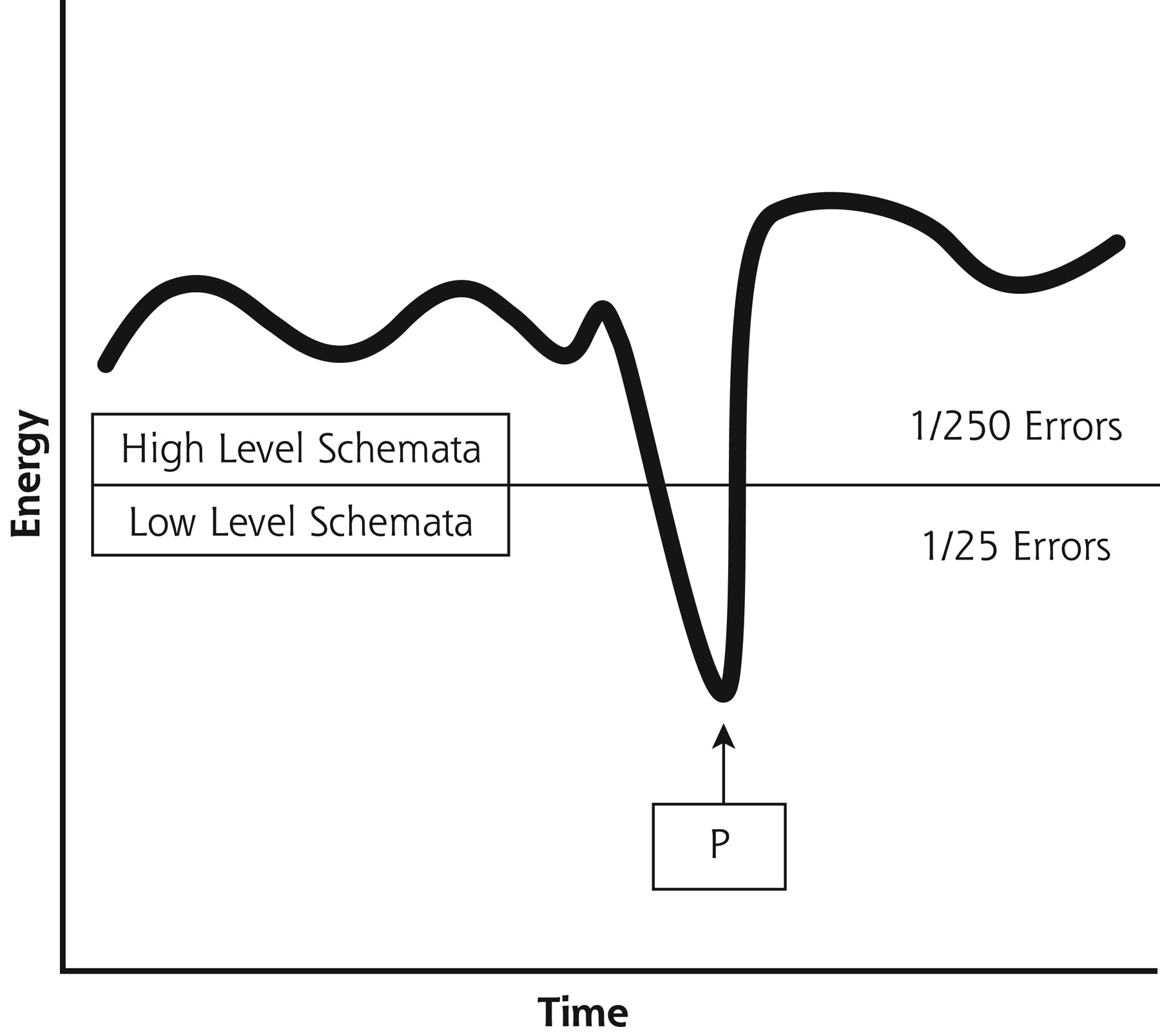
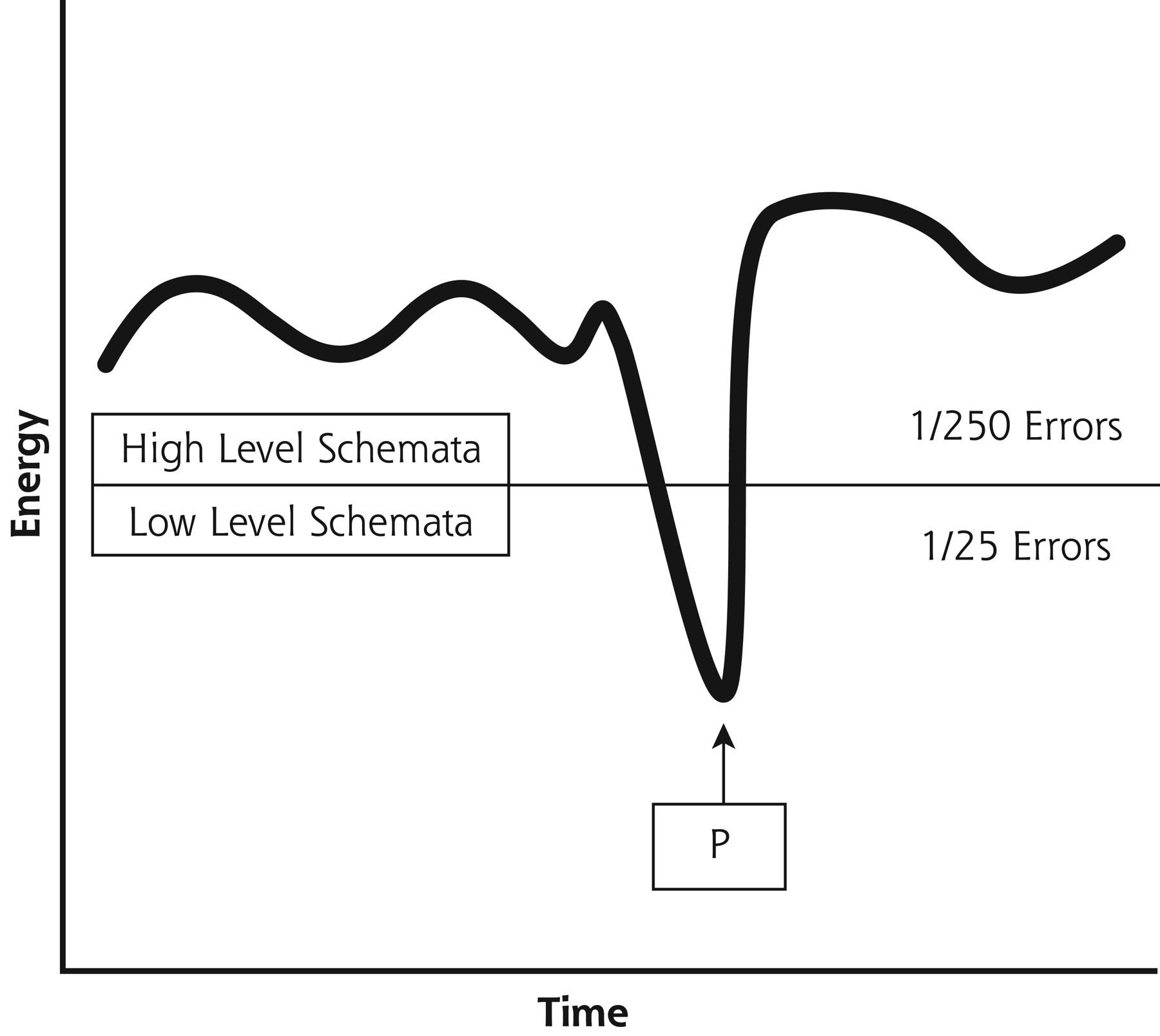
- Figure 4.
Low- or high-level schemata in use.
Observe that in a point of time (P) the physician applies lower level schemata, increasing the rate of errors. When this happens, the physician needs a cognitive alibi, such as “I am very tired,” “this patient is exaggerating,” etc.


Tables
Excessive or Lack of Emotional Arousal Excessive or Lack of Hedonic Tone Fatigue Patient hostility (especially when indirectly expressed) Poor clinical skills The professional’s feelings of rejection or hostility toward the patient (especially when unrecognized) Transient cognitive problems, (for example, sleep disturbances, alcohol consumption, etc) The clinician has a somatic discomfort Lack of motivation Creating more work if a certain hypothesis is confirmed Urgency to finish Overwhelming clinical workload, “excessive workload” Low-Level Decision Rules High-Level Decision Rules Learned in basic stages of apprenticeship Learned from experience Errors experienced not incorporated Errors experienced incorporated Tacit knowledge not reconsidered Tacit knowledge conscientiously revisited Low-Level Schemata High-Level Schemata I’ve got it! As soon as the patient told me, I knew what he had. I should look beyond early hypotheses. If the patient is satisfied with the diagnosis of another physician, why should I bother to find out more data? I should always form my own criteria. When in doubt, choose the simplest or most convenient hypothesis. When in doubt, assume the worst hypothesis. Complains a lot? He doesn’t have anything! I must take a fresh look - perhaps by recording what the patient expresses and later reading it back, paying attention to the diagnosis that spontaneously comes to mind. How might my previous experience affect my actions with this patient? What am I assuming about this patient that might not be true? What surprised me about this patient? How did I respond? What interfered with my ability to observe, be attentive, or be respectful with this patient? How could I be more present with and available to this patient? Were there any points at which I wanted to end the visit prematurely? If there were relevant data that I ignored, what might they be? What would a trusted peer say about the way I managed this situation? Were there any points at which I felt judgmental about the patient-- in a positive or negative way?
The Article in Brief
Teaching doctors to develop their insight and self-awareness could help reduce medical errors. Specific skills to reduce errors include learning to rethink medical situations (that is, being open to a new understanding of the patient's condition(s) and what the doctor should do in response) and learning techniques so that difficult or tense medical visits are not ended too soon.




{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Understanding the Context of Health for Persons With Multiple Chronic Conditions: Moving From What Is the Matter to What Matters
- The pitfalls of premature closure: clinical decision-making in a case of aortic dissection
- L'incertitude clinique: Aider nos etudiants
- Clinical uncertainty: Helping our learners
- Developing Physician Communication Skills For Patient-Centered Care
- Mindfulness and Professionalism in Dentistry
- Stopping the error cascade: a report on ameliorators from the ASIPS collaborative
- Exploring and Validating Patient Concerns: Relation to Prescribing for Depression
- Physicians' Responses to Patients' Medically Unexplained Symptoms
- Quality and Quality Improvement in Forensic Mental Health Evaluations
- The Biopsychosocial Model 25 Years Later: Principles, Practice, and Scientific Inquiry
- How to Use the Annals Online Discussion
- Questions, Interpretation, Exhortation
- In This Issue: Practice Change and Patient Safety