
Abstract
PURPOSE The number of problems managed concurrently by family physicians during patient encounters has not been fully explored despite the implications for quality assessment, guideline implementation, education, research, administration, and funding. Our study objective was to determine the number of problems physicians report managing at each visit and compare that with the number reflected in the chart and the bill.
METHODS Twenty-nine members of the Wisconsin Research Network reported on encounters with 572 patients using a physician problem log. The patient chart notes and the diagnoses submitted for billing from the encounters were compared with the information in these logs.
RESULTS The physicians reported managing an average of 3.05 problems per encounter and recorded 2.82 in the chart and 1.97 on the bill. For all patients, 37% of encounters addressed more than 3 problems, and 18% addressed more than 4. For patients older than 65 years, there was an average of 3.88 problems at each visit, and for diabetic patients there was an average of 4.60. There was evidence for the selective omission of mental health and substance problems from the diagnoses used for billing.
CONCLUSIONS Family medicine involves the concurrent care of multiple problems, which billing data do not adequately reflect. Our findings suggest a mismatch between family medicine and current approaches to quality assessment, guideline implementation, education, research, administration, and funding. Activities in all these areas need to address the physician’s task of prioritizing and integrating care for multiple problems concurrently.
- Family medicine
- family practice
- comprehensive health care
- documentation
- professional practice
- physician’s practice patterns
- delivery of health care
INTRODUCTION
To measure quality realistically, develop and implement guidelines, educate physicians, design research, and administer and pay for services, it is important to understand the number of problems addressed concurrently during primary care encounters. It is also important to assess whether the commonly used data sources, such as chart review and billing data, adequately reflect this aspect of the complexity of care.
Based on previous work, including that of Flocke et al1 and Zyzanski et al,2 we hypothesized that family physicians manage multiple problems during routine outpatient visits. We further hypothesized that there are considerable differences from what actually occurs during primary care encounters (as measured by physician report), what is recorded in the chart, and what is listed on the bill.
We therefore set out to describe the numbers of problems family physicians report managing during outpatient encounters and compare this number with the number generated from the more standard assessment of the content of the visit; that is, reviewing charts and billing data. This method is somewhat different from that used in direct observation studies,3 as our study attempted to “get inside the physician’s head” to ascertain the problem content of the visit, regardless of whether it was observed or recorded. For example, a physician might see a depressed patient for an acute sprain and assess through the interaction that the patient was doing well on his therapy and make a decision not to explore the problem further or change therapy. Such a patient management action would be captured by physician log but not by direct observation.
METHODS
We recruited 29 family physician members of the Wisconsin Research Network (WReN) to record the number of discrete problems managed during patient care encounters. Physicians were in both community and academic practices: 9 were in teaching practices and 20 were in community practices of which 12 were rural. The study was reviewed and approved by the University of Wisconsin Human Subjects Committee. Informed consent for patient and physician participation was obtained. Patients were older than 18 years and competent to give informed consent or were accompanied by an adult competent to give consent.
Each physician filled out a problem log for each patient after each encounter with 20 consecutive patients. This log, a copy of the progress note, and a copy of the bill from each of the recorded encounters were mailed to the WReN office.
The progress notes were analyzed by an experienced medical record coder for the number of discrete problems addressed at a level that would justify at least a level one charge. For purposes of training and standardization, we supplied physicians with detailed instructions, 4 case scenarios, and sample problem logs to fill out. The authors reviewed the responses, and participants were given feedback upon their responses.
For the problem log, a problem was defined as any issue about which the clinician gathered information and made a decision during the encounter. The decision made could be implied (eg, the cough did not require investigation or treatment if it was noted but nothing was done.) To address the issue of when a problem is just part of another problem (eg, neuropathy as part of diabetes), the standard was that if additional data were obtained and a separate decision was made, then the problem should be listed separately. Known problems (eg, diabetes) were not to be listed unless actually addressed at that visit (eg, at an urgent care visit for a sprain). If separate problems merged into 1 at the end of a visit (eg, fever and chest pain merging to pneumonia), then only 1 problem was to be listed.
This broad definition of a problem thus included, eg, fever, hypertension, well-child care, joint pain, or excessive drinking. The definition also included problems in persons other than the patient during the encounter—the so-called secondary patient.4 Thus the issue of a husband’s depression discussed during a woman’s annual examination would be listed as a problem.
For the chart audit, for a problem to be counted, it had to have at least sufficient documentation to justify a level 1 charge. A problem did not have to be listed separately in the progress note for it to be counted; rather, it could have appeared just in the history (eg, “angina is unchanged”) with the implication that the decision was not to change therapy if level 1 criteria were otherwise met.
For the audit of the bill, a problem was defined as any problem listed on the bill for that encounter.
To check for the Hawthorne effect (the change in behavior that results from being observed), we reviewed the progress note from the patient’s previous visit (prior to the study visit), counted the number of problems, and compared this number with the number in the progress note created at the study visit where the physician was recording the number of problems in the log.
Analysis
Data were entered into an Access database and analyzed using SAS statistical software. The number of problems recorded in the physician logs, chart audits, and billing data were compared pairwise for statistical significance using the paired t test. Separate t tests of significance were performed for the subgroup of patients who were aged 65 years or older and for the subgroup of patients with diabetes. The chi-square test was used to compare log, chart, and billing data.
RESULTS
Twenty-nine WReN physicians submitted data on 572 encounters. Eighty-three percent of the encounters were with a regular patient of the physician. Twentyfive percent of the patients were 65 years of age or older, and 62% were female. These findings are comparable to data from the 2000 National Ambulatory Medical Care Survey (NAMCS), which found for all ambulatory visits that 24.3% were by patients aged 65 and older and 59.3% were by female patients.5
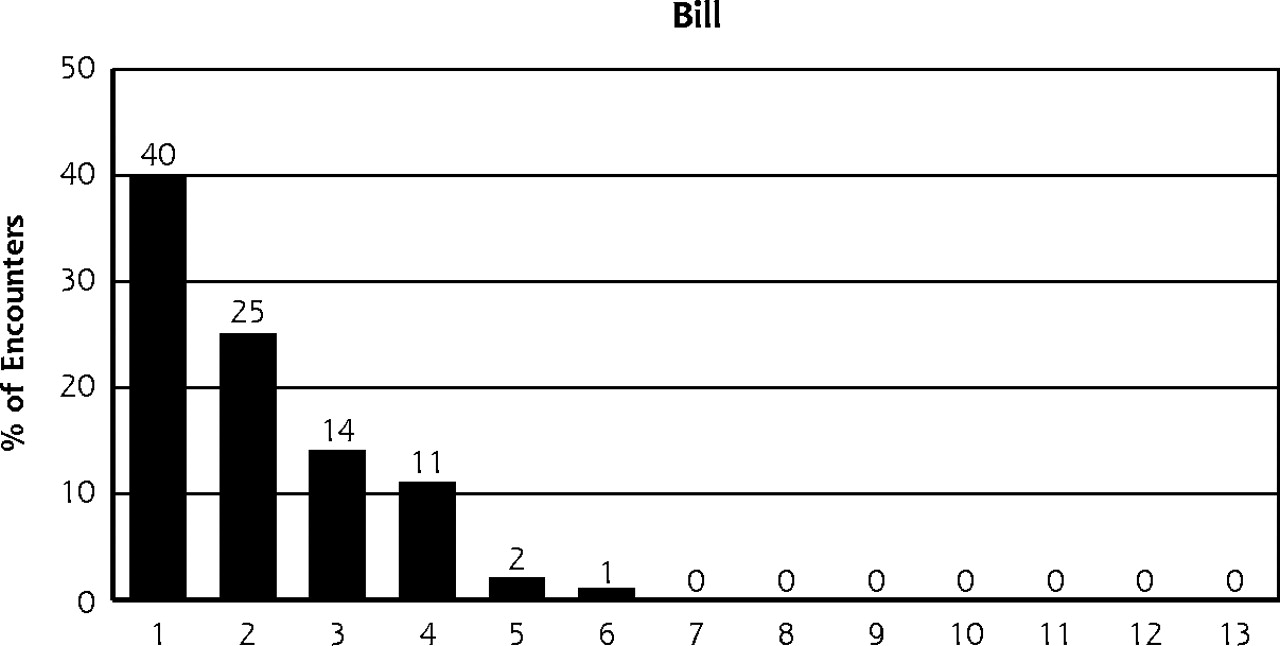
The main findings of this study for all encounters are presented in Figure 1⇓ and Table 1⇓. Table 1⇓ also includes data for patients older than 65 years and for patients with diabetes.
Number of Problems per Encounter and Percentage of Encounters With Multiple Problems
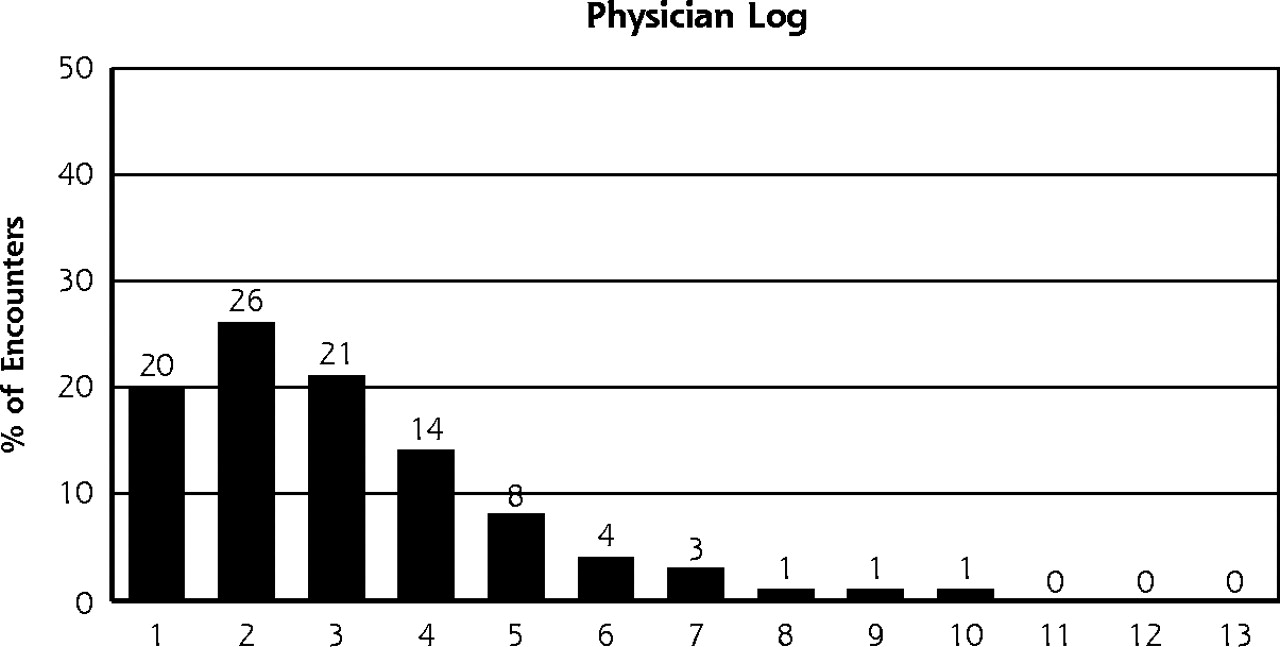
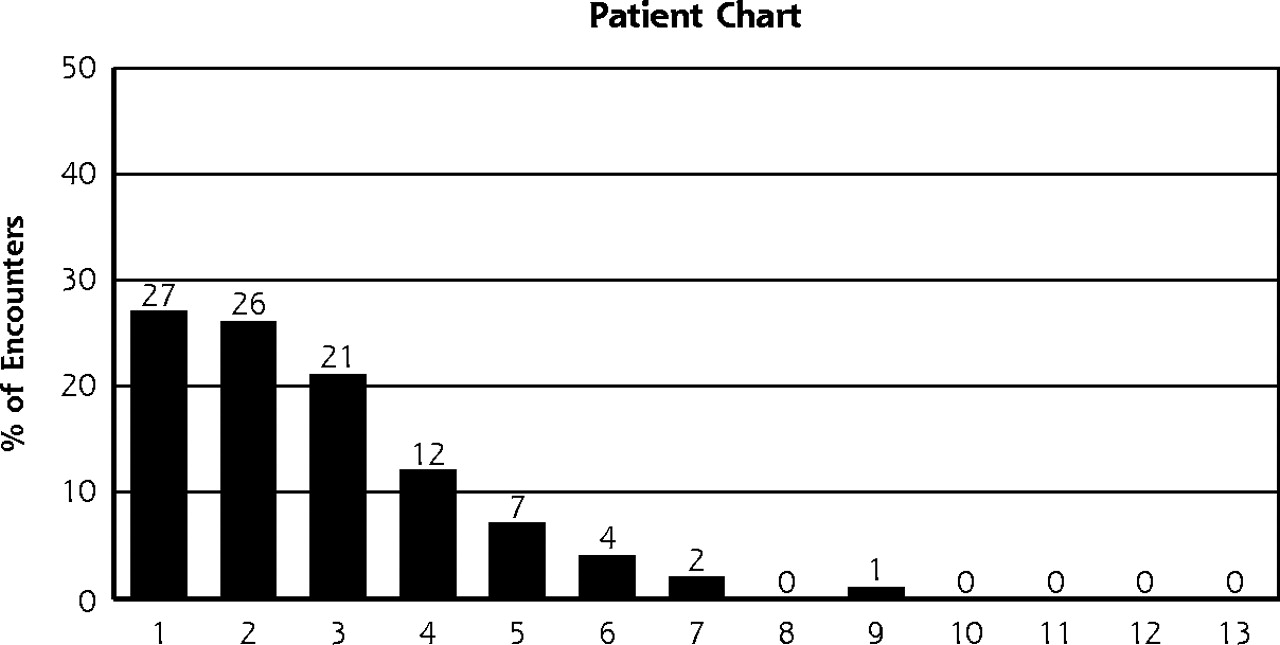

Number of problems per encounter recorded by physician log, patient chart, and bill for 573 encounters.
Of the patients for whom their sex was recorded, the 351 female patients had 3.1 problems per encounter. For the 213 male patients the average number of problems was 2.9 (P = .27, not significant).
When a physician saw his or her regular patients, an average of 3.2 problems were managed at each encounter compared with 2.4 when the patient was not a regular patient of that physician (P <.001).
Physicians reported that 7% of visits included problems related to a secondary patient. No bill was created for the secondary patient.
We examined 2 categories of problems to test the hypothesis that some problems, especially mental health and substance use and abuse problems, are less likely to appear on the bill than are routine medical problems, as has been suggested by Susman et al.6 The problem logs showed a total of 96 entries related to hypertension, and diagnoses related to hypertension appeared 74 times (77%) on the bills. In contrast,137 mental health and substance problems (including tobacco use) were listed in the log, but there were only 58 related diagnoses on the bill (42%). The difference is significant at P = .02.
In checking for the Hawthorne effect, we found that the progress notes from the study encounter averaged 2.82 problems per visit. The notes from the preceding encounter showed only 1.9 problems (SD 1.2) (P <.001).
DISCUSSION
Our study findings, as have the findings of others exploring the black box of primary care,3 have implications for assessing care, implementing guidelines, education, research, administration, and the funding of care. Our study is the first to attempt to assess the content of the primary care encounter by directly asking physicians to record in a log what problems they were addressing and then comparing this information with the usual measurements.
Measures of quality applied to primary care physicians may be inappropriate if the quality of care across all patient problems over time is not assessed. Whereas most quality assessment and improvement efforts focus on one problem at a time,7 an essential value of primary care is a comprehensive approach to identify the most important problem(s) to be dealt with on a given occasion and to prioritize, provide, and integrate care for several problems.8,9 Although the definition of primary care by the Institute of Medicine (IOM) includes comprehensiveness, the IOM does not define primary care operationally.10 It can, however, be argued that the number of problems addressed during an encounter provides one measure of the comprehensiveness of primary care services.
Understanding the concurrent management of problems helps to explain a paradox of primary care. This paradox is the finding that, compared with specialists, generalists tend to provide inferior disease-specific care11 and use fewer resources while producing similar or improved health outcomes for patients with chronic disease,12,13 and health care systems that emphasize primary care have better health status among their populations than specialist-dominated systems.14–,17 The prioritizing and integrating functions of multiproblem management may help explain why.
Our finding of an average of 3.05 problems per encounter is slightly more than what other studies have identified. One early study18 found that third-year medical students identified an average of 2.68 problems per logged encounter during the final month of a 12-week clerkship. During a year-long ambulatory care clerkship, students identified 1.97 problems per encounter with internists as preceptors, 1.32 with family physicians, and 1.21 with pediatricians.19 Using direct observation of patient care, Zyzanski et al2 found that physicians in high-volume and low-volume practices identified 1.8 and 1.9 problems per visit, respectively, with problems being defined as the number of diagnoses listed, the number of treatments listed, or a problem mentioned in the assessment or plan. Flocke and colleagues, using direct observation, found an average of 2.7 problems per encounter with family physicians; 24% of visits had more than 3, and 14% had more than 4 problems at each encounter.1
Problems involving the secondary patient were identified in 7% of the encounters in our study. Other studies have reported discussion of such problems during 18% of encounters (with no change in billing current procedural terminology [CPT] codes),14 in 16% to 20% of encounters,2 and in 6% of office encounters.20 In this latter study this care was reflected in only 5% of the bills for those visits.
Our study, among others, shows that most family medicine outpatient visits involve multiple problems, which is not accurately reflected in the number of diagnoses recorded on the bill. Similarly, Flocke and colleagues found that 58% of visits had fewer problems on the bill than were observed, with only 13% having more problems on the bill than were observed.1 Other work specifically directed at the diagnoses on the bill showed that only 69% of diagnoses in the progress note appeared on the bill and, conversely, that 22% of diagnoses listed on the bill were not addressed in the progress note.21 Two studies found only 55% to 57% concordance between the CPT code on the bill and the content of the visit, with overcoding and undercoding being equally likely.22,23
The underreporting in billing may reflect the lack of incentive to report multiple diagnoses when billing for one problem (eg, diabetes) will justify the bill, or when billing for mental health or substance use problems diagnoses pose a risk to the patient.6
One other measure of practice content, the National Ambulatory Care Medical Survey (NAMCS) data set, may also be incomplete with respect the number of problems addressed since the entry form for the NAMCS has room for only 3 problems, thus missing problems in up to one third of encounters. Analyses of family medicine based on billings and probably even the NAMCS fail to reflect completely the problem content of encounters.
The management of multiple problems is demanding for physicians. In a study of difficult patients, it was found that the factor of “the patient has many problems” had the second strongest loading of any scale for these patients24 and that the existence of (or treatment for) one problem may hinder the care of others.25
For this reason, the usefulness of guidelines that focus only on one disease may be limited. Although a reductionistic approach might improve care for the disease under scrutiny, most primary care patients have comorbid conditions for which they consult primary care physicians.26 Patients have needs for care of all their problems, acute illness or injury, chronic illness, prevention, mental health, and family problems.8 Quality improvement efforts that focus on the whole as well as the parts are needed.7
Reported shortfalls in following guidelines may be explained in part by the number and types of problems a patient brings to each visit. The competing demands of multiple problems affect mammography screening,27 the care of depression,28,29 diabetes,30 and the provision of informed consent.31,32 In the case of counseling for tobacco use, a direct observation study found that in 24% of encounters with cigarette smokers, the omission of counseling was justified by the nature of the competing problems.33 A 1999 review of the literature on issues in guideline implementation shows remarkably few studies addressing the issue of competing demands in guideline implementation.34
Our findings and those of related studies have implications for education, in that we need to direct more efforts to the issue of the effective and efficient concurrent management of multiple problems. In the same vein, researchers should not ignore the multiple problem aspect of care in the design of their studies. As a rural physician said to one of the authors (JB), “Don’t do research on diabetes. Do research on patients with diabetes!” Research on the management of multiple problems is essential if the results are to be most relevant to family medicine settings. Finally, administrators and funders need to move beyond the assumption that the bill is a reflection of the content of the patient encounter as they assess, support, and pay for patient care.
Limitations
The most obvious limitation of our study is the dependence on physician self-report. The physicians were aware of the study hypothesis, and they could have exaggerated the number of problems seen at each encounter. Indeed, that would be one hypothesis to explain why the number of problems in the chart at the index visit was higher than the number for preceding visit—an apparent Hawthorne effect. It is also possible, however, that the physicians were simply more careful when writing or dictating their notes after they had listed all the problems they addressed on the encounter problem log. The Hawthorne effect may have increased the number of problems recorded in the patient chart, which would have led us to underestimate the shortfall of the chart in recording the number of problems logged by the physicians.
Although there is room to doubt the accuracy of physician self-report,35 we hope that the immediacy of self-report, being no later than the end of the session, would lead to reasonably accurate reporting. In addition, the general concordance or our results with those found in other studies using different methods would suggest that there was no great bias.
An additional limitation of this study relates to reviewing only progress notes. Because other charted information (eg, flow sheets, problem lists, immunization records) was not assessed, we probably missed some problems in the chart audit. The chart audit was further limited because only a single individual reviewed each progress note.
Unfortunately, there is no reference standard for determining the number of problems dealt with at an encounter, as the presence of an observer can influence the process of care.36 Furthermore, even direct observation studies are limited by the inability to describe those problems that are considered by the physician but do not lead to observable actions. The issue of what problems are addressed in the physician’s mind, even if not explicit, is central to understanding this aspect of the complexity of the visit.
Finally, because this study was limited to family physicians in one state, the generalizability is limited.
CONCLUSIONS
Our study supports the hypothesis that visits to family physicians involve multiple problems, and many visits are complex, with the physician addressing more than 3 problems more than one third of the time. It further supports the hypothesis that the bill is a poor indicator of the actual content of the encounter. These findings, coupled with the findings of others in the literature, suggest a need to reconceptualize our approaches in several areas. First, quality assessment and guidelines should refocus on the entirety of patient care rather than taking a reductionistic look at disease-specific indicators. Second, education for physicians, especially those going into primary care, should move beyond traditional single-disease–oriented educational models. Third, research in family medicine, where appropriate, should address whole-patient issues rather than just single disease issues. Fourth, administrators and funders should pay more attention to the multiproblem nature of care.
Future work should improve on the generalizability of this work, paying special attention to the apparent Hawthorne effect. The work should explore the relationship between the types of problems that the physician actually deals with and the problems that appear on the bill. The work should enable the development of specific plans for improving the assessment of primary care and developing guidelines, for education of current and future physicians, for research protocols that address the entirety of patient care, and for administration and reimbursement mechanisms that support the concurrent care of multiple problems.
Acknowledgments
We thank Ms. Mary Stone for her critically important support of this project.
Study participants: Mary Arenberg, MD; Bruce Barrett, MD; Dennis J. Baumgardner, MD; John W. Beasley, MD; Rod Erickson, MD; Steve Erickson, MD; David Hahn, MD; Terry Hankey, MD; Clark Hanmer, MD; Cynthia Haq, MD; Jim Harrison, MD; Paul Hartlaub, MD; Ira Kastenberg, MD; Rex Kolste, MD; Dean Kresge, MD; Lu Marchand, MD; Mustansir Majeed, MD; James Milford, MD; Lori Neumann, MD; David Olson, MD; Scott Peschke, MD; Leon Radant, MD; Joe Ross, MD; Mary Ellen Sabourin, MD; Michael Saunders, MD; George Schroeder, MD; Jean Slane, MD; Jonathan Temte, MD; Lawrence W. Waite, DO
Footnotes
-
Conflicts of interest: none reported
-
Funding support: Grant and in-kind support were received from the Franciscan Skemp Foundation, the University of Wisconsin Department of Family Medicine, and the Wisconsin Academy of Family Physicians.
- © 2004 Annals of Family Medicine, Inc.
REFERENCES




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Family medicine teaching strategy for managing patients with comorbidity: Collect, cluster, and coordinate
- Strategie denseignement pour la prise en charge des patients presentant des comorbidites en medecine de famille: Collecte, agregation et coordination
- Unrecognised depression among older people: a cross-sectional study from Norwegian general practice
- Diagnoses per Encounter by Telephone, Televideo, and In-Office Visits
- Association of Telehealth with Short-Interval Follow-Up
- Changing Reasons for Visiting Primary Care Over a 35-Year Period
- Clustering and Healthcare Costs With Multiple Chronic Conditions in a US Cross-Sectional Study
- Much to do with nothing: microsimulation study on time management in primary care
- Family medicine, fast and slow
- Revisiting Primary Care's Critical Role in Achieving Health Equity: Pisacano Scholars' Reflections from Starfield Summit II
- The Full Scope of Family Physicians Work Is Not Reflected by Current Procedural Terminology Codes
- In This Issue: Powerful Ideas for Action
- Burden of common mental disorders in a community health centre sample
- A Primary Care Panel Size of 2500 Is neither Accurate nor Reasonable
- Capturing the complexity of first opinion small animal consultations using direct observation
- An Argument for Comprehensiveness as the "Special Sauce" in a Recipe for the Patient-Centered Medical Home
- The content of general practice consultations: cross-sectional study based on video recordings
- Estimating the Population Prevalence of Diagnosed and Undiagnosed Diabetes
- Overwhelmed Patients: A videographic analysis of how patients with type 2 diabetes and clinicians articulate and address treatment burden during clinical encounters
- Information Chaos in Primary Care: Implications for Physician Performance and Patient Safety
- Comparison of the accuracy of patients' recall of the content of telephone and face-to-face consultations: an exploratory study
- Does the evidence referenced in NICE guidelines reflect a primary care population?
- Family Medicine Outpatient Encounters are More Complex Than Those of Cardiology and Psychiatry
- Impact of EHR-Based Clinical Decision Support on Adherence to Guidelines for Patients on NSAIDs: A Randomized Controlled Trial
- Primary Care: Current Problems And Proposed Solutions
- Primary care physicians' experiences with electronic medical records: Implementation experience in community, urban, hospital, and academic family medicine
- Knowing we practise good medicine: Implementing the electronic medical record in family practice
- Savoir que nous exercons une bonne medecine: Mise en aeuvre des dossiers medicaux electroniques en pratique familiale
- State of the Science: Promoting Self-Care in Persons With Heart Failure: A Scientific Statement From the American Heart Association
- A Science of Connectedness
- How Often Do Physicians Address Other Medical Problems While Providing Prenatal Care?
- Perceived Complexity of Care, Perceived Autonomy, and Career Satisfaction Among Primary Care Physicians
- Confronting The Growing Burden Of Chronic Disease: Can The U.S. Health Care Workforce Do The Job?
- The Medical Home: Growing Evidence to Support a New Approach to Primary Care
- Global Health and Primary Care Research
- Is 'Clinical Inertia' Blaming Without Understanding? Are Competing Demands Excuses?
- In This Issue: Doctor-Patient and Drug Company-Patient Communication
- Describing Primary Care Encounters: The Primary Care Network Survey and the National Ambulatory Medical Care Survey
- Behavior-Change Action Plans in Primary Care: A Feasibility Study of Clinicians
- Randomized Controlled Trials: Do They Have External Validity for Patients With Multiple Comorbidities?
- Practice-Based Research in Primary Care: Facilitator of, or Barrier to, Practice Improvement?
- Is There Time for Management of Patients With Chronic Diseases in Primary Care?
- In this Issue: The Patient-Clinician Relationship and Practice-Based Network Research