
Article Figures & Data
Figures
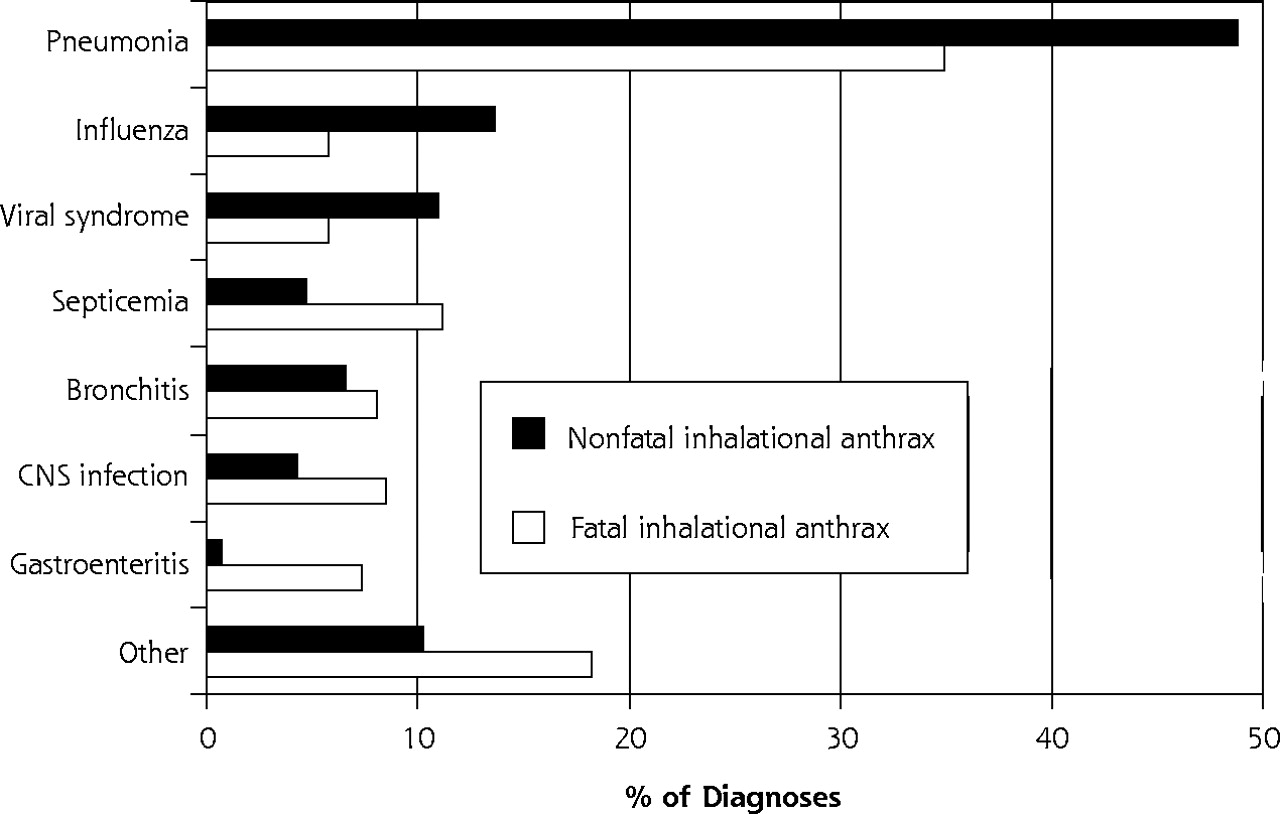
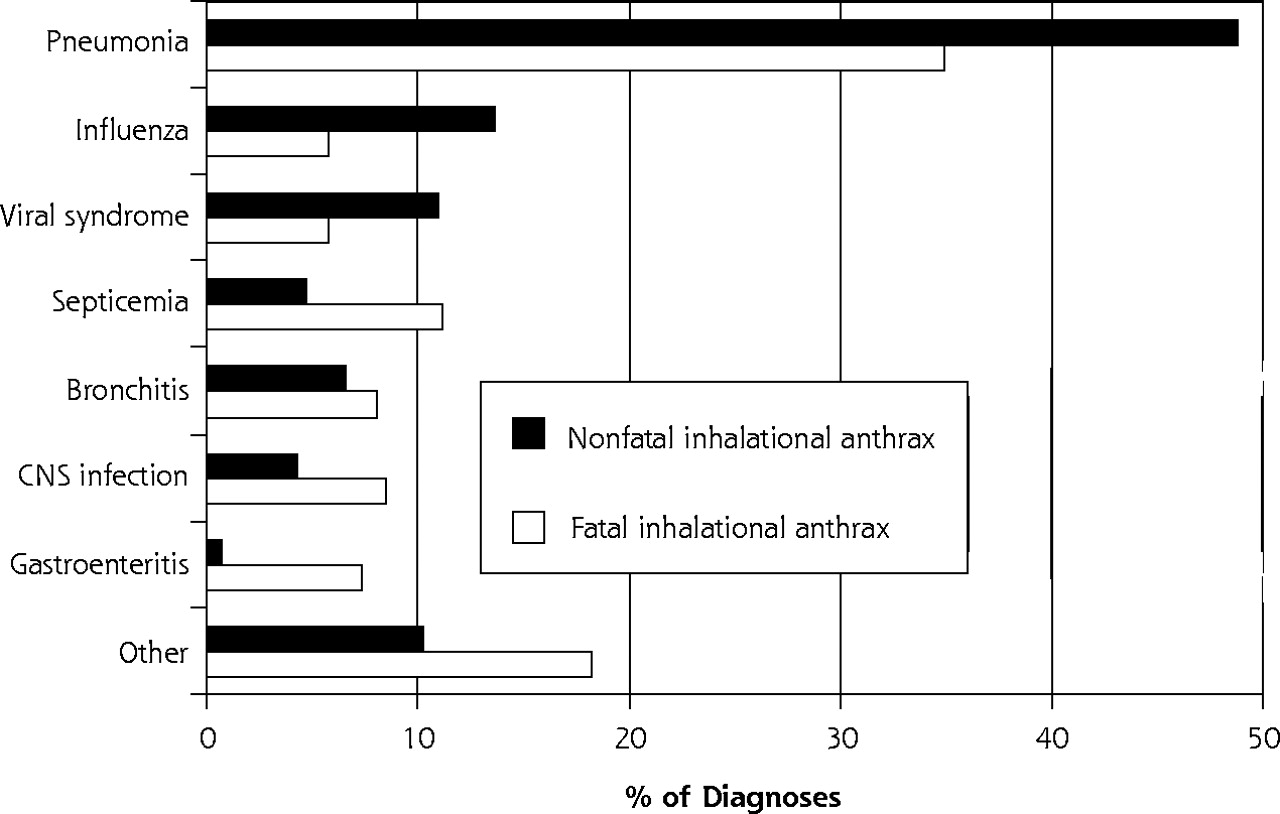
- Figure 1.
Percentage of diagnoses in each of 8 diagnostic categories assigned to cases of inhalational anthrax.
CNS = central nervous system.
Tables
Characteristic Respondents No. (%) Nonrespondents No. (%) Final Sample % P Value* * Values are for tests of differences between respondents and nonrespondents. † Men and women comprise 68.4% and 31.6% of US family physicians, respectively.17 ‡ Of US family physicians, 35.0% are located in the Eastern Seaboard region; 22.6%, in the East Central region; 19.4%, in the West Central region; 6.5%, in the Mountain region; and 16.7%, in the Pacific region.17 Sex † .235 Male 160 (35.7) 286 (64.3) 67.2 Female 78 (40.8) 113 (59.2) 32.8 Location of practice ‡ .090 Eastern Seaboard region 71 (33.5) 147 (66.5) 30.6 East Central region 60 (42.3) 82 (57.7) 24.8 West Central region 51 (34.0) 99 (66.0) 21.1 Mountain region 17 (28.3) 43 (71.7) 7.0 Pacific region 40 (45.5) 48 (54.5) 16.5 Diagnoses (ICD-9 Code) Responses No. (%) Cumulative Percentage Note: Of the nonanthrax diagnoses, 559 were from inhalational anthrax cases, 52 from Legionella cases, and 105 from the influenza cases. ICD-9 = International Classification of Diseases, 9th Revision; CNS = central nervous system. 1. Pneumonia (480-486) 237 (42.4) 42.4 2. Influenza (487) 56 (10.0) 52.4 3. Viral syndrome (079.99) 48 (8.6) 61.0 4. Septicemia (038) 43 (7.7) 68.7 5. Bronchitis (466) 41 (7.3) 76.0 6. CNS infection (047-049, 320-323) 35 (6.3) 82.3 7. Gastroenteritis (008-009) 21 (3.8) 86.1 8. Upper respiratory tract infection (460, 465) 17 (3.0) 89.1 9. Nonspecific febrile illness (780.9) 10 (1.8) 90.9 10. Chronic obstructive pulmonary disease (496) 8 (1.4) 92.3 11. Congestive heart failure (428.0) 7 (1.3) 93.6 12. Pulmonary embolism (415.1) 5 (0.9) 94.5 13. Tuberculosis (011.0-011.9) 4 (0.7) 95.2 14. Sinusitis (461.0-461.9) 2 (0.4) 95.6 15. Dehydration (276.0-276.5) 2 (0.4) 95.9 16. Syncopal episode (780.2) 2 (0.4) 96.3 17. Hantavirus pulmonary syndrome (480.8) 2 (0.4) 96.6 18. Adult respiratory distress syndrome (518.5) 2 (0.4) 97.0 19. Dementia (294.1) 1 (0.2) 97.2 20. Acute multiple sclerosis (340) 1 (0.2) 97.4 21. Pyelonephritis (590.1) 1 (0.2) 97.6 22. Diabetic ketoacidosis (250.1) 1 (0.2) 97.7 23. Angina (413.0-413.9) 1 (0.2) 97.9 24. Coxsackie virus infection (074.0-074.8) 1 (0.2) 98.1 25. Pleurisy (511.0-511.9) 1 (0.2) 98.3 26. Lyme disease (088.81) 1 (0.2) 98.5 27. Leukocytosis (288.8) 1 (0.2) 98.7 28. Interstitial pneumonitis (515) 1 (0.2) 98.8 29. Mononucleosis (075) 1 (0.2) 99.0 30. Pericarditis (420.0-420.99) 1 (0.2) 99.2 31. Empyema (510) 1 (0.2) 99.4 32. Aortic dissection (441.0-441.9) 1 (0.2) 99.6 33. Plague (Yersinia pestis) (020.0-020.9) 1 (0.2) 99.7 34. Tularemia (021.0-021.8) 1 (0.2) 99.9 35. Intestinal perforation (569.83) 1 (0.2) 100.0 Total 559 (100) - Table 3.
Initial Diagnosis Provided for Cases of Fatal and Nonfatal Inhalational Anthrax, Legionella Pneumonia, and Influenza A, and Family Physicians’ Responses to Clinical Case Vignettes
Family Physicians’ Responses Case No. Type Initial Diagnosis Reported 3, 7 No. Most Common Diagnosis Second Most Common Diagnosis Note: The first and second most common hypothetical diagnoses are provided. For summary categories, the total numbers of responses and top 3 hypothetical diagnoses are provided. The number of cases include 9 “anthrax” diagnoses and 7 cases for which the diagnosis was not listed. FIA = fatal inhalational anthrax; CNS = central nervous system; CHF = congestive heart failure; NFIA = nonfatal inhalational anthrax; LEG = Legionella pneumonia; INF-A = influenza A; URI = upper respiratory infection. * Initial diagnoses of inhalational anthrax were based on workplace exposure. † All 11 fatal and nonfatal cases. Inhalational anthrax cases Fatal 1 FIA Meningitis 56 CNS infection Sepsis 6 FIA Viral syndrome 52 Pneumonia Bronchitis 8 FIA Gastroenteritis 48 Gastroenteritis Viral syndrome 12 FIA CHF 60 Pneumonia CHF 14 FIA Viral syndrome 48 Pneumonia Influenza Overall FIA . . . 264 Pneumonia, sepsis, and CNS infection Nonfatal 3 NFIA Pneumonia 46 Pneumonia Septicemia 4 NFIA Inhalational anthrax* 61 Pneumonia Bronchitis 5 NFIA Inhalational anthrax* 45 Pneumonia Influenza 9 NFIA Viral syndrome 54 Influenza Pneumonia 10 NFIA Inhalational anthrax* 40 Pneumonia Influenza 11 NFIA Bronchitis 61 Viral syndrome Pneumonia Overall NFIA . . . 307 Pneumonia, influenza, and viral syndrome Total† . . . 571 Pneumonia, influenza, and viral syndrome Other cases 2 LEG Pneumonia 53 Pneumonia Sepsis 7 INF-A Influenza 50 Pneumonia Bronchitis 13 INF-A Influenza 58 URI Bronchitis
Supplemental Appendix
Appendix 1. Study instrument: letter of introduction and clinical case histories.
Files in this Data Supplement:
- Supplemental data: Appendix 1 - PDF file, 8 pages, 98 KB
The Article in Brief
Inhalational anthrax is a very rare infectious disease that resembles many other common diseases, such as influenza, pneumonia, and acute bronchitis. Because of this resemblance, patients are likely to go to their primary care doctors when anthrax symptoms arise. The resemblance to other diseases also makes inhalational anthrax difficult to diagnose. Primary care doctors have a key role to play in recognizing and responding to bioterrorism events, such as inhalational anthrax, and should be included in educational efforts for such events.




{kind=link}
Jump to section
Related Articles
Cited By...
- Soil-Related Bacterial and Fungal Infections
- In this Issue: The Patient-Clinician Relationship and Practice-Based Network Research
- Rapid Assessment of Agents of Biological Terrorism: Defining the Differential Diagnosis of Inhalational Anthrax Using Electronic Communication in a Practice-Based Research Network