
Article Figures & Data
Figures
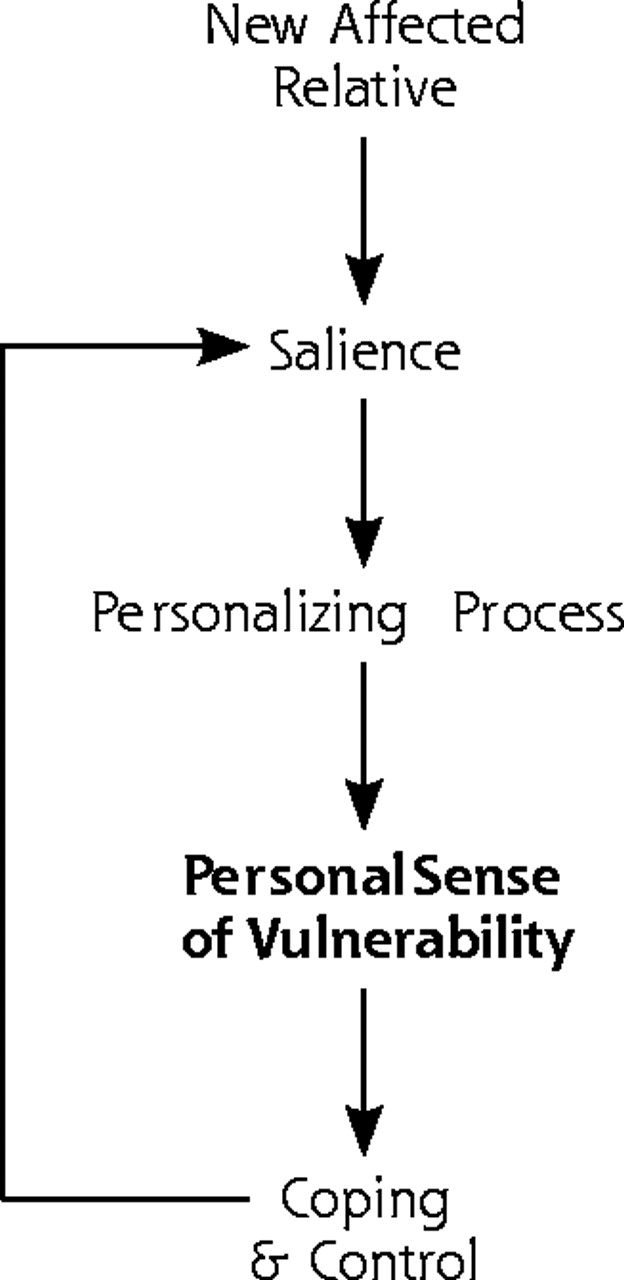
- Figure 1.
Third-order constructs and their interrelationships: a theoretical framework of how persons with familial risk develop and manage their personal sense of vulnerability.

Tables
FDR = first-degree relative; HD = heart disease. 1. Does this article report on findings from qualitative research, and did that work involve both qualitative methods of data collection and data analysis? YES/NO 2. Is the research relevant to the synthesis topic? YES/NO 3. Aims What are they? Is there a clear statement of the aims of the research? 4. Methods Types/s of methods: Is a qualitative method appropriate? 5. Sampling Inclusion and exclusion criteria: 5.1 Is it clear where the sample was selected from? Characteristics: 5.2 Is it clear why this setting was chosen? Age: Mean age: _____ SD: _____ Range: _____ 5.3 Is it clear who was selected? Gender: Women: _____Men: _____ 5.4 Is the sample selection appropriate and justified? Subjects: Patient _____ FDR _____ Other _____ Other family member _____ 5.5 Is it clear how the sample was selected? 5.6 Is the sample size justified? Disease: Cancer _____ HD _____ Diabetes _____ 5.7 Is it clear how many people accepted or refused to take part in the research? Ethnicity: 5.8 Is it clear why some participants chose not to take part? Educational level: 5.9 Is adequate information given on the characteristics of the people in the sample? Socioeconomic status: 6. Data collection Describe setting: 6.1 Is it clear where the setting of the data collection was? 6.2 Is it clear why that setting was chosen? 6.3 Is it clear how the purpose of the research was explained and presented to the participants? 6.4 Is it clear how the data were collected? 6.5 Is it clear how the data were recorded? 6.6 Is it clear whether the methods were modified during the process, and if so, why? 6.7 Is it clear who collected the data? 7. Data analysis 7.1 Is it clear how the analysis was done? Outline analysis: 7.2 Is it clear how the categories/themes were derived from the data? 7.3 Is there adequate description? 7.4 Have attempts been made to feed results back to respondents? 7.5 Have different sources of data about the same issue been compared where appropriate (triangulation)? 7.6 Was the analysis repeated by more than one researcher to ensure reliability? 8. Research partnership relations 8.1 Is it clear whether the researchers critically examined their own role, potential bias, and influence? 8.2 Has the relationship between researchers and participants been adequately considered? 9. Justification of data interpretation 9.1 Are sufficient data presented to support the descriptive findings? 9.2 Are quotes numbered/identified? 9.3 Do the researchers explain how the data presented in the article were selected from the original sample? 9.4 Do the researchers indicate links between data presented and their own interpretations of what the data contain? 9.5 Are negative, unusual, or contradictory cases presented? 9.6 Is there adequate discussion of the evidence both for and against the researchers’ interpretations? 10. Transferability 10.1 Is there conceptual and/or theoretical congruence between this and other work? 10.2 Are the findings of this study transferable to a wider population? 11. Findings 11.1 Is it possible to summarize the findings? 11.2 Were the findings explicit and easy to understand? Total score (of 36 criteria) - Table 2.
Grid Displaying First-Order Constructs (Key Concepts) Grouped Within Emerging Second-Order Constructs (Main Themes), by Study and Disease
Mean Appraisal Score* (Range) Diseases in My Family Experience of Relative’s Illness Personal Models of Disease Personalizing Risk Control of Familial Risk FH = family history; FDR = first-degree relative; HD = heart disease; DM = diabetes mellitus. * Total score = 36. † Pilot scores - consensus. Brorsson et al, 1995; hypercholesterolemia (HD) 22 19† “My family gets heart attacks.” Including nongenetic family members Perceived threat inherent in the association between hypercholesterolemia and the event in the FH Seriousness associated with fatal events, disability, and premature deaths Time lag since FH of event less important Chalmers & Thompson, 1996; cancer (breast) 23 23† “Walking in relative’s path” “Living the cancer experience” “Developing a risk perception”: comparing aspects of personality, lifestyle, and body type; appraising own threatening experiences with breast abnormalities; personalizing the risk, variable, intuitive or reasoned “Putting risk in its place”: controlling what one can; rehearsing one’s own cancer; “finding the best time” as emotional control over risk perception; adopting self-care practices Amount of sharing of cancer experience: close attachment leads to greater shared experience Phase and variability of illness trajectory: complicated illness leads to greater salience Witnessing suffering: the physical and psychosocial impact Emery et al, 1998; cancer (colorectal) (CRC) 24 26.25† Understanding genetics differs from scientific explanation Reconstructed risk according to personal and family experiences, and personal understanding of inheritance Personalization of risk provides framework for control of own and family member’s risk “Risk framework” allows person to combine genetic and environmental risk and assess risk to offspring Green et al, 1993; cancer (ovarian) 25 18.3 (17–19) Ovarian cancer “in the family” Awfulness of mother’s disease, rather than personal risk, especially among women whose mothers had recently died Idiosyncratic use of genetic terms Dominant concept of proneness or vulnerability, especially to illness experienced by close relative of same sex Lack of control, powerless Relatively young age and dependent children of affected relatives particularly upsetting Personal experience showed ovarian cancer likely to prove fatal if not detected early Little understanding of genetic component of risk; also due to shared exposure to common risk factors Similarities with unaffected parent could protect No obvious controllable risk factors. Some considered removal of ovaries Women whose mother had died recently showed more anxiety Models of familial disease did not follow Mendelian genetics Asymptomatic phase of disease Few realized ovarian cancer could pass through the male line Positive about screening: “has to be better than nothing” Peaks and troughs of anxiety, eg, before screening, approaching age of diagnosis of relative General fear of cancer. Concern for daughters Harris et al,1998; CRC 26 22 (21–23) At risk if relative (not just FDR) had had CRC despite relative’s age. Magnitude of family history and death of relative increase seriousness of FH Determinants of risk: genetic predisposition, environmental risks, increasing age, other cancer, low-fiber diet, “bad luck.” Concept of risk factors that trigger cancer, such as sunlight, constipation, pollution, shock Perceived personal susceptibility due to FH Screening seen as effective, although there was limited understanding Variable access to family history information Fear and older age were barriers to screening Hunt et al, 2000; HD 27 25.3 (23–27) HD viewed as family condition, with perceived FH more than number of cardiac events in family Even with several affected relatives, some thought HD due to chance. All mentioned heredity Distinction made between inherited risk within family as a whole and personal risk Factors encouraging more healthy behavior: bodily markers of decline, health events, having children, financial stimuli, and enjoyment Relationships, ages, and pattern of death add to importance, with age at death always mentioned Complex mechanism: biological and social Stressed differences from affected relatives to downplay risk Barriers to change: uncertainty, image of HD as “a good way to go,” past material and cultural circumstances, costs, time constraints, lack of motivation Variable notion of premature death, and variable amount of FH information available Notions of candidacy Effects of gender and social class Cardiac deaths of elderly relatives often discounted. Counter examples discussed, eg, fit young relatives “dropping dead” Hunt et al, 2001; HD 28 17.5 (17–18) Number of affected relatives, their age, and relationship Genes or heredity mentioned as cause by more than 2/3 Distinction made between inherited risk within family as a whole, and personal risk Often highly ambivalent about FH More weight given to deaths in FDRs, especially parents Death of one (or more) relatives could be due to chance Stressed differences from affected relatives to downplay risk, eg, smoking, taking after other side of family. Many continue wrestling with decisions about modifying behavior, especially weight and effects of age Patterns of death, eg, age of death Search for patterns to indicate heredity, eg, number of relatives with HD on one side of family Variable notion of premature death Men from manual socioeconomic groups required greater number of affected relatives to perceive FH Incomplete knowledge of FH could lead to ambivalence McAllister et al, 1998; cancer (breast) 29 22 (22) Awareness that breast cancer may be inherited Close involvement often distressing Awareness of inheritance Used inheritance of other characteristics, often following gender-specific pattern, to explain why not at personal risk Continuing anxiety, especially about own and daughter’s risk Variable access to family history information; often avoided. Men often excluded from female illness discussions Multifactorial model: not attributed solely to inheritance, also environmental risks such as smoking (Potential) daughters at higher risk because of FH; no concerns about (potential) son’s health Avoidance of, or exclusion from, discussions about breast cancer “Girl’s problem,” which most men colluded with Michie et al, 1996; cancer (colorectal: familial adenomatous polyposis) 30 25 (25) Young relatives die, undergo operations, or experience pain Multifactorial models of genetic disease: all mentioned genes, although uncertainty about role; some aware of environmental causes. Proneness, vulnerability not a problem Some: “there is no problem” “Genes as a black box.” Screening seen as aversive, but important: “a necessary evil,” “seeing is believing” Lay models of Mendelian inheritance Vagueness about genetic testing: little evidence of informed decision making Uncertainty of not being diagnosed “Functional pessimism” to cope Ryan & Skinner,1999; cancer (breast) 31 17.5 (17–18) FH a risk factor, although most did not appreciate differences in risk depending on age of relative Multifactorial model: lifestyle risks almost equal to familial risk; high-fiber diet or stress may be more important Personalizing risk process Screening could cause cancer Misunderstandings about risk factors: environmental toxins and drugs thought influential Proneness, vulnerability Wanted thorough analysis of risk, then recommendations for lowering risk. Fewer than one half wanted to know genetic susceptibility status: many concerns. Risk modification by lifestyle changes welcomed Feelings of fatalism Discounted risk information if affected relative had protective characteristic or no risk factors Shepherd et al, 2000; type 2 diabetes mellitus (AODM) 32 14 (13–15) Four generations of family had 14 affected family members. DM regarded as serious disease within family Witnessing suffering of grandfather Causes included chutney and germs contracted while in prisoner-of-war camp. Personal models of inheritance, such as youngest child, or alternate generations. Genetic information too complicated. Mental pictures of genes Physical resemblance of family members linked to those thought likely to develop DM Disease Location Setting Sample No. and Sex Age Range Years Methods IHD = hypercholesterolemia; FDR = first-degree relative; UKCCCR = United Kingdom Coordinating Committee on Cancer Research; FAP = familial adenomatous polyposis; MODY = maturity-onset diabetes of the young; n/a = not available; HD = heart disease. Brorsson et al, 1995 22 Hypercholesterolemia (HD) Malmo, Sweden Health Survey Study at Primary Health Care Centre: men with moderately elevated cholesterol levels 63 men 35–45 Interview Chalmers & Thompson, 1996 23 Cancer (breast) Winnipeg, Canada FDRs of women with breast cancer: multiple recruitment strategies 55 women 18 ≤50 37 ≤50 Interview Emery et al, 1998 24 Cancer (colorectal) Wessex, UK Referrals to family cancer genetics clinic 11 women 6 men 28–86 mean 52 Interview Green et al, 1993 25 Cancer (ovarian) Cambridge, UK Self-referrals to UKCCCR Familial Ovarian Cancer Register 20 women 33–72 (most in 40s) Interview Harris et al, 1998 26 Cancer (colorectal) Newcastle, NSW, Australia Random sample (at least 1 affected FDR) from surveillance file of colorectal surgeon 12 women 12 men 40–70 mean 50 4 focus groups Hunt et al, 2000 27 HD West Scotland, UK Purposively sampled health study respondents (FASTCARD) 31 women 30 men 41–51 Interview Hunt et al, 2001 28 HD West Scotland, UK Purposively sampled health study respondents (FASTCARD) 31 women 30 men 41–51 Interview McAllister et al, 1998 29 Cancer (breast) Dublin, Ireland, UK Men with at least 1 affected FDR identified from oncology clinic 22 men 25–60 Interview Michie et al, 1996 30 Cancer (colorectal, FAP) London, UK From Polyposis Register of specialist hospital 12 women 8 men 15–46 mean 27 Interview Ryan & Skinner 1999 31 Cancer (breast) Missouri, USA FDRs of recent patients at oncology clinic 29 women 22–65 mean 40 4 focus groups Shepherd et al, 2000 32 Diabetes (MODY) Exeter, UK MODY-affected family and health professionals from secondary care n/a n/a Case study - Table 4.
Implications for Practice: Key Areas for Clinicians to Explore With Patients That Might Improve Risk Assessment Communication and Disease Management Strategies
Constructs Key Areas Salience Number of affected relatives Affected relative’s age at diagnosis or death Severity of illness: premature death or disability Acknowledging familial risk Influence of gender, class, ethnic group Living through relative’s illness experience Shared environment with affected relative Counting and discounting familial events Comparing similarities and differences with affected relatives Patterns within family history, eg, ages, gender, etc Personalizing process Models of health and illness Models of disease causation Models of inheritance Notions of bad luck and fatalism Personal sense of vulnerability Behavior change, eg, lifestyle risk factors Undergoing disease screening Acceptability of disease as illness or mode of death Continued anxiety
The Article in Brief
In an effort to prevent disease, health professionals often ask patients about their family history of cancer, heart disease, and diabetes. Knowing the number of family members who had a disease and their age at illness and death can help determine whether a patient is at greater risk for that disease. Patients also consider these factors when thinking about their risk for diseases, but they consider other factors as well. These include such factors as their similarity and emotional closeness to the ill relative, and their experience of the relative's illness. As health professionals learn more about genetic risks for disease, it is important that they explore ways in which patients understand and feel at risk for inherited disease.
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- Advancing the communication of genetic risk for cardiometabolic diseases: A critical interpretive synthesis
- How do people of South Asian origin understand and experience depression? A protocol for a systematic review of qualitative literature
- Association Between Causal Beliefs and Shoe Wearing to Prevent Podoconiosis: A Baseline Study
- The NHS Health Check programme: implementation in east London 2009-2011
- Inaccurate Risk Perceptions and Individualized Risk Estimates by Patients with Type 2 Diabetes
- Experienced Continuity of Care When Patients See Multiple Clinicians: A Qualitative Metasummary
- Knowledge, Perception, and Behaviors of Relatives of People With Premature Heart Disease: A Systematic Literature Review
- Family history in primary care: understanding GPs' resistance to clinical genetics -- qualitative study
- Thou shalt versus thou shalt not: a meta-synthesis of GPs' attitudes to clinical practice guidelines
- Perceived Risk of Colorectal Cancer: Sources of Risk Judgments
- How should public health professionals engage with lay epidemiology?
- Perceived Vulnerability to Heart Disease in Patients with Familial Hypercholesterolemia: A Qualitative Interview Study
- 'Coming Down the Line'-- Patients' Understanding of Their Family History of Common Chronic Disease
- "Our community of reflective practitioners will continue its quest informed...."
- How Do People Interpret Their Family Histories of Diabetes, Coronary Disease, or Cancer?
- In This Issue: New Model Finances, Systematic Reviews, Patients and Health Care