
Article Figures & Data
Figures
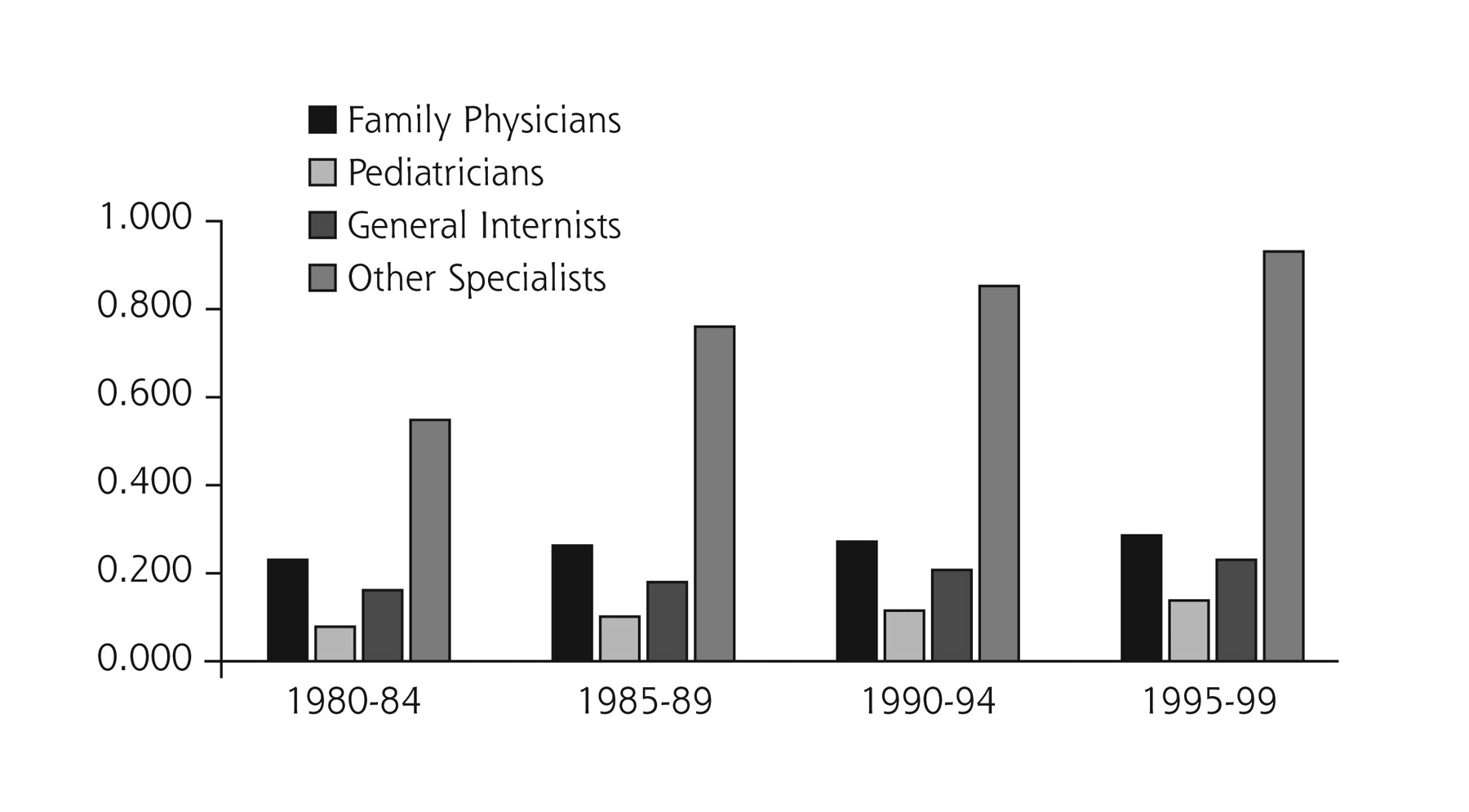
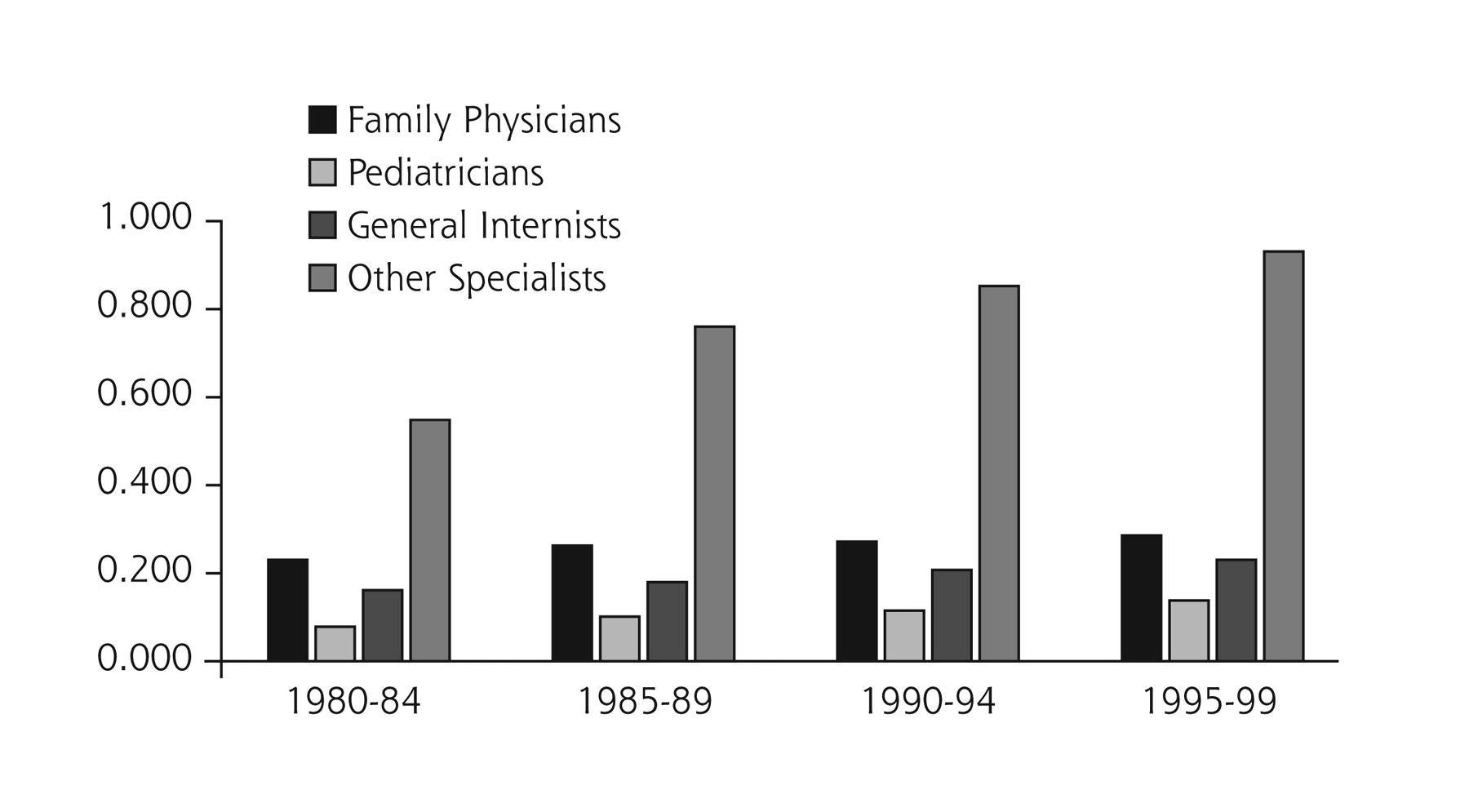
- Figure 1.
Number of office-based physicians per 1,000 people in the United States
Source: the Robert Graham Center, Washington, DC.
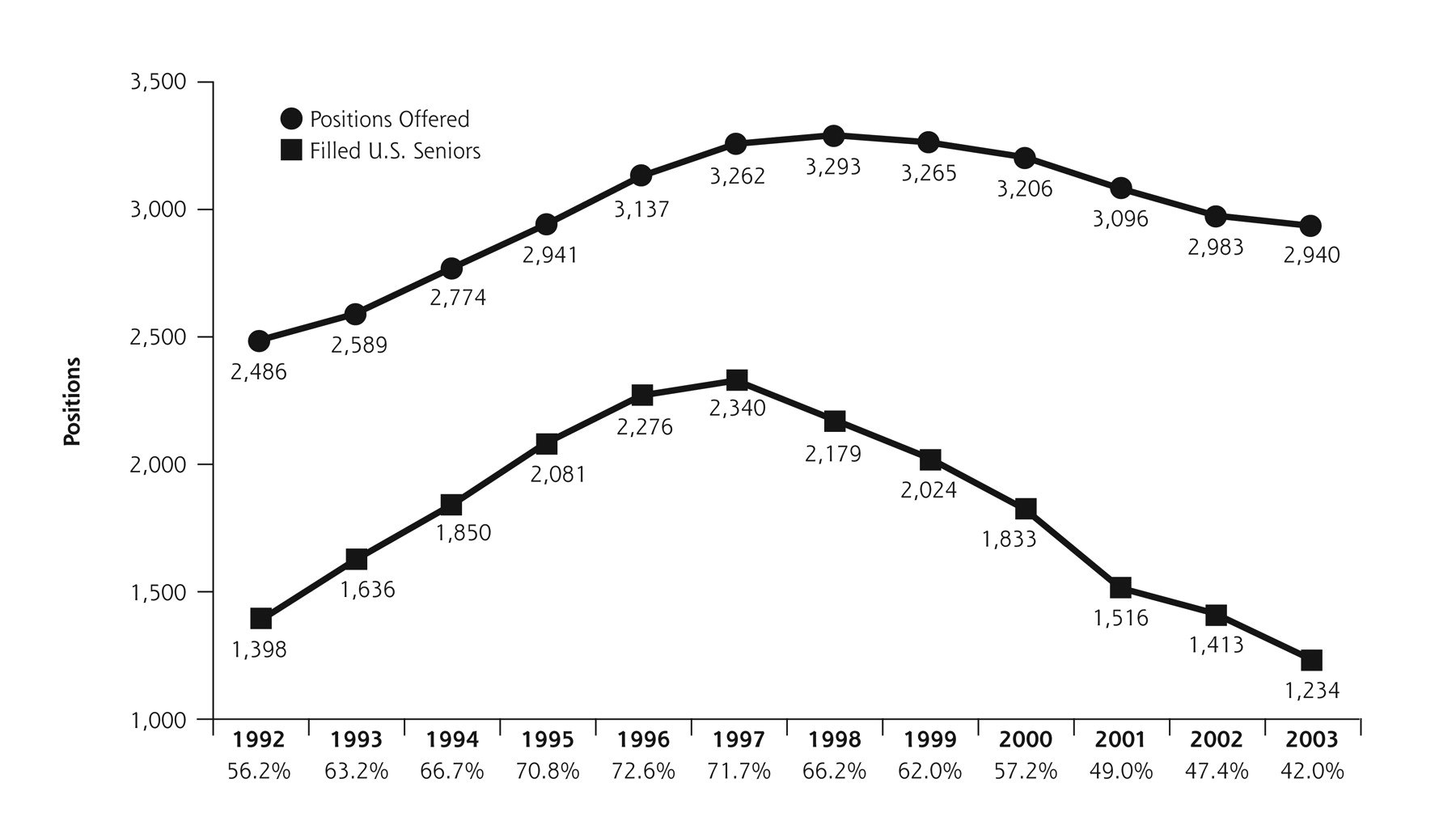
- Figure 2.
Positions offered and filled with US seniors in March 1992–2003.
Source: American Academy of Family Physicians, Leawood, Kan.
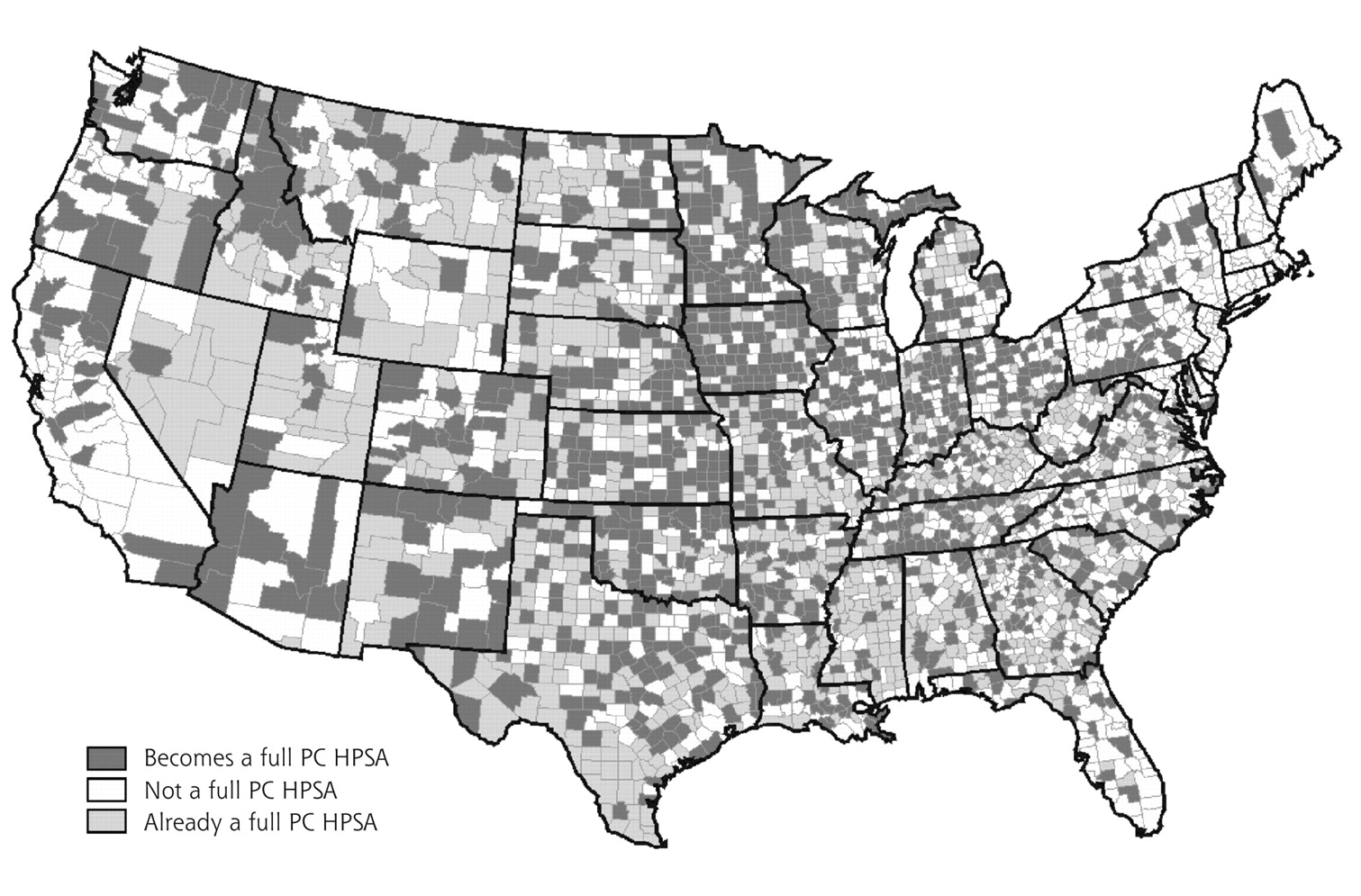
- Figure 3.
Simulation of whole county primary care health professions shortage areas (PCHPSAs) without family physicians (FPs) in 1999.
PC = primary care; FP = family physicians; HPSA = health professional shortage area. Source: The Robert Gaham Center: Policy Studies in Family Practice and Primary Care.
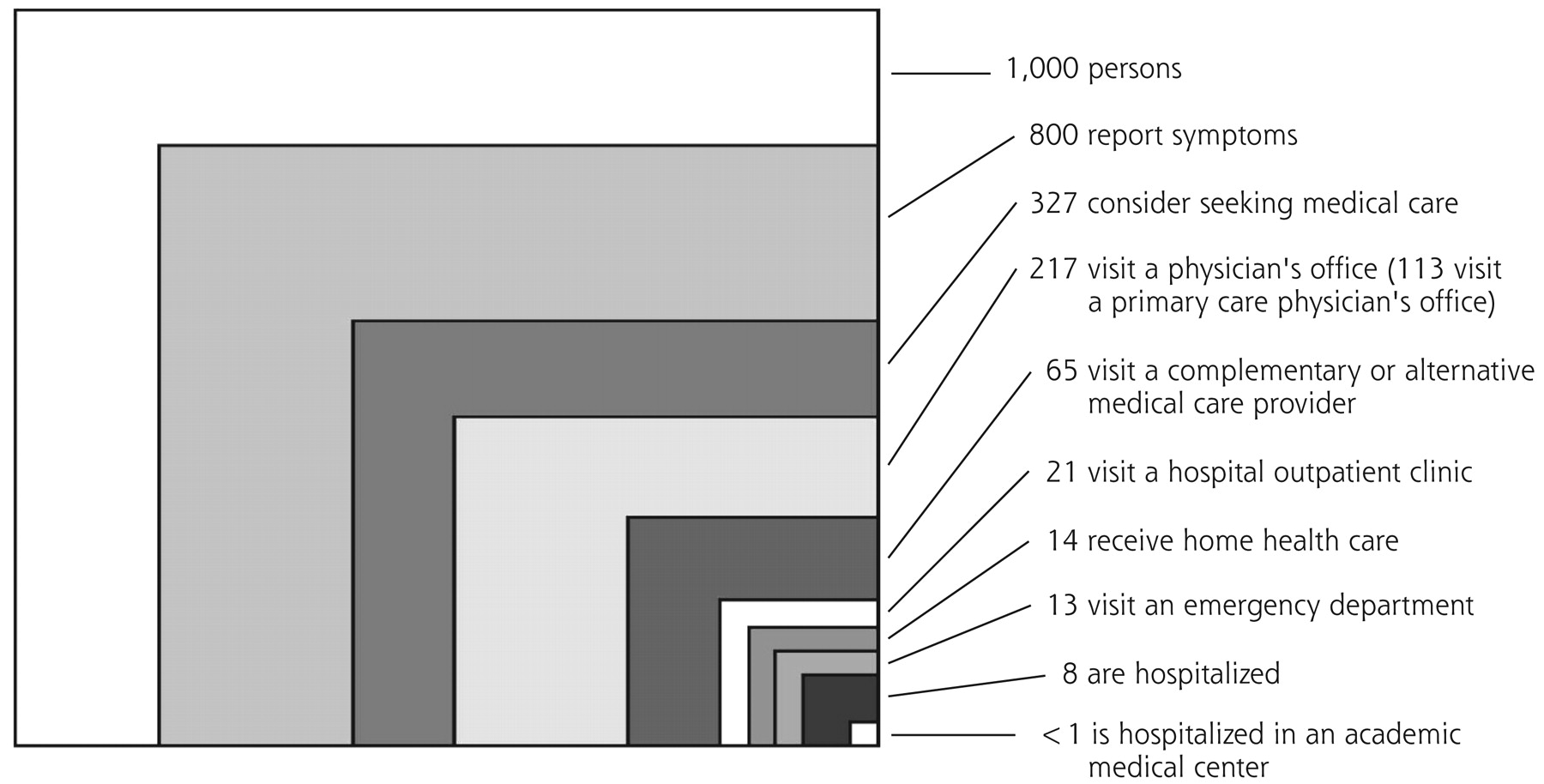
- Figure 4.
The ecology of medical care revisited.
Note: All numbers refer to discrete individual persons and whether or not they received care in each setting in a typical month. From: Green LA, Fryer GE Jr, Yawn BP, Lanier D, Dovey SM. The ecology of medical care revisited. N Engl J Med. 2001;344:2021–2025. Reprinted with permission from the Massachusetts Medical Society.
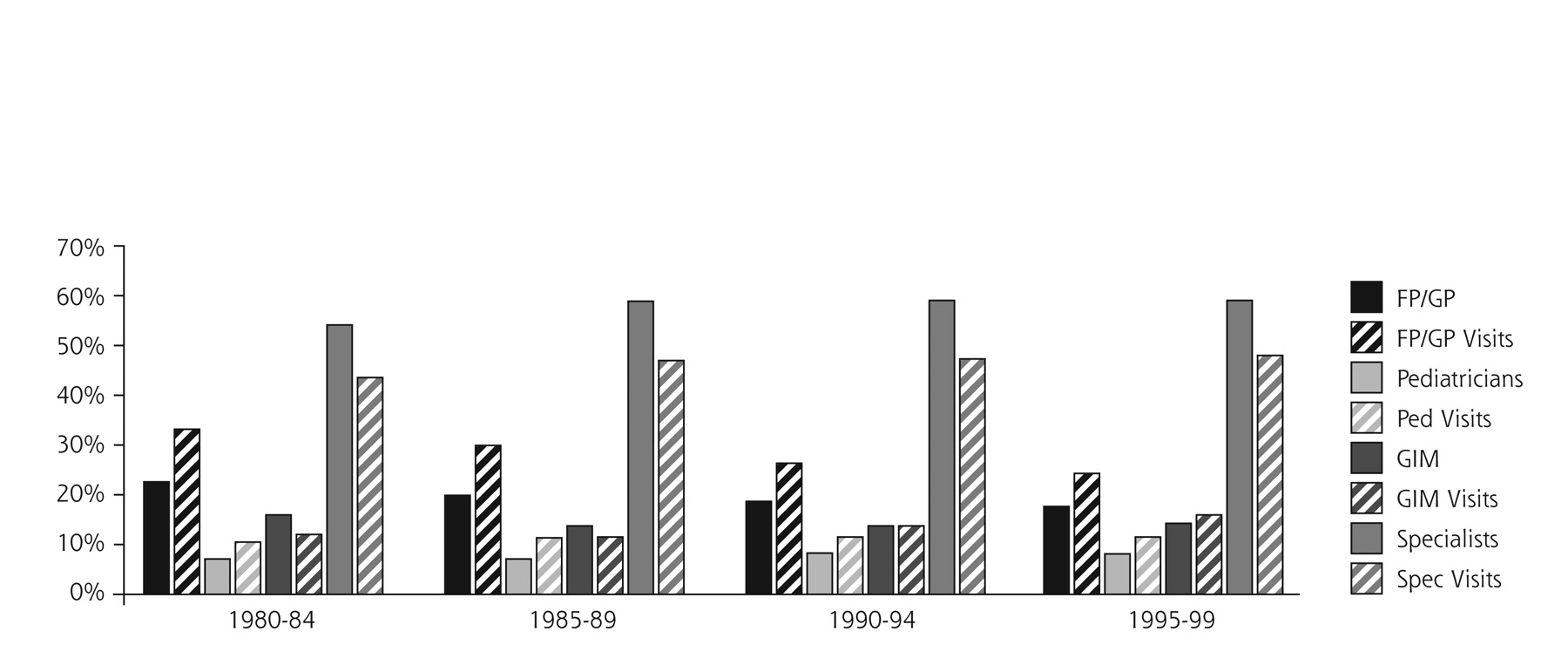
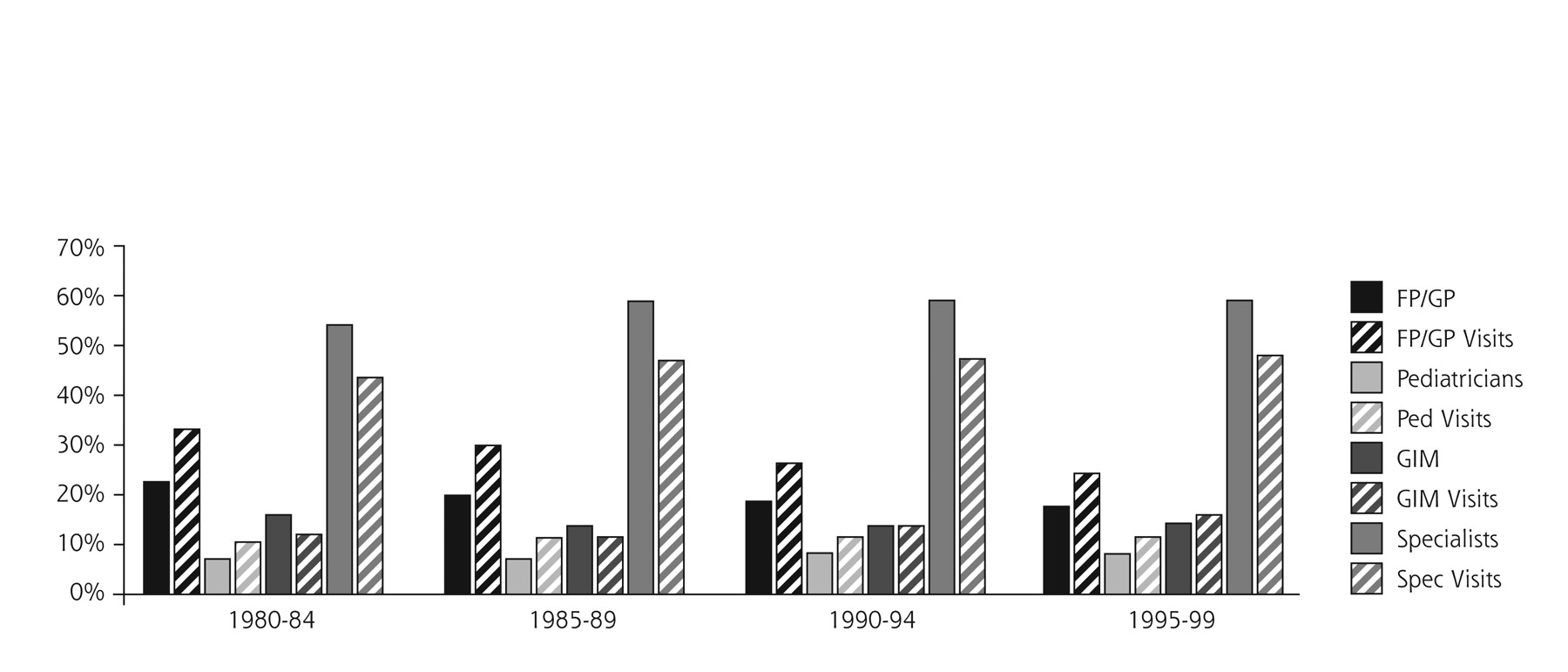
- Figure 5.
Percentage of physician population compared with percentage of visits seen.
Source: American Medical Association Physician Masterfile and the National Ambulatory Medical Care Survey.



Tables
Source: Institute of Medicine. Crossing the Quality Chasm: A New Health System for the 21st Century. Washington, DC: National Academy Press, 2001. Safe—Avoiding injuries to patients from the care that is intended to help them Effective—Providing services based on scientific knowledge to all who could benefit and refraining from providing services to those not likely to benefit Patient-centered—Providing care that is respectful of and responsive to individual patient preferences, needs, and values, and ensuring that patient values guide all clinical decisions Timely—Reducing waits and sometimes harmful delays for both those who receive and those who give care Efficient—Avoiding waste, including waste of equipment, supplies, ideas and energy Equitable—Providing care that does not vary in quality because of personal characteristics such as gender, ethnicity, geographic location, and socioeconomic status Current Approach New Rule Source: Institute of Medicine. Crossing the Quality Chasm: A New Health System for the 21st Century. Washington, DC: National Academy Press, 2001. Care is based primarily on visits Care is based on continuous healing relationships Professional autonomy drives variability Care is customized according to patient needs and values Professionals control care The patient is the source of control Information is a record Knowledge is shared and information flows freely Decision making is based on training and experience Decision making is evidence-based Do no harm is an individual responsibility Safety is a system property Secrecy is necessary Transparency is necessary The system reacts to needs Needs are anticipated Cost reduction is sought Waste is continuously decreased Preference is given to professional roles rather than the system Cooperation among clinicians is a priority Generating an understanding of family practice. Despite its 30-year history, neither the general public nor health care professionals understand all that family practice represents Organizing individuality. There is significant variance in practice scope from one family physician to the next. As a specialty, family medicine has deliberately resisted specific definition from the beginning Winning respect in academic circles. Family medicine suffers as a result of not having gained the respect and resultant endorsement of key academic institutions. Some medical schools feel that family medicine will bring neither money nor recognition to the school; as a result, they neither support the specialty nor encourage students to pursue it Making family medicine an attractive career option. Issues requiring attention include: inadequate remuneration, little recognition in the medical field, managed care challenges, quality of care yielding to pressures to increase the quantity of visits, and specialists thinking general internists are better diagnosticians than family physicians Addressing the obsession with science and technology in the United States. Family medicine is associated with neither; some people think family physicians are old-fashioned and cannot handle more critical health issues. There is a conspicuous absence of family medicine breakthrough research Category Number Source: The Robert Graham Center, Washington, DC. Family physicians/general practitioners 86,321 (71,106 FP+15,215 GP) General internists 70,362 General pediatricians 39,176 Osteopathic family physicians/general practitioners 28,407 Nurse practitioners 102,829 Physician assistants 45,311 - Table 5.
Distribution by Specialty of the Usual Source of Care for People With Selected Conditions and a Physician as That Usual Source
Condition Family Medicine % General Internal Medicine % General Pediatrics % All Others % Note: Based on 1996 Medical Expenditure Panel Surveys. Arteriosclerotic cardiovascular disease 56 31 0.0 14 Stroke 56 34 0.9 9 Hypertension 63 28 0.2 8 Diabetes 67 23 0.6 10 Cancer 60 26 2.3 11 Chronic obstructive pulmonary disease 62 22 5.4 11 Asthma 58 15 20.8 6 Anxiety, depression 62 20 7.0 11 - Table 6.
Proportion of Visits to Family Physicians and General Practitioners for Selected Problems
Problem 1980–1992 1993–1999 Source: Based on National Ambulatory Medical Care surveys, National Center for Health Statistics, US Public Health Service. General examination 40 37 Pharyngitis 48 41 Otitis Media 30 24 N1 pregnancy 18 10 Contraception 23 21 Menopause 31 16 Asthma 28 26 Diabetes 41 34 Obesity 62 48 High blood pressure 49 41 Migraine 38 34 Benign prostatic hypertrophy 8 15 Depression 39 39 All 30 25 Characteristic Description A deep understanding of the dynamics of the whole person This approach leads family physicians to consider all the influences on a person’s health. It helps to integrate rather than fragment care, involving people in the prevention of illness and the care of their problems, diseases, and injuries A generative impact on patients’ lives This terminology comes from Erik Erikson’s work on personality development. Family physicians participate in the birth, growth, and death of people and want to make a difference in the lives of their patients. While providing services that prevent or treat disease, family physicians foster personal growth in individuals and help with behavior change that may lead to better health and a greater sense of well-being A talent for humanizing the health care experience The intimate relationships family physicians develop with many of their patients over time enables family physicians to connect with people. This ability to connect in a human way with people allows family physicians to explain complex medical issues in ways that people can understand. Family physicians take into account the culture and values of their patients, while helping them get the best care possible A natural command of complexity Family physicians are comfortable with uncertainty and complexity. They are trained to be inclusive, to consider all the factors that lead to health and well-being—not just pills and procedures A commitment to multidimensional accessibility This means not only to be physically accessible to patients and their families and friends, but to maintain open, honest, and sharing communications with all involved with the care process Characteristics Description Patient-centered care Patients are active participants in their health and health care. The practice has a customer service orientation that embraces the importance of meeting patients’ needs, reaffirming that the fundamental basis for health care is “people taking care of people.”72 Whole-person orientation A visible commitment to whole-person care through such mechanisms as developing cooperative alliances with services or organizations that extend beyond the practice setting, but are essential for meeting the complete range of needs for a given patient population.37 The practice has the ability to help guide a patient through the health care system by integrating their care—not simply coordinating it A team approach An understanding that health care is not delivered by an individual, but rather by a system,40 which translates to the development of a multidisciplinary team approach for delivering and continually improving care for an identified population.73 Elimination of barriers to access Elimination, to the extent possible, of barriers to access by patients through implementation of open scheduling, expanded office hours, and additional, convenient options for communication between patients and practice staff Advanced information systems The ability to use an information system to deliver and improve care, to provide effective practice administration, to communicate with patients, to network with other practices, and to monitor the health of the community.74,75 A standardized electronic health record, adapted to the specific needs of family physicians, constitutes the central nervous system of the practice Attractive, convenient, and functional offices Office facilities that are attractive, convenient, and functional in order to meet a variety of patient needs and expectations Focus on quality Ongoing assessment of performance and outcomes and implementation of appropriate changes to enhance quality Equitable reimbursement Payment mechanisms that provide for equitable reimbursement for services from public and private payers Integration of personal care Health assessment (evaluation of health and risk status) Disease prevention (early detection of asymptomatic disease) Health promotion (primary prevention and health behavior/lifestyle modification) Patient education and support for self-care Diagnosis and management of acute injuries and illnesses, with referral as appropriate Diagnosis and management of chronic diseases Coordination and provision of rehabilitative services Supportive care, including end-of-life care Women’s health care Primary mental health care Advocacy for the patient within the health care system Traditional Model of Practice New Model of Practice Care is provided to both genders and all ages; includes all stages of the individual and family life cycles in continuous, healing relationships Care is provided to both genders and all ages; includes all stages of the individual and family life cycles in continuous, healing relationships The doctor is center stage The patient is center stage Unnecessary barriers to access by patients Open access by patients Care is mostly reactive Care is reactive and prospective Care is often fragmented Care is integrated Paper medical record Electronic health record An unpredictable package of services is offered A defined package of services is offered reliably Individual patient oriented Individual and population oriented Communication with practice is synchronous (in person or by telephone) Communication with the practice is both synchronous and asynchronous (e-mail, Web portal, voice mail) Quality of care is assumed Quality of care is continuously measured and improved The physician is the main source of care A multidisciplinary team is the source of care Individual physician-patient visits Individual and group visits involving several patients and members of the health care team Consumes knowledge Consumes and produces knowledge Safety is assumed Systems to insure safety are built in Experience based Evidence based Haphazard chronic disease management Purposeful, organized chronic isease management Struggles financially, undercapitalized Positive financial margin, adequately capitalized
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- "They Go Hand in Hand": Perspectives on the Relationship Between the Core Values of Family Medicine and Abortion Provision Among Family Physicians Who Do Not Oppose Abortion
- "They Go Hand in Hand": Perspectives on the Relationship Between the Core Values of Family Medicine and Abortion Provision Among Family Physicians Who Do Not Oppose Abortion
- Time for Family Medicine to Stop Enabling a Dysfunctional Health Care System
- Priorities for Artificial Intelligence Applications in Primary Care: A Canadian Deliberative Dialogue with Patients, Providers, and Health System Leaders
- Priorities for Artificial Intelligence Applications in Primary Care: A Canadian Deliberative Dialogue with Patients, Providers, and Health System Leaders
- Forces for Integration
- Holding On and Letting Go: A Perspective from the Keystone IV Conference
- Health Is Primary: Family Medicine for America's Health
- A Method for Estimating Relative Complexity of Ambulatory Care
- Implementing the Patient-Centered Medical Home: Observation and Description of the National Demonstration Project
- Methods for Evaluating Practice Change Toward a Patient-Centered Medical Home
- Summary of the National Demonstration Project and Recommendations for the Patient-Centered Medical Home
- Elements of the Patient-Centered Medical Home in Family Practices in Virginia
- Initial Lessons From the First National Demonstration Project on Practice Transformation to a Patient-Centered Medical Home
- Perceived Complexity of Care, Perceived Autonomy, and Career Satisfaction Among Primary Care Physicians
- The nature of informational continuity of care in general practice
- The Medical Home: Growing Evidence to Support a New Approach to Primary Care
- The Medical Home: Locus of Physician Formation
- Annals Journal Club: Novel Staffing for Improved Patient Disease Management
- Family Medicine and the Life Course Paradigm
- In This Issue: Glimpses of a Transformed Model of Care
- Stimulus, Response, Interpretation
- In This Issue: New Model Finances, Systematic Reviews, Patients and Health Care
- Report on Financing the New Model of Family Medicine
- Religion, Spirituality, and the Practice of Medicine