
Abstract
PURPOSE Primary care is the foundation of the health care workforce and the only part that extends life and improves health equity. Previous research on the geographic and specialty distribution of physicians has relied on the American Medical Association’s Masterfile, but these data have limitations that overestimate the workforce.
METHODS We present a pragmatic, systematic, and more accurate method for identifying primary care physicians using the National Plan and Provider Enumeration System (NPPES) and the Virginia All-Payer Claims Database (VA-APCD). Between 2015 and 2019, we identified all Virginia physicians and their specialty through the NPPES. Active physicians were defined by at least 1 claim in the VA-APCD. Specialty was determined hierarchically by the NPPES. Wellness visits were used to identify non–family medicine physicians who were providing primary care.
RESULTS In 2019, there were 20,976 active physicians in Virginia, of whom 5,899 (28.1%) were classified as providing primary care. Of this primary care physician workforce, 52.4% were family medicine physicians; the remaining were internal medicine physicians (18.5%), pediatricians (16.8%), obstetricians and gynecologists (11.8%), and other specialists (0.5%). Over 5 years, the counts and relative percentages of the workforce made up by primary care physicians remained relatively stable.
CONCLUSIONS Our novel method of identifying active physicians with a primary care scope provides a realistic size of the primary care workforce in Virginia, smaller than some previous estimates. Although the method should be expanded to include advanced practice clinicians and to further delineate the scope of practice, this simple approach can be used by policy makers, payers, and planners to ensure adequate primary care capacity.
- workforce
- primary care physicians
- family medicine
- pediatrics
- scope of practice
- professional practice
- delivery of health care
INTRODUCTION
Primary care is foundational to a high-functioning and equitable health system and is the only part of the health care workforce that extends life and improves health equity.1,2 The physician specialties that provide primary care typically include adolescent medicine, family medicine, general practice, geriatric medicine, internal medicine, joint internal medicine and pediatrics, and pediatrics.3 A comprehensive evaluation of the primary care workforce is essential to establish adequate and equitable access to primary care in every community. Additionally, as the population grows and ages, communities should plan for future workforce needs. Finally, to adapt policies that address primary care reimbursement, knowing which physicians provide primary care is essential. By establishing the primary care workforce, it will be possible to further describe the scope, practice setting, and complexity of care provided by primary care physicians. Furthermore, by designating which physicians provide primary care, resources and primary care spending can be more accurately and equitably distributed.
The American Medical Association (AMA) Masterfile has been widely used to describe the physician workforce.1,4,5 Not all researchers have access to the Masterfile, so we propose a method that offers a workforce analysis for those states with claims data and that does not have the limitations of the Masterfile. Although the Division of Health Solutions Data Management makes continuous updates, physician reporting is not mandated and specialty designation or addresses may be outdated or inaccurate.6 Further, the Masterfile is separated into active and inactive physicians, but activity is self-reported by physicians and classified as working more than 20 hours weekly in direct patient care, education, research, administration, or other medical activities. Physicians are not required to update this information annually or at any specific duration over the course of their career. As a result, the Masterfile is suspected to overestimate the rural physician supply by 20%.7
Although the state-specific Virginia primary care workforce has been described previously using the AMA Masterfile, the findings are subject to the above limitations.8 In the past several years, many factors have had an impact on Virginia’s primary care workforce, including Medicaid expansion (effective January 1, 2019) and the COVID-19 pandemic. Approximately 8.5 million people reside in Virginia, and Medicaid expansion increased access to care for more than 500,000 adults. As primary care has led efforts in managing expanded population care and quickly responded to the COVID-19 pandemic,9,10 an accurate estimate of the workforce is necessary to describe the adequacy, distribution, and features of primary care in the state.
In this article, we describe a method for identifying the active workforce that provides primary care in Virginia. Our method leverages the breadth of data available from a state claims database, and bases workforce counts on observed output through claims data rather than relying solely on self-reported outcomes or board certification. We use wellness visits as an adjunctive measure for making primary care designations, reasoning that these visits indicate a unique primary care function beyond any stated specialty.
METHODS
Virginia was chosen as a case example to demonstrate use of several databases to identify the workforce. We used a multistep method to identify all physicians, active status, specialty, and provision of a scope of care that included aspects of primary care, based on publicly available data.
Data Sources
We obtained data from 2 sources: the National Plan and Provider Enumeration System (NPPES) and the Virginia All-Payer Claims Database (VA-APCD). The NPPES database was accessed from the Centers for Medicare and Medicaid Services website (https://download.cms.gov/nppes/NPI_Files.html) in July 2020, and contained physician information (name, mailing address, practice address, etc), specialty taxonomy, and National Provider Identifier (NPI). The VA-APCD databases for 2015-2019 were delivered by Virginia Health Information of the Virginia Department of Health during summer 2020, and contained deidentified information on patient claims, including visit dates, diagnosis and treatment codes, and corresponding NPIs. Up to 80% of all claims in Virginia are recorded in the APCD, making it a reliable source for measuring a clinician’s output or work11; state code §32.1-276.7 mandates that all insurers, including Medicare, Medicaid, TRI-CARE, and private insurers, provide claims data to the APCD.
Identifying Clinician Specialty
We used specialty codes from the NPPES to classify Virginia physicians into 5 categories: family medicine, internal medicine, pediatrics, obstetrics and gynecology, and other specialists, according to National Uniform Claim Committee (NUCC) taxonomies (https://www.nucc.org/index.php/code-sets-mainmenu-41/provider-taxonomy-mainmenu-40/csv-mainmenu-57). The NUCC taxonomy identifies an NPI’s specialty using 3 levels: first is group, the major arrangement of entities by service or occupation; second is classification, a detailed specification of service and occupation within the grouping generally designated by board certification; and third is area of specialization, the area of practice within a classification designated by subspecialty certification (Supplemental Table 1). We filtered NPIs to include only those under the NUCC grouping of Allopathic & Osteopathic Physicians. From there we divided physicians into the 5 categories. We chose family medicine because this is a concrete specialty for primary care. We chose internal medicine, pediatrics, and obstetrics and gynecology because these specialties likely often serve a primary care role as a secondary function. The specialist category served as a catchall for all other classifications, which are not likely to perform any primary care role.
Identifying the Primary Care Workforce
Active Physicians
We next identified active physicians. A physician was identified as active for a particular year during the study period (2015-2019) if his or her NPI was associated with at least 1 claim in the VA-APCD for that year. Additionally, physicians who were not identified in the NPPES but had an active claim in the VA-APCD were added as clinically active but with an uncategorized specialty. We filtered out claims from physicians whose practice location was outside the state of Virginia, thereby restricting our list to only those physicians with a Virginia license on record in the NPPES.
Physicians Acting in a Primary Care Capacity
We identified physicians acting in a primary care capacity in 2 ways: first, we included all active physicians who had an NUCC taxonomy of family medicine (Supplemental Table 2), and second, we included all other active physicians who had at least 10 wellness visit codes from January 1 through December 31, 2019. Supplemental Table 3 provides the Current Procedural Terminology (CPT) and Healthcare Common Procedure Coding System (HCPCS) codes used to identify wellness visits. We arrived at a 10-visit minimal threshold because it largely removed wellness claims entered in error while maximizing the count of physicians who were plausibly providing primary care. We further justified this threshold by considering a histogram of total wellness visits for family medicine and pediatric physicians (Figure 1). The bimodal nature of these histograms suggests that the first mode contains physicians who do not predominantly act in a primary care function, while the second mode and its preceding tail contains physicians providing the bulk of primary care. As this distribution is based on a low count of clinical visits, physicians with even 10% full-time equivalent clinical care should not be inadvertently missed.

Distribution of family medicine physicians and pediatricians by annual number of wellness visits.
Note: Estimated annual total number of wellness visits for each physician. Blue dashed line denotes 10–wellness visit threshold. The bimodal distribution, with large right skew, indicates that most family physicians and pediatricians had more than 200 wellness visits per year, but a small proportion had fewer than 10 per year.
RESULTS
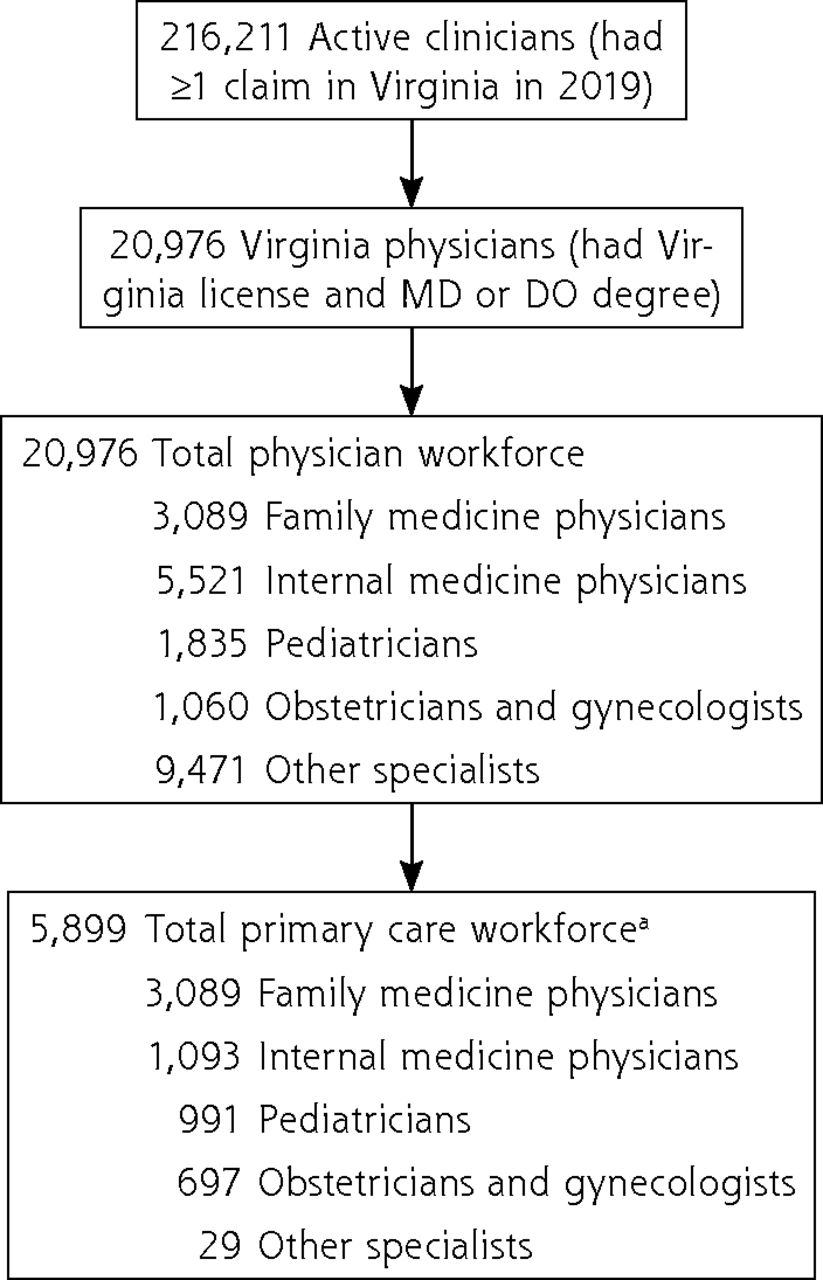
Figure 2 shows the multistep method we used to sequentially identify active physicians, Virginia physicians, physician specialty, and activity in a primary care capacity. In 2019, there were 216,211 physicians who were active as defined by the presence of at least 1 claim in the VA-APCD, which includes physicians providing teleradiology and telehealth services, pathologists, and any physicians from surrounding states who care for Virginians. Of those, 20,976 physicians had both a Virginia license and a doctor of medicine (MD) or doctor of osteopathic medicine (DO) degree. The counts for each specialty are shown in the third row. Among the 20,976 active physicians in Virginia, 5,899 (28.1%) met our definition of primary care physicians, comparable to prior estimates using the AMA Masterfile,12 but three-fourths of the estimate by the Association of American Medical Colleges.13 Family medicine physicians represented 52.4% of these primary care physicians, internal medicine physicians 18.5%, pediatricians 16.8%, obstetricians and gynecologists 11.8%, and other specialists 0.5%.

Multistep method for identifying the active primary care workforce in Virginia, 2019.
DO = doctor of osteopathic medicine; MD = doctor of medicine.
a Primary care designation required either family medicine speciality or another specialty with ≥10 wellness visit codes for the year.
Table 1 provides the total number of active physicians identified in Virginia both overall and by specialty category for each year between 2015 and 2019. Also included are the counts and percentages of these totals classified here as part of the primary care workforce. The total number of active physicians in Virginia remained steady throughout 2015-2019, with the overall number of physicians increasing by 3.5% during that time. Over those 5 years, 60.45% of all physicians and 60.87% of primary care physicians remained active. Merely 11.66% of all physicians had a claim in only 1 year. The number of active family medicine physicians increased by 5%, internal medicine physicians by 5%, pediatricians by 0%, obstetricians and gynecologists by less than 1%, and specialists by 3%. During the study period, the population of Virginia grew 1% from 8.41 million to 8.50 million, and the percent of people with new insurance due to Medicaid expansion was 5.4%. Finally, some physicians met the 10–wellness visit threshold in a given year but not in the next; for the primary care specialties, this value ranged from 9.13% to 19.87% of physicians (Supplemental Table 4).
Virginia’s Active Physician Workforce, Total and Primary Care, 2015-2019
Figure 3 is a Venn diagram of the groupings used to define our Virginia primary care workforce in 2019, based on all active clinicians for that year. This diagram, a workforce conceptual model, shows that there are clinicians outside our definition who could be performing a primary care function in the state. These clinicians could be clinicians who do not have a Virginia license reported in NPPES, who do not have an MD or DO degree, or both. The diagram also shows how small a footprint primary care has among all entities filing claims. In 2019, nearly 20% of internists, 54% of pediatricians, and 66% of obstetricians and gynecologists were classified as providing primary care; less than 1% of specialists were so classified. Between 2015 and 2019, the percentage of active physicians classified as providing primary care remained about 28% to 29%.

Venn diagram for identifying the 5,899 members of Virginia’s active primary care workforce in 2019.
DO = doctor of osteopathic medicine; MD = doctor of medicine; VA-APCD = Virginia All-Payer Claims Database.
Notes: Diagram based on all active clinicians in Virginia in 2019 (as determined from ≥1 claim in VA-APCD database). Top left (blue) includes 25,332 clinicians who held a Virginia license. Top right (orange) includes 147,577 physicians who had an MD or DO degree. Bottom center (gray) includes 366 clinicians likely serving in a primary care capacity as ascertained from wellness visit claims, but who did not hold a Virginia license and did not have an MD or DO degree.
DISCUSSION
We describe a novel method for identifying the primary care workforce and physicians serving a primary care function in Virginia. The use of these databases and identifiers including active status, matching for NPI, and identifying wellness visits for non–primary care specialties is a first step toward a comprehensive approach to identify the types of primary care physicians in a state. This analysis identified 3,089 family physicians, 1,093 internists, and 991 primary care pediatricians in Virginia as physicians providing primary care, values lower than prior estimates.14,15 Additionally, 65.7% of obstetricians and gynecologists provided primary care as defined by wellness visits, which appears valid given the frequency at which these physicians provide well-woman examinations.
Our method uses wellness examinations as one indicator of primary care. We considered other possible indicators, such as vaccines, injections, or number of diagnoses per visit. It is likely, however, that none of these are specific to primary care. For example, pneumococcal vaccines are often provided by pulmonologists and joint injections by orthopedists, and numerous specialists code more than 4 or 5 diagnoses per visit with a patient. As such, wellness visits appeared to be the most robust indicator for identifying primary care activity. We did not apply this metric to family medicine self-designated physicians. If we had applied this criterion, only 1,793 family physicians would be considered primary care physicians, an additional 22.0% reduction in Virginia’s primary care workforce. Although some family physicians do practice in urgent care clinics, emergency departments, or specialty settings (eg, orthopedic or dermatology practices), we suspect most, even without 10 wellness examinations annually, are functioning as primary care physicians. Ongoing work to determine primary care status based on practice setting will help to remove non–primary care family physicians and increase the number of internal medicine, pediatric, obstetric and gynecologic, and specialist physicians included in our primary care workforce measure.
Prior workforce analysis excluded specialists in the identification of physicians who provide primary care.8,14,16 In Virginia, some primary care, specifically in remote and rural regions of the state, is likely provided by specialist physicians acting as both specialists and primary care physicians. Applying this inclusion criterion, we find that only a small number of specialists, 29 to 41, were functioning in this capacity.
The method we describe has some limitations. Wellness visits, although a major part of primary care, may not be fully emblematic of the broad scope of primary care functionality. In the future, it may be possible to evaluate a cohesive set of measures that more specifically indicates a primary care function. Additionally, Virginia has a large number of active-duty military personnel (~128,000) and people receiving care from the Veterans Health Administration (~736,000). Our analysis does not include care received on military installations or at the Veterans Administration, as claims for that care are not currently captured in the VA-APCD. Similarly, uninsured care and direct primary care are not captured in the VA-APCD because of lacking claims with any payer. The NPPES data are routinely updated to capture changes in the national medical workforce indicating the possibility of a lag in providing updated physician information; therefore, a limitation to our decision to count physicians with a Virginia license is that some Virginia physicians may be missed because their information in the NPPES has not been updated to show that they have this license. For example, this is often the case for new physicians transitioning out of residency. Despite this limitation, we believe our measure of the primary care workforce is more representative of the active workforce because continuity in practice is a key attribute of primary care. A stable workforce between 2015 and 2019 supports this assumption. Finally, as described, we overestimated the number of family physicians and underestimated the number of other specialists practicing primary care. Future work will correct this situation by considering additional scope of practice characteristics and more importantly, practice setting, although these approaches are harder to replicate as they require more manual efforts.
The foundation of this workforce data offers great potential for further analysis. Using claims, the scope of care provided by primary care physicians can be more definitively described. Additionally, these data enable exploration of the Starfield concepts of comprehensiveness, coordination, and continuity of care.17 The longitudinal and patient-specific data provided in the APCD will allow for further research into the longitudinal primary care physician-patient relationship. As we work to better build our primary care health care delivery system and we shift payments to value-based models, the distribution and efficacy of primary care will need to be continually explored. Our analysis provides a first step into a more thorough understanding of primary care in Virginia and will act as the foundation for further research in workforce, scope, and value in medicine.
Footnotes
Conflicts of interest: authors report none.
Funding support: Funding for this study was provided by the Department of Medical Assistance Services and the National Center for Advancing Translational Sciences (UL1TR002649).
- Received for publication September 30, 2021.
- Revision received February 24, 2022.
- Accepted for publication May 11, 2022.
- © 2022 Annals of Family Medicine, Inc.




{kind=link}
{kind=link}
{kind=link}