
Abstract
We conducted 2 analyses using administrative data to understand whether more family physicians in Ontario, Canada stopped working during the COVID-19 pandemic compared with previous years. First, we found 3.1% of physicians working in 2019 (n = 385/12,247) reported no billings in the first 6 months of the pandemic; compared with other family physicians, a higher portion were aged 75 years or older (13.0% vs 3.4%, P <0.001), had fee-for-service reimbursement (37.7% vs 24.9%, P <0.001), and had a panel size under 500 patients (40.0% vs 25.8%, P <0.001). Second, a fitted regression line found the absolute increase in the percentage of family physicians stopping work was 0.03% per year from 2010 to 2019 (P = 0.042) but 1.2% between 2019 to 2020 (P <0.001). More research is needed to understand the impact of physicians stopping work on primary care attachment and access to care.
INTRODUCTION
The COVID-19 pandemic disrupted how care was delivered by family physicians. To limit transmission, practices adopted a range of measures including active and passive screening, cleaning, strict use of personal protective equipment, and reducing the number of staff and patients in the office. In the first few weeks of the pandemic, nonessential care was deferred1 and total visits to primary care decreased by nearly 30%.2 At the same time, there was a dramatic shift to virtual care2 and primary care physicians were tasked with other system roles.3
These changes placed extraordinary stress on family physicians, particularly in Canada and the United States, where many operate as small business owners and rely on fee-for-service billings for revenue.4 Surveys of family physicians during the first wave of the pandemic detail numerous challenges including reduced revenue, retention of office staff, and difficulty obtaining personal protective equipment; many physicians also worried about their own personal safety.5,6 These challenges may have led some family physicians to prematurely stop working7–9 but more research is needed in different settings.
In Ontario, physicians are primarily paid through the provincial health insurance plan which provides coverage to all provincial residents for physician visits. Roughly 80% of family physicians work in a patient enrollment model where they formally enroll patients and between 15% and 70% of payment is based on age-sex adjusted capitation.10,11 The remaining 20% largely operate independent, fee-for-service practices with many working in walk-in clinics or doing focused practice.12 We sought to understand the number and characteristics of physicians stopping work in the first 6 months of the pandemic in Ontario, Canada.
METHODS
We conducted 2 analyses using routinely collected data including billing claims. Data sets only included de-identified data that were linked using unique encrypted identifiers and analyzed at ICES. ICES is an independent, nonprofit research institute whose legal status under Ontario’s health information privacy law allows it to collect and analyze health care and demographic data, without consent, for health system evaluation and improvement. Patients were attributed to physicians based on enrollment data; patients who were not enrolled were attributed to a physician using virtual rostering according to the highest billings for that patient.
First, we calculated the ratio of total visits (office, virtual, and home) from March 11, 2020 to September 29, 2020 to total visits in the same period in 2019 for each family physician who had at least 50 billing days in 2019; we assessed variation in the ratio within and across physician groups. We identified physicians who had 0 visits from March 11, 2020 to September 29, 2020 and compared their characteristics to those who had any visits during that time period using a t-test for mean and χ2 test for categorical variables.
Second, we conducted a repeated cross-sectional analysis. For each year from 2010 to 2020, we examined the cohort of physicians practicing in the first quarter of the year and noted the number and percent who stopped practicing (ie, had no billings) between April 1 and September 30. We fit a linear regression line to the number of physicians per 1,000 who stopped practicing in each year from 2010 to 2019 and used this to predict the expected 2020 outcome; we compared this to the observed 2020 outcome. Analysis was done in SAS Enterprise Guide (SAS Institute Inc) and graphs were produced in R v4.0.5 (the R Foundation).
RESULTS
We analyzed data for 12,247 family physicians practicing in Ontario in 2019 (Table 1). During the week of September 29, 2019 there were 916,831 total visits in 2019, of which 97% were in-office, compared with 903,402 total visits in 2020, of which 40% were in-office (Supplemental Figure 1). Most family physicians had 0 to 50% fewer total visits post-pandemic compared with the same period in 2019 (Supplemental Figure 2) but there was considerable variation both between and within groups (Supplemental Figure 3).
Characteristics of All Family Physicians in Ontario, Canada Active in 2019 and Comparison of Characteristics Between Those With No Outpatient Visits During the First 6 Months of the COVID-19 Pandemic (March-September 2020) and Those With Any Visits
There were 3.1% (n = 385) of physicians practicing in 2019 who had no primary care visits during the first 6 months of the pandemic (Table 1). Compared with other family physicians, a higher portion of physicians with no primary care visits were aged 75 years or older (13.0% vs 3.4%, P <0.001), practicing fee-for-service (37.7% vs 24.9%, P <0.001), had a panel size under 500 patients (40.0% vs 25.8%, P <0.001), had fewer billing days in 2019 (mean 73 vs 101, P <0.001), and had fewer total visits in 2019 (1,266 vs 2,087, P <0.001). Fifty-six percent (n = 215) of those who stopped working practiced in a patient enrollment model (PEM). The percentage of all family physicians who stopped work ranged from 0% to 14% in a given subregion with higher percentages in both urban and rural areas (Supplemental Figure 4).
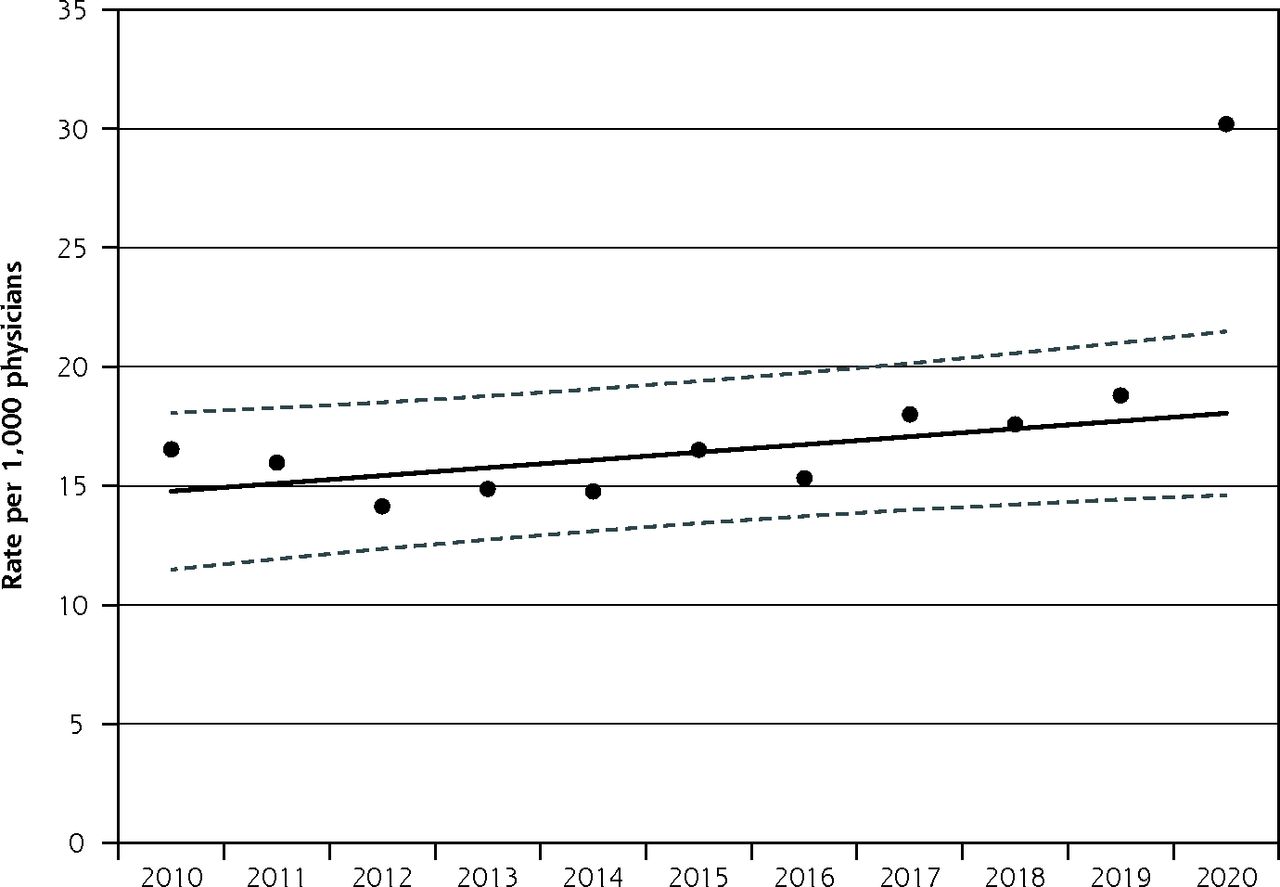
In each year between 2010 and 2019, an average of 1.6% of family physicians who were working from January to March stopped work between April and September; in contrast, 3.0% stopped work in 2020 (Supplemental Figure 5). Figure 1 depicts the observed and fitted data. The fitted regression line estimated 1.48% of family physicians stopped working in 2010. The absolute increase in the percentage of family physicians stopping work was 0.03% per year from 2010 to 2019 (P = 0.042) but 1.2% between 2019 to 2020 (P <0.001).

Number of family physicians per 1,000 who were actively practicing from January to March in a given year but who had 0 primary care visits between April and September of that year, 2010-2020. Observed numbers and fitted regression line with 95% CIs.
DISCUSSION
We found that roughly 3% of the 12,000 practicing family physicians in Ontario, Canada stopped working during the first 6 months of the pandemic—approximately twice as many as in previous years. Our estimate of the proportion stopping work was consistent using 2 different analytic methods. Physicians stopping work were more likely to be aged 75 years or over, practice fee-for-service, have a panel size under 500, and work less than other physicians in the previous year—factors that are likely correlated and consistent with physicians heading into retirement.
Although the absolute number of physicians stopping work was small, the impact on patients and communities is likely substantial. Just over one-half of the physicians who stopped working were practicing in a patient enrollment model and responsible for care of formally rostered patients. Using the mean panel size of 788, we can estimate these physicians cared for approximately 170,000 patients who may now be unattached. The number of unattached is likely even higher as some physicians who practiced outside a patient enrollment model and who stopped working were also providing comprehensive primary care. These health human resource challenges are occurring in a province where approximately 10% of the population does not have a family physician.13,14
Although we cannot directly attribute causation, we hypothesize that some family physicians accelerated their retirement plans because of the pandemic. Possible reasons include the concerns about health, increased practice costs due to recommended infection prevention and control measures, drop in revenue due to the reduction in total visits,15,16 and burnout.17,18 More research is needed to understand the long-standing impact on primary care attachment and access to care and the broader impact on population health.
Acknowledgments
Thank you to Peter Gozdyra for creating the map of percentage of physicians stopping work by subregion.
Footnotes
Conflicts of interest: authors report none.
Author contributions: T.K. and R.H.G. conceived of the study. All authors helped design the study. F.C.W., A.K., and L.L. conducted the analysis. All authors helped interpret the data. T.K. drafted the manuscript and all authors critically reviewed it. All authors read and approved the final manuscript.
Funding support: This study was supported by ICES, which is funded by an annual grant from the Ontario Ministry of Health (MOH) and the Ministry of Long-Term Care (MLTC). This study also received funding from the Canadian Institutes of Health Research funding reference number SOP 162662 and also received some support from the INSPIRE Primary Health Care Research Program which is funded through the Health Systems Research Program of the Ontario Ministry of Health and Long-Term Care. Parts of this material are based on data and information compiled and provided by Ontario Ministry of Health (MOH). The analyses, conclusions, opinions, and statements expressed herein are solely those of the authors and do not reflect those of the funding or data sources; no endorsement is intended or should be inferred.
T.K. and R.H.G. are supported as Clinician Scientists by the Department of Family and Community Medicine at the University of Toronto and at St Michael’s Hospital. T.K. is the Fidani Chair of Improvement and Innovation in Family Medicine at the University of Toronto. M.E.G. is supported by the Brian Hennen Chair in Family Medicine at Queen’s University.
- Received for publication August 31, 2021.
- Revision received March 12, 2022.
- Accepted for publication May 4, 2022.
- © 2022 Annals of Family Medicine, Inc.
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- Primary care in the COVID-19 pandemic and beyond: Lessons from Ontario
- Characteristics of walk-in clinic physicians and patients in Ontario: Cross-sectional study
- Characteristics of family physicians with additional training or focused practices in caring for older adults: Population-based retrospective cohort study
- Public experiences and perspectives of primary care in Canada: results from a cross-sectional survey
- Describing primary care patterns before and during the COVID-19 pandemic across Canada: a quasi-experimental pre-post design cohort study using national practice-based research network data
- Characteristics of primary care practices by proportion of patients unvaccinated against SARS-CoV-2: a cross-sectional cohort study
- Soins primaires pour tous: Le Canada peut sinspirer de pays semblables ayant un niveau eleve de continuite relationnelle entre patientele et centres de soins primaires
- Characteristics of Walk-In Clinic Physicians and Patients in Ontario, Canada: A Cross-Sectional Study
- Characteristics of patients attached to near-retirement family physicians: a population-based serial cross-sectional study in Ontario, Canada
- Primary care for all: lessons for Canada from peer countries with high primary care attachment
- Trends in attachment to a primary care provider in Ontario, 2008-2018: an interrupted time-series analysis
- Should family medicine residents in Canada do a third year of training?
- Factors influencing practice choices of early-career family physicians in Canada: A qualitative interview study
- Trends in patient attachment to an aging primary care workforce: a population-based serial cross-sectional study in Ontario, Canada
- Evaluation of the implementation of single points of access for unattached patients in primary care and their effects: a study protocol
- Garder la porte dentree ouverte : assurer lacces aux soins primaires a toute la population canadienne
- Keeping the front door open: ensuring access to primary care for all in Canada
- Health care crisis in Canada: What is the matter?
- Family medicines stress test
- Family physician practice patterns during COVID-19 and future intentions: Cross-sectional survey in Ontario, Canada