
Abstract
PURPOSE Most patients are escorted to exam rooms (escorted rooming) although patients directing themselves to their exam room (self-rooming) saves patient and staff time while increasing patient satisfaction. This study assesses patient and staff perceptions after pragmatic implementation of self-rooming.
METHODS In October-December 2020, we surveyed patients and staff in 25 primary care clinics after our institution expanded self-rooming from 4 specially built clinics during the COVID-19 pandemic. Semi-structured surveys asked about rooming process used, rooming process preferred, and perceptions of self-rooming compared with escorted rooming.
RESULTS Most patients (n = 1,561) preferred self-rooming (86%), especially among patients aged <65 years and in family medicine clinics. Few patients felt less welcomed (10.6%), less cared about (6.8%), more isolated (15.6%), more lost/confused (7.6%), or more frustrated (3.2%) with self-rooming compared with escorted rooming. Early-adopter clinics that implemented self-rooming ≤2016 had even lower rates of patients feeling more isolated, lost/confused, or frustrated with self-rooming compared with escorted rooming.
Over one-half of staff (n = 241; 180 clinical, 61 nonclinical) preferred self-rooming (59%) and thought most patients liked self-rooming (65.8%), especially among clinical staff and in early adopter clinics (≤2016). Few staff reported worse waiting times for patients (12.4%), medical assistants (MAs) (15.9%), and clinicians (16.4%) or worse crowding in waiting areas (1.7%) and hallways (10.1%). Unlike patient-reported confusion (7.6%), most staff thought self-rooming led to more patient confusion (63.8%), except in early-adopter clinics (44.4%).
CONCLUSIONS Self-rooming is a patient-centered innovation that is also acceptable to staff. We demonstrated that pragmatic implementation is feasible across primary care without expensive technology or specially designed buildings.
INTRODUCTION
Self-rooming is a relatively new process where patients direct themselves to an assigned exam room immediately after checking in, bypassing the traditional experience in which a staff member would escort them from a waiting room to their exam room. Self-rooming decreases waiting time for patients and decreases staff time and cost, while increasing patient satisfaction, as we previously reported.1 However, leaders of traditionally designed clinics are often reluctant to redesign the rooming experience, believing their buildings need specific features like hallways with few intersections, and dual-access rooms.2 Previous studies have demonstrated that self-rooming can increase efficiency, cost effectiveness, and patient satisfaction, but emphasize the need for modified or additional technology3 and specially designed buildings.1,4,5 Health systems did not routinely consider potential benefits and missed opportunities of widespread self-rooming practices until the presence of patients in a traditional waiting room became an intolerable risk due to the COVID-19 pandemic.
Health systems responded to the threat of COVID-19 spread by rapidly implementing self-rooming with existing clinic layouts to promote physical distancing and avoid viral exposure in waiting rooms. Our health system, UW Health, is a public academic institution in Madison, Wisconsin. We successfully piloted self-rooming in 2 clinics in 2008-2009, which informed the design of 4 clinics in 2015-2016 specifically designed and built to improve team-based care and patient flow.1,4,5 Faced with the need to limit COVID-19 spread, our health system quickly overcame concerns about uninviting or confusing building infrastructure, patients getting lost, or unescorted patients compromising privacy. The rooming process was rapidly redesigned to implement self-rooming in the majority of our primary care clinics without the need for investments in technology or building construction.
The objective of this study was to determine whether self-rooming is an acceptable alternative to escorted rooming based on the perceptions of patients and staff in 25 primary care clinics that implemented self-rooming. We surveyed patients and staff rooming process preferences and perceptions. Based on our initial experience and survey results, concerns that self-rooming would be unworkable in most primary care clinic settings were unfounded. Ultimately our health system decided that self-rooming will be a permanent feature and it has been implemented across the remaining primary care clinics in the health system.
METHODS
Setting
UW Health is a public academic institution in Madison, Wisconsin that served >314,000 patients through a largely capitated system at 29 academic and community primary care clinics during the study period (October-December 2020). In over one-half of the clinics, at least 20% of the patient population was uninsured, on Medicaid, on Medicare, and/or was non-White in race/ethnicity. Of these clinics, 5 were in rural communities and 1 was a federally qualified health center. UW Health and the University of Wisconsin Primary Care Academics Transforming Healthcare (PATH) group is supporting rapid transformation of primary care related to COVID-19. UW Health has committed to be a learning health system through the process of learning from our own experience and regular evaluation of outcomes.6
Design
Early in the pandemic, our primary care system reduced numbers of patients seen in ambulatory clinics to limit the spread of COVID-19. By May 2020, we were slowly increasing necessary face-to-face office visits but needed to continue physical distancing. A workgroup was formed from 4 primary care clinics that use self-rooming in buildings designed for that purpose.1,4,5 Our workgroup was tasked to promote and formalize self-rooming in all 29 of our primary care clinics, each with a different structural layout not intentionally designed to make self-rooming possible. The workgroup designed a self-rooming workflow that does not require new technology or building construction, with the following components: (1) workflow for patient scheduling representatives when patients arrive to the clinic; (2) workflow for medical assistants (MAs) when patients arrive to their exam room; (3) workflow for clinicians when patients are ready; (4) retrofitting the layout of clinics to support wayfinding for patients.
Intervention and Implementation
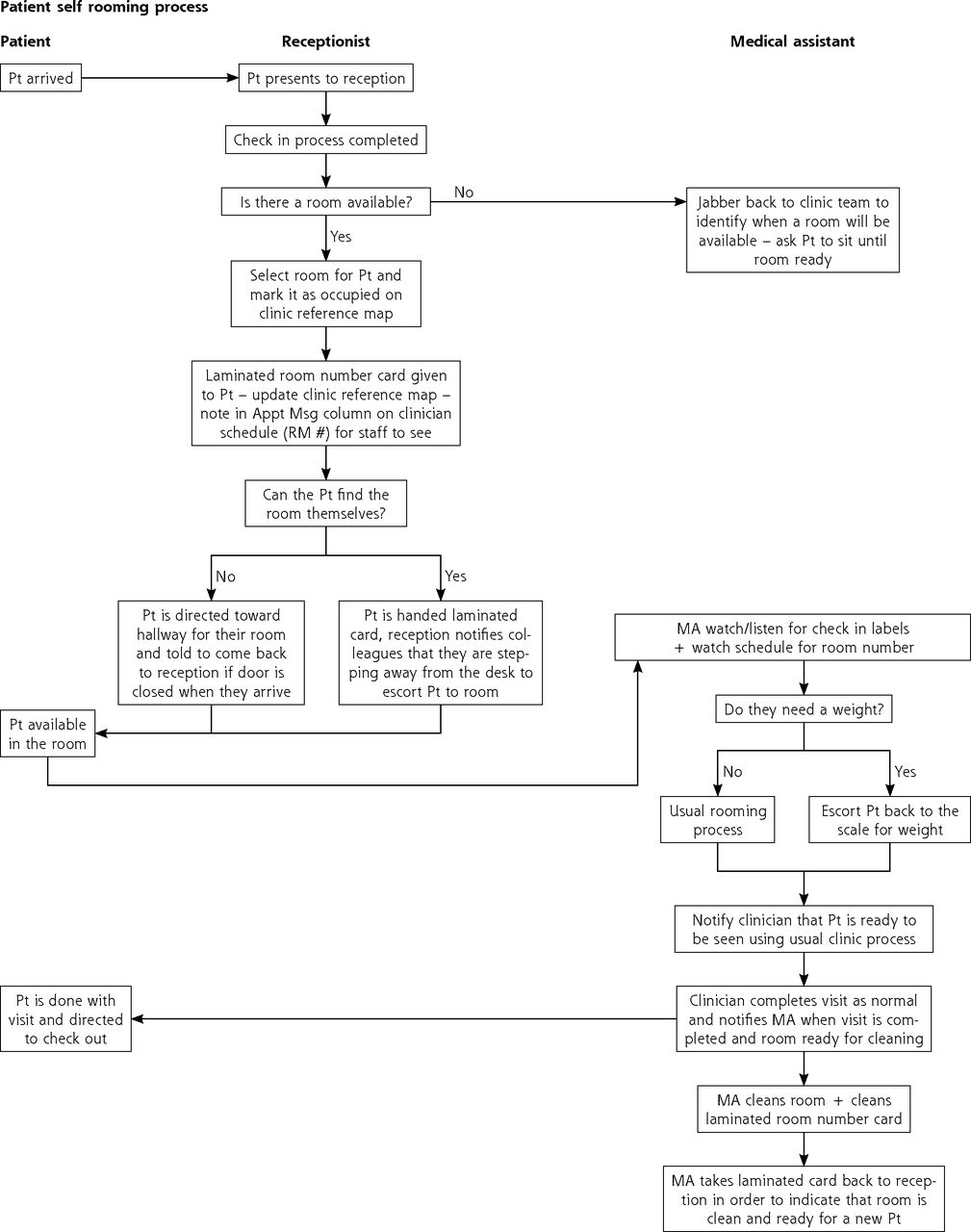
Figure 1 shows our self-rooming workflow. Patient scheduling representatives (PSRs) give patients laminated cards with directions to their exam room and patients go directly there. Exceptions include patients waiting when no rooms are available or being escorted by PSRs if unable to find their room. Patient scheduling representatives inform MAs electronically through the schedule or secure messaging. Medical assistants complete usual processes directly in exam rooms, clean rooms after clinician visits, and take laminated cards back to reception. This self-rooming plan was implemented in all family medicine clinics and all but 2 general internal medicine clinics by May 30, 2020. It has now been implemented across all primary care clinics including pediatrics and will be a permanent change for our institution. Our detailed workflow (both check-in and check-out) and supplemental materials including surveys are available on HIPxChange (www.hipxchange.org/SelfRooming).
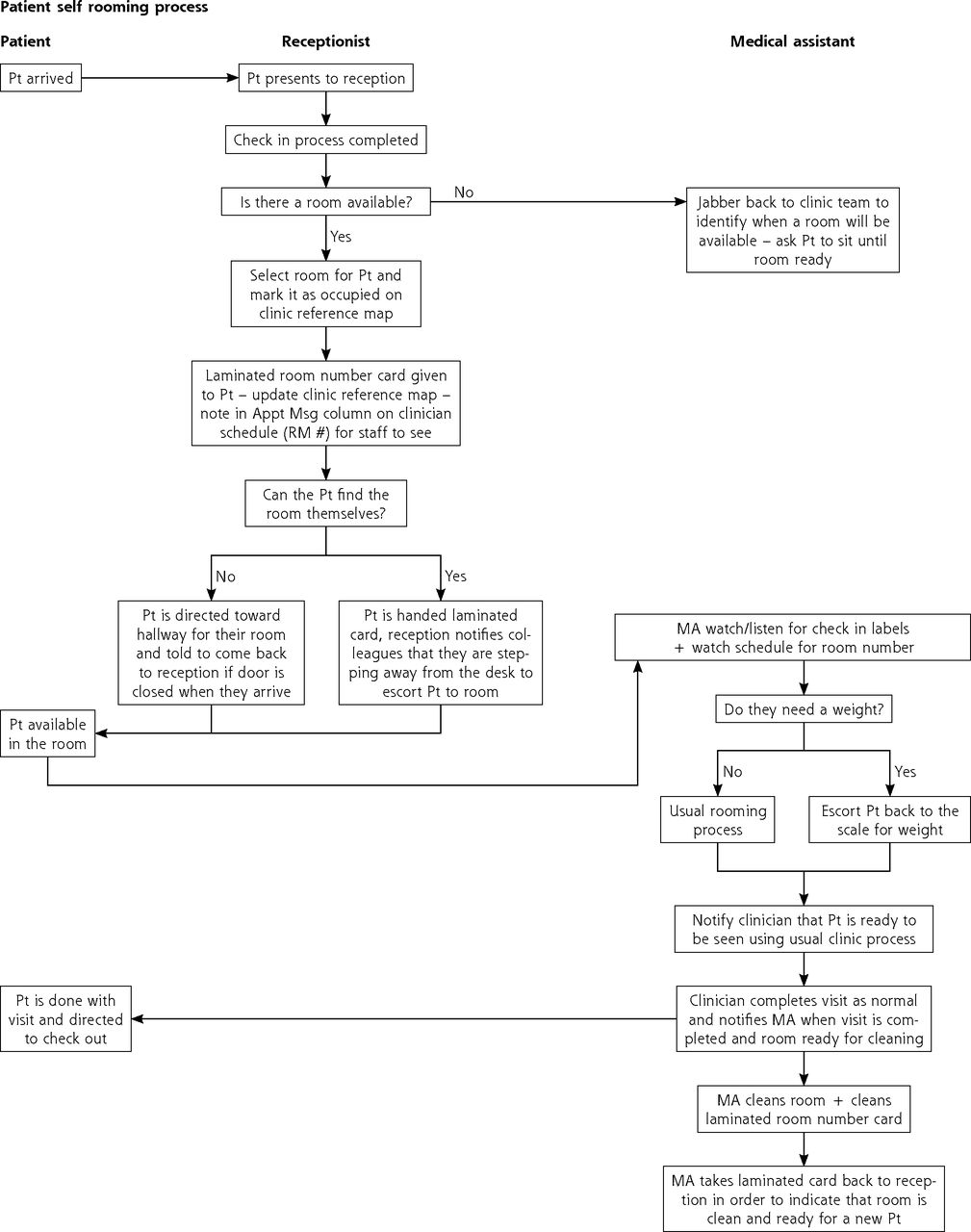
Process map of the self-rooming workflow.
Jabber = electronic messaging software used to facilitate communication among team members; MA = medical assistant; Pt = patient; receptionist = patient scheduling representative; RM = room
Data Collection
We developed semistructured surveys to assess patient and staff preferences and perceptions between self-rooming and escorted rooming during the study period October-December 2020, in the 25 clinics that had implemented self-rooming.
The patient survey was self-administered by consecutive patients between visit check-in and check-out after each clinic received 100 paper copies of the survey. The survey asked (1) whether the patient was escorted, self-roomed, or other; (2) whether they preferred escorted rooming, self-rooming, or other; and (3) how welcomed, isolated, lost or confused, cared about, and frustrated they felt with self-rooming compared with escorted rooming (much less, somewhat less, neither, somewhat more, much more).
Staff surveys were self-administered online. Clinical staff (MAs and clinicians) and nonclinical staff (PSRs) were asked (1) whether they preferred escorted rooming, self-rooming, or other, and (2) how self-rooming compared with escorted rooming on waiting times, crowding, and patient confusion (much worse, somewhat worse, neither, somewhat better, and much better).
Surveys prompted open-ended comments and basic respondent demographics. The institutional review board (IRB) exempted this study as an improvement program evaluation with permission to publish.
Data Analysis
We calculated descriptive statistics and significance tests using the C2 test of independence—or Fischer’s exact test when cells were <5—in the statistical software SPSS Version 26.0 (IBM Corp). The “prefer self-rooming” variable was coded 1 for the response “Receive a card with the room number and proceed directly to the exam room (self-rooming).” To inform primary care redesign by determining whether self-rooming was an acceptable (not worse) alternative to escorted rooming, we dichotomized the remaining variables as follows.7 For patient responses, we coded the positive variables (welcomed, cared about) as worse (“much less” or “somewhat less”) vs not worse (“neither”, “somewhat more”, or “much more”) and the negative variables (isolated, lost/confused, frustrated) as worse (“much more” or “somewhat more”) vs not worse (“neither”, “somewhat less”, or “much less”). Similarly, we coded staff responses as worse (“much worse” or “somewhat worse”) vs not worse (“neither”, “somewhat better”, and “much better”). We also examined open-ended survey responses for key themes related to patient and staff concerns and suggestions.
RESULTS
Patient response rates across clinics (median = 79%, interquartile range = 38% to 100%) did not vary systematically with patient demographics. Patient respondents (n = 1,561) were mostly female, average age 52.4 (Table 1). Of the respondents, 1,336 patients self-roomed, 80 were escorted, and 99 described elements of self-rooming (eg, told which room to go to but not given a card).
Characteristics of Patients and Staff Responding to the Rooming Questionnaire
On the preferred rooming process question, 86.4% of patients selected self-rooming (Table 2), 7.2% escorted rooming, and 6.4% “other,” describing in comments elements of self-rooming or no preference. Preferring self-rooming was significantly higher among patients aged <65 years and in family medicine clinics. Few patients reported feeling less welcomed (10.6%), less cared about (6.8%), more isolated (15.6%), more lost/confused (7.6%), or more frustrated (3.2%) with self-rooming. Early adopter clinics that implemented self-rooming ≤2016 had even lower rates of patients feeling more isolated, lost/confused, or frustrated with self-rooming.
Patient Perceptions of Self-Rooming Compared With Escorted Rooming
Staff surveys were completed by most staff (n = 241; 180 clinical, 161 nonclinical), who are mostly clinical staff with ≥5 years of experience (Table 1). Table 3 shows over one-half of staff preferred self-rooming (59.3%) and reported most patients like self-rooming (65.8%). These proportions were significantly higher among clinical staff and in early adopter clinics (≤2016). Clinical staff respondents were additionally asked about waiting times, crowding, and patient confusion. Few reported longer waiting times for patients (12.4%), MAs (15.9%), and clinicians (16.4%) or more crowding in waiting areas (1.7%) and hallways (10.1%). However, in contrast with patient-reported perceptions, most staff thought self-rooming led to more patient confusion (63.8%) though this was significantly lower (44.4%) in early adopter clinics.
Staff Perceptions of Self-Rooming Compared With Escorted Rooming
Most open-ended survey responses reported positive perceptions of self-rooming. Some comments described remaining concerns and respondents provided suggestions for self-rooming implementation to mitigate these concerns (Table 4).
Patient and Staff Concerns and Suggestions for Self-Rooming Implementation
DISCUSSION
Our institution successfully implemented self-rooming across primary care during the COVID-19 pandemic with no capital investments in new technological or building infrastructure. This large post-implementation survey of patients (n = 1,561) and staff (n = 241) in 27 clinics showed that most patients and a smaller majority of staff selected self-rooming as their preferred process. Furthermore, only few respondents thought self-rooming was worse than escorted rooming in terms of patient friendliness, waiting times, and crowding. Self-rooming was perceived even better in pre-pandemic early adopter clinics (≤2016) and among patients aged <65 years and clinical staff. One notable exception was that most staff believed that patient confusion would be worse with self-rooming than with escorted rooming, a belief that was not consistent with actual patient-reported perceptions.
This study demonstrated that implementing self-rooming does not require new infrastructure and significant capital investment as previously believed. Redesigning workflows within existing infrastructure achieved accelerated and low-cost implementation of self-rooming across all primary care clinics during the pandemic. Building on our previous pilot estimating clinic cost-savings of 6 staff hours monthly translating to $1,500 annually,1 our self-rooming implementation in 25 clinics yields estimated cost savings of 150 staff hours monthly translating to $37,500 annually. With the ongoing staff turnover and retention challenges in health care, self-rooming could be part of a solution. The benefits of self-rooming reported by patients and staff in this study are consistent with benefits shown by previous studies focused on implementing self-rooming through mobile technology3 or in clinics with intuitive layouts.1,3 Specifically designed infrastructure for self-rooming was previously seen as a requirement and its absence as an impediment. With the pandemic, those concerns were set aside and our study shows them to be unfounded. This study demonstrated that even without investments in mobile communication technology or building redesigns, self-rooming is acceptable to patients and staff. In line with human factors engineering models of work systems design,8-11 this finding suggests that our redesigned workflow is well aligned with the user needs of patient and staff, with task and organizational features adequately balancing out the absences of dedicated technology and building infrastructure.
Most patients selected self-rooming as their preferred rooming process and few felt it was less patient friendly than escorted rooming. We found that patients often feel at least as welcome and cared about when able to immediately go to their own exam room rather than waiting in a designated waiting area. The time alone in the exam room also appears to provide patients the opportunity to mentally prepare for the visit without distractions. This is consistent with research suggesting that the emotions and behaviors of other patients in the waiting room may increase a patient’s stress before the visit.12,13 Our findings suggest that with some exceptions to be investigated in future work as described below, most patients are able and willing to find their own exam room and that this may honor their sense of autonomy. Our study therefore demonstrates that there may have previously been missed opportunities for widespread adoption of self-rooming, beyond the obvious safety advantages of not grouping patients in the same space to avoid contagion during and beyond a pandemic.14
Our study shows that staff concern about patient confusion with self-rooming was unfounded. Most staff believed it would be more confusing for patients to be asked to room themselves; in contrast, few patients actually felt more confused with self-rooming. This kind of misalignment between staff perception of patient experience and the reported experience of patients has been found in previous studies15-17 and adds more specific details to our previous report about patient satisfaction with self-rooming.1 Possible explanations for the disconnect include the general uncertainty associated with the pandemic, a natural resistance to change, the inertia of a longstanding process, and staff’s overestimation of their role in patient experience and underestimation of patients’ abilities. It is reassuring that the misalignment of perception between staff and patients about the patient experience appears to diminish over time. In fact, in clinics that had implemented self-rooming ≤2016, staff perceptions that self-rooming leads to more patient confusion than escorted rooming are significantly higher than in clinics that implemented it recently. The same trend is observed with staff perceptions that most patients like self-rooming, which mirror patient perceptions in clinics that have had self-rooming for a few years. The low proportion of patient confusion was also not significantly different for patients aged >65 years, who, despite being somewhat less likely to prefer self-rooming (82% vs 88%), were not significantly more likely to feel confused, lost, isolated, or frustrated with self-rooming. This suggests that self-rooming is acceptable even for some patients whom staff may perceive as more vulnerable. Some comments from patients and staff did suggest that certain patients with a physical or cognitive impairment may prefer escorted rooming. Suggested approaches for managing negative staff expectations include education and awareness about positive patient preferences and perceptions, future reassessment of self-rooming after a period of adjustment, and engaging staff and patients in informing future refinements to the self-rooming process. Refinements may include reviewing how patient-reported information may be collected from patients if they are no longer in a waiting room, such as via patient portals or telephone calls.
Strengths and Limitations
This is the first health system–level study of self-rooming. It addresses a primary care redesign need that recently became more salient and will likely endure post pandemic given ongoing staff shortages. Study strengths include its evaluation of a quality improvement strategy in a real-world setting and its reliance on a successful pilot to roll out a full-scale implementation. Large patient and staff survey sample sizes help substantiate findings that self-rooming is a patient-friendly innovation that is strongly preferred by patients and acceptable to staff, complementing previous evidence of cost savings.
The study has several limitations. First, although this study included almost all primary care clinics in our system, it does not account for the potentially different characteristics of other systems and their patient populations and workforces. Second, the surveys were in English and self-administered, possibly excluding persons with limited English proficiency or low literacy. Third, we dichotomized responses on the 5-point survey items to address small cells, leading to loss of granularity and richness of data. Fourth, staff surveys differentiated between clinical and nonclinical staff but not among clinical staff (clinicians vs MAs). Nonclinical staff surveys also lacked the detailed questions asked of the clinical staff. Fifth, this study was conducted during a pandemic, when it can be expected that most aspects of care would be prioritized lower compared with personal safety. Generalizability to a post-pandemic normal cannot be assumed without repeating the study. Finally, this study focused on short-term perceptions of gains or risks. The study did not consider potential impacts on long-term relationship building by reducing opportunities for patient interaction while walking to the exam room. Similarly, the study did not examine long-term risks or gains for specific populations.
Future Directions
There are several future directions for additional study. First, repeating the surveys post pandemic would address the bias toward personal safety. Second, self-rooming in pediatrics needs study. Third, future surveys need to better distinguish different staff roles and to ask all respondents if they prefer returning to escorted rooming. Fourth, qualitative in-person interviews can explain and expand on the study’s findings. Finally, longer-term impact studies can evaluate which rooming type better affords time and opportunity for focused relationship building. Longer-term impacts studies may also examine specific populations with lower access to care, greater inequities, linguistic challenges, lower health literacy, older adults, and persons with mental health or cognitive issues. Follow-up studies include examining longer-term gains like patients having time to be prepared, MAs having more focused time in the room, and increased privacy especially in rural/small towns.
CONCLUSIONS
The pandemic forced us to explore innovative ways to address concerns about the feasibility of implementing self-rooming as a process redesign, without technology or building investments. Waiting rooms have become an unsafe way of serving our patients during this pandemic and beyond. Self-rooming is patient friendly and acceptable within staff workflows. Our organization and patients benefitted during the pandemic from this work to conclude that self-rooming is not only efficient, economical, and safer than the waiting room, but that it is also preferable to patients and staff, with minimal concerns compared with escorted rooming.
Acknowledgments
The authors gratefully acknowledge feedback from members of the Primary care Academics Transforming Health (PATH) group and manuscript preparation support from Peter Nordby and student assistants in the Health Innovation Program (HIP).
Footnotes
Conflicts of interest: authors report none.
Funding support: The project described was supported by the Primary Care Academics Transforming Healthcare (PATH) writing collaborative, the Health Innovation Program, and the Institute for Clinical and Translational Research, which is supported by the Clinical and Translational Science Award (CTSA) program, the National Center for Advancing Translational Sciences (NCATS), grant 1UL1TR002373. Dr Ramly is supported in part by a grant from the Agency for Healthcare Research and Quality (AHRQ K01 HS028926). The content is solely the responsibility of the authors and does not necessarily represent the official views of funders.
- Received for publication February 4, 2022.
- Revision received September 9, 2022.
- Accepted for publication October 10, 2022.
- © 2023 Annals of Family Medicine, Inc.




{kind=link}