
Article Figures & Data
Figures
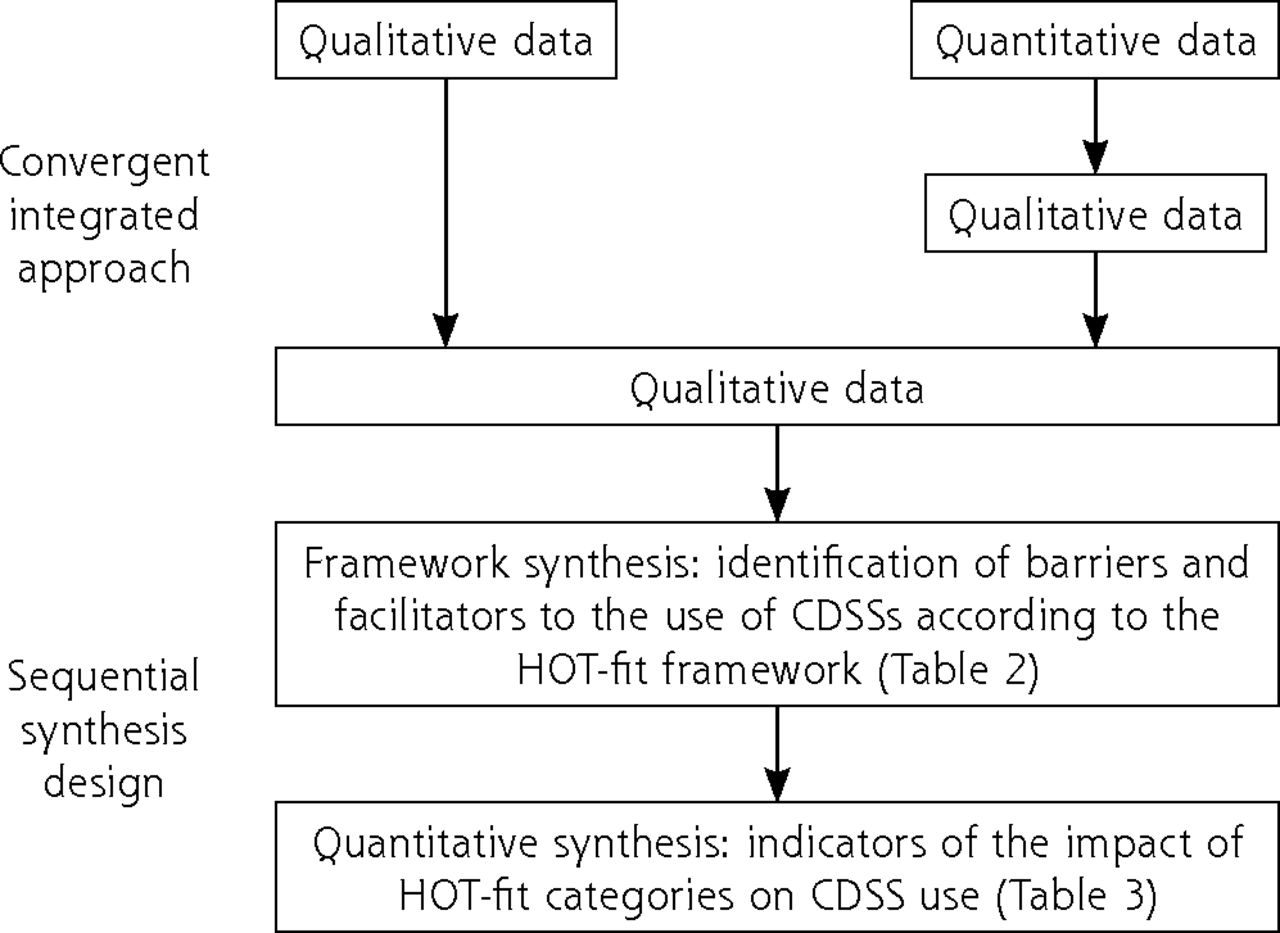
- Figure 1:
HOT-fit framework (derived from Yusof et al29).
HOT-fit = human, organization, technology, net benefits.
Note: The HOT-fit framework describes the interdependent human, organizational, and technological factors related to health information system adoption. A fit between the human, organizational, technological factors and the net benefit dimension is required for the adoption of these systems.
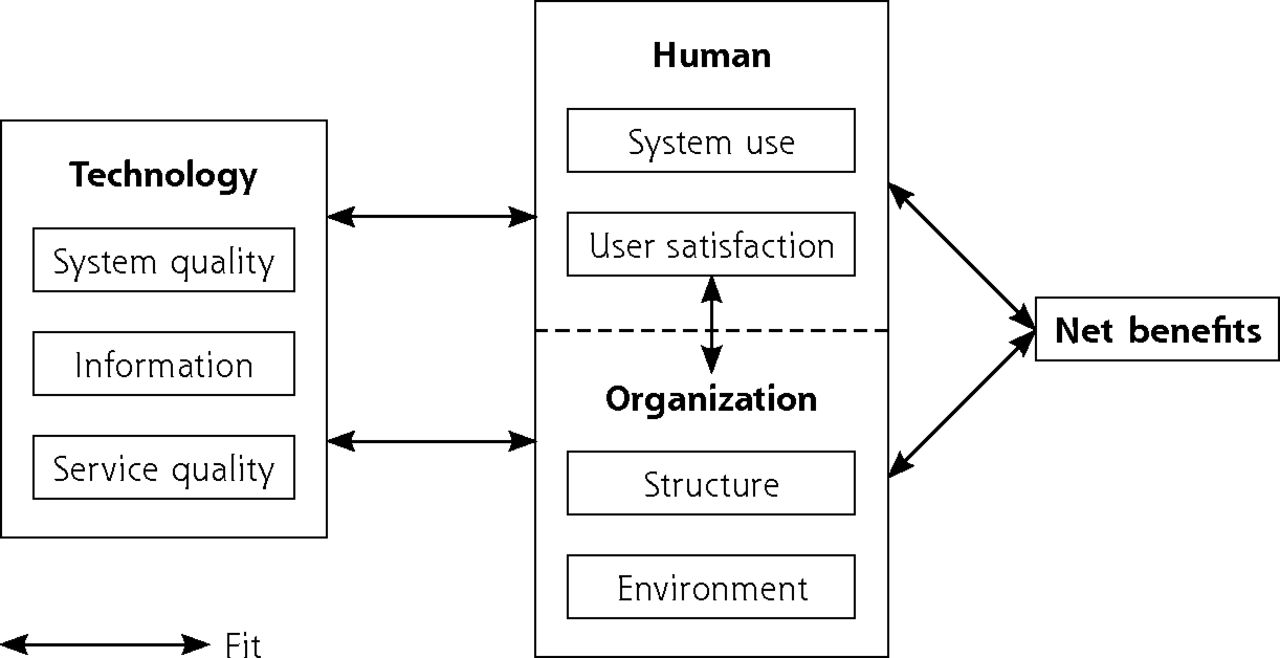
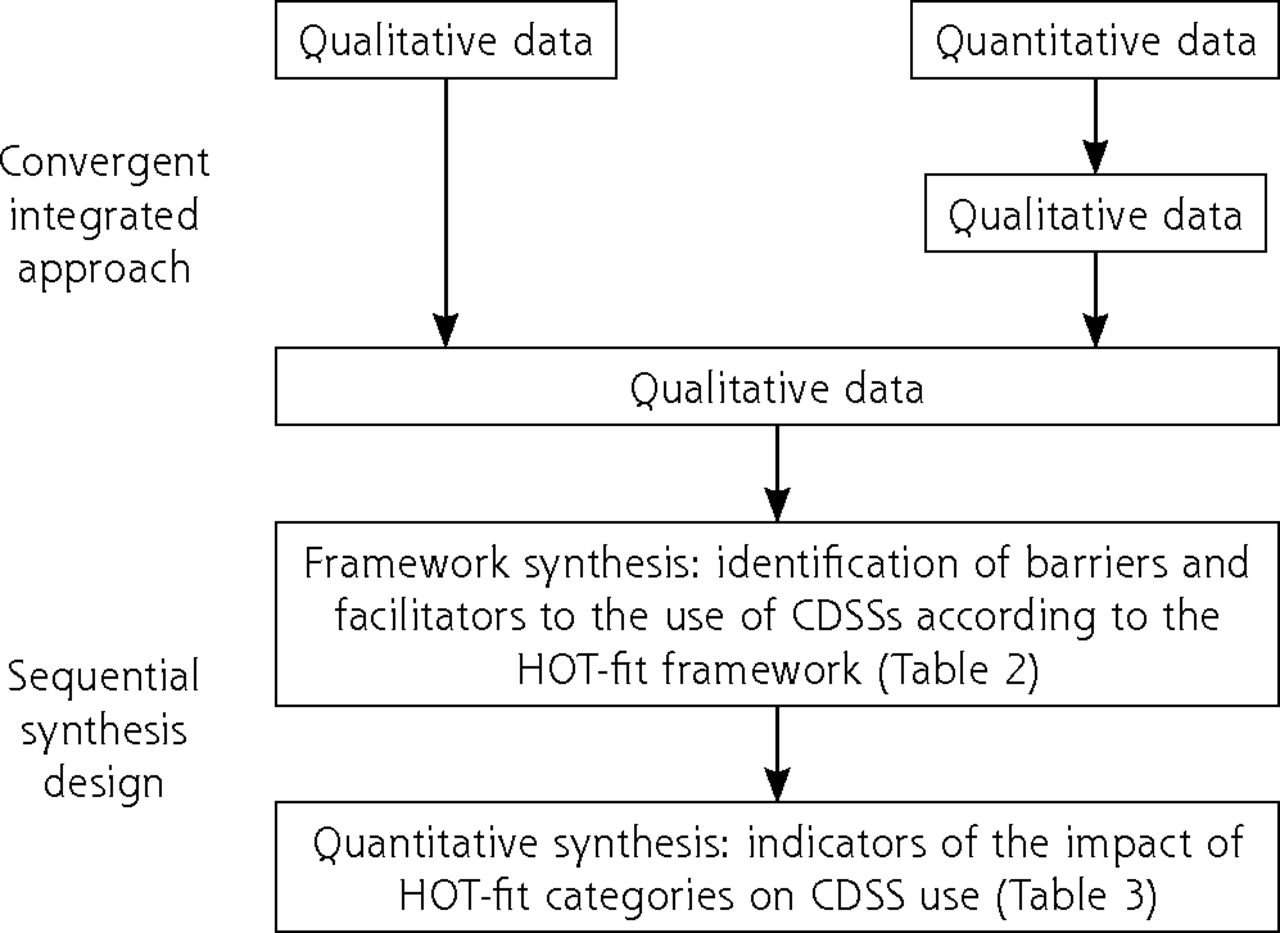
- Figure 2.
Mixed-methods synthesis design.
CDSS = clinical decision support system; HOT-fit = human, organization, technology, net benefits.
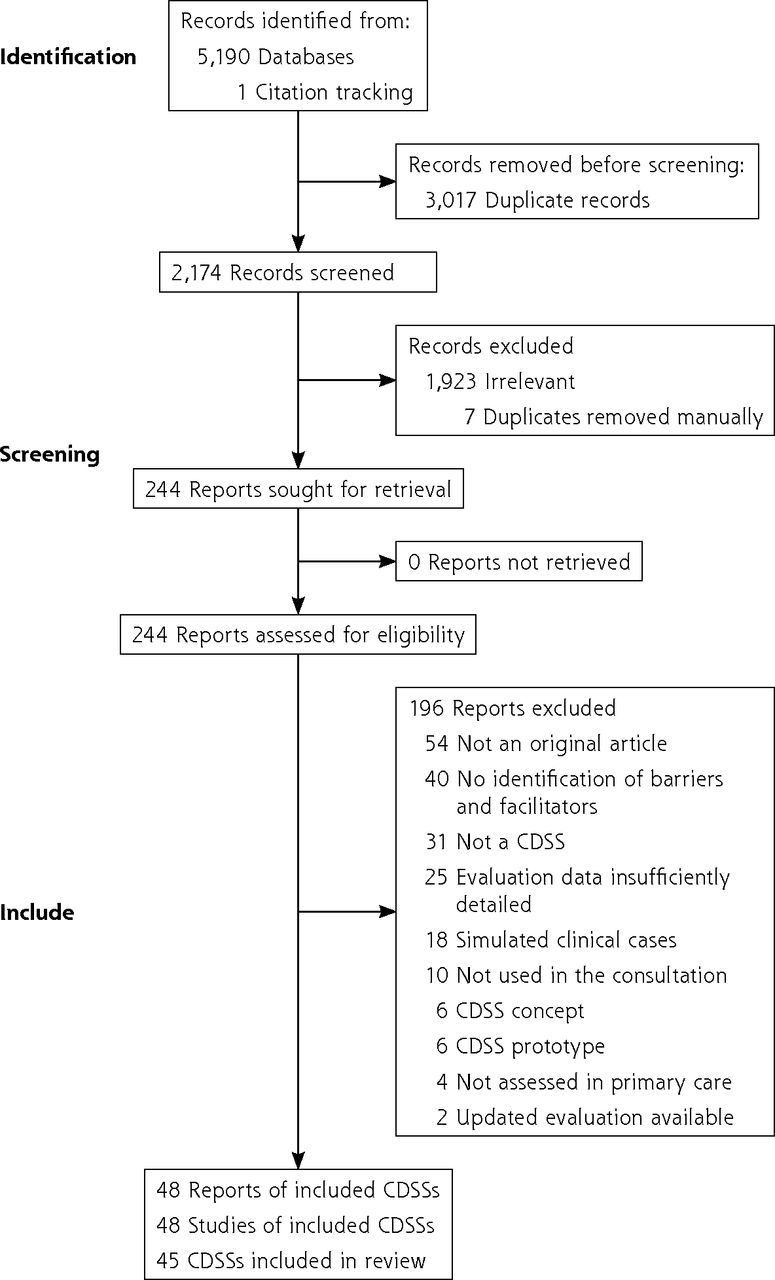
- Figure 3.
PRISMA flow chart.
CDSS = clinical decision support system; PRISMA = Preferred Reporting Items for Systematic Review and Meta-Analysis.


Tables
CDSS n = 45 in 48 Studies Name Country of Use Care Procedures Targeted Health Issues North America Alagiakrishnan et al,36 2016 SMART-CDS Canada Prevention (iatrogenesis) Adaption of medication to renal function from the patient’s EHR Ash et al38 2011 USA Diagnosis, Therapeutics (prescribing, vaccination) Drug-drug, drug-condition, and drug-allergy interaction checking, patient care plan dashboard with reminders, nearly 3,000 condition specific point-and-click templates for documentation Curry et al42 2011 Decision Support Server Canada Prevention (disease, test ordering) Prescription of diagnostic imaging Dixon et al43 2013 USA Prevention (disease, test ordering), Management of chronic disease(s) Diabetes mellitus type II, hypertension, coronary artery disease Doerr et al44 2014 My Family USA Prevention (disease, test ordering) Cancer risk management Edelman et al45 2014 The Pregnancy and Health Profile (PHP) USA Prevention (disease, test ordering) Prenatal genetic screening Feldstein et al46 2013 Patient Panel-Support Tool (PST) USA Prevention (iatrogenesis, disease, test ordering), Management of chronic disease Graphically displays ‘‘care gaps’’ (eg, for screening, medication use, monitoring, risk-factor control, vaccination) Guenter et al47 2019 McMaster Pain Assistant (MPA) Canada Diagnosis, Therapeutics (prescribing, vaccination) Neuropathic pain Jenssen et al51 2016 USA Prevention (disease, test ordering)
Therapeutics (prescribing, vaccination)Smoking cessation Kempe et al52 2017 Immunization information systems USA Prevention (disease, test ordering) Vaccination Lam Shin Cheung et al54 2020 eAMS Canada Therapeutics (prescribing, vaccination), Management of chronic disease(s) Asthma Lemke et al55 2020 GWA USA Prevention (disease, test ordering) Genetic risk assessment Litvin et al. (2012) ABX-TRIP CDSS USA Prevention (disease, test ordering), Diagnosis, Therapeutics (prescribing) Acute respiratory infections Litvin et al56 2016 USA Prevention (disease, test ordering) Identification and management of chronic kidney disease Minian et al62 2021 Canada Prevention (disease, test ordering) Alcohol cessation Montini et al63 2013 USA Prevention (disease, test ordering)
Therapeutics (prescribing, vaccination)Tobacco cessation Price et al67 2017 Canada Prevention (iatrogenesis) Potentially inappropriate prescriptions in the elderly Richardson et al68 2019 USA Therapeutics (prescribing, vaccination) Sore throat, upper respiratory tract infections Rubin et al72 2006 USA Therapeutics (prescrbiing, vaccination), Diagnosis Acute respiratory tract infections Trafton et al76 2010 ATHENA-OT USA Therapeutics (prescribing, vaccination) Opioid therapy for chronic, noncancer pain Trinkley et al77 2021 USA Therapeutics (prescribing, vaccination) Heart failure Williams et al79 2016 USA Prevention (disease, test ordering) Pediatric cardiovascular risk Zheng et al81 2005 CRS USA Prevention (iatrogenesis, disease, test ordering), Therapeutics (prescribing, vaccination), Management of chronic disease(s) Diabetes mellitus type II, hyperlipidemia, steroid-induced osteoporosis, influenza, pneumonia, breast cancer, cervical cancer Europe af Klercker et al35 1998 Sweden Diagnosis Ear, nose, throat diseases Arts et al37 2018 The Netherlands Management of chronic disease(s) Diabetes mellitus type II, atrial fibrillation, hypertension, medication prescriptions relating to care of older adults Bindels et al41 2003 GRIF Automated Feedback System The Netherlands Prevention (disease, test ordering) Comments on the appropriateness of diagnostic tests ordered by general practitioners Helldén et al48 2015 The renal button Sweden Prevention (iatrogenesis) Adaption of medication to renal function from the patient’s EHR Heselmans et al49 2020 and Koskela et al53 2016 EBMeDS Belgium, Estonia, Finland, Italy Prevention (iatrogenesis, disease, test ordering), Therapeutics (prescribing, vaccination), Management of chronic disease > 1,000 NICE-accredited international guidelines Lugtenberg et al58,59 2015 (2 articles) NHGDoc The Netherlands Prevention (disease, test ordering, iatrogenesis), Therapeutics (prescribing, vaccination), Management of chronic disease(s) Diabetes mellitus type II, cardiovascular risk management, asthma/COPD, thyroid disorders, viral hepatitis and other liver diseases, atrial fibrillation, subfertility Pannebakker et al64 2019 England Prevention (disease, test ordering) Pigmented skin lesions Rieckert et al68,69 2018, 2019 PRIMA-EDS Germany, Austria, Italy, England Prevention (iatrogenesis) Polypharmacy in older and chronically ill people Rousseau et al71 2003 England Therapeutics (prescribing, vaccination), Management of chronic disease(s) Asthma and angina in adults Toth-Pal et al75 2008 Evibase Sweden Management of chronic disease(s) Congestive heart failure Australia Abimbola et al34 2019 Health Tracker Australia Prevention (disease, test ordering) Cardiovascular risk management Bandong et al39 2019 My Whiplash
NavigatorAustralia Therapeutics (prescribing, vaccination) Whiplash-associated disorders Peiris et al65 2014 Australia Diagnosis, Therapeutics (prescribing, vaccination) Back pain management Wan et al78 2012 Australia Management of chronic disease(s) Diabetes mellitus type 2 Wilson et al80 2007 EMPOWER Australia Prevention (disease, test ordering), Therapeutics (prescribing, vaccination) Cardiovascular risk management, hypertension South America Maia et al60 2016 Brazil Management of chronic disease(s) Diabetes mellitus type II Marcolino et al61 2021 Brazil Prevention (disease, test ordering), Management of chronic diseases Diabetes mellitus type II, hypertension, cardiovascular risk treatment Silveira et al73 2019 TeleHAS Brazil Prevention (disease, test ordering), Therapeutics Cardiovascular risk management, hypertension Africa Bessat et al40 2019 REC Burkina Faso Diagnosis, Therapeutics (prescribing, vaccination) Follow-up and treatment of children under the age of 5 years in developing countries Jensen et al50 (2019) eIMCI South Africa Prevention (disease, test ordering), Therapeutics (prescribing, vaccination) Management of childhood illness Sukums et al74 2015 QUALMAT Burkina Faso, Ghana, Tanzania Therapeutics (prescribing, vaccination) Antenatal and intrapartum care Asia Praveen et al66 2014 India, Indonesia, Thailand Management of chronic disease(s) Cardiovascular risk management CDSS = clinical decision support system; COPD = chronic obstructive pulmonary disease; EHR = electronic health record; NICE = National Institute for Health and Care Excellence.
- Table 2.
Main Facilitators Reported in More Than 7 CDSSs, and Their Explanatory Elements, Classified According to the HOT-Fit Framework
HOT-Fit Framework Main Facilitatorsa (No. CDSSs Concerned) Explanatory Elements Factors and Dimensions (No. CDSSs concerned) Evaluation Measures Human (n = 41)
User satisfaction (n = 31)
Perceived usefulness
Training
Software satisfaction
Motivation to use
Overall satisfaction
Perceived usefulness of the CDSS (n = 23)
Training before use is appreciated (n = 10)
PCPs would continue to use the CDSS (n = 9)
Patients’ perceived usefulness of the CDSS increases PCPs motivation to use it (n = 7)
CDSSs increase PCPs satisfaction (n = 7)Organization (n = 41)
Structure (n = 39)Clinical process Natural integration of the CDSS in the clinical workflow (n = 13) Autonomy Producing reports of quality measures through collected data increases the value from the CDSS’s use in clinical practice (n = 7) Expansion of skill set and roles in assisting physicians and patients in meeting care needs Teamwork Other professionals ease physician’s increased workload with the CDSS (n = 6) Technology (n = 45)
System quality (n = 45)Ease of use The CDSS is user-friendly (ergonomic) (n = 30)
CDSS recommendations are easy to understand (n = 9)Usefulness of system features and functions Reminders (n = 8) Ease of learning Easy to use after a short learning period (n = 9) Information quality (n = 40) Usefulness Information provided is useful for the targeted process of care (n = 13)
Educational materials for patients are valuable (n = 7)General agreement with the validity of recommendations Format Pleasing visual layout [n = 12] Relevance Recommendations are relevant (n = 11) Reliability Recommendations are reliable (n = 9) Service quality (n = 11) Technical support Satisfaction with the CDSS service support (n = 7) CDSS technical staff availability Net benefits (n = 42) Effectiveness Potential to improve the quality of care (n = 23) Brings preventive care to the forefront Helps to systematize assessment of every patient Facilitates patient care management CDSS helps PCPs to improve guideline adherence (n = 11) Efficiency Using CDSS saves time (n = 22) Shortening documentation time Giving a quick patient evaluation from relevant data in patients’ EHRs Decision-making quality CDSS facilitates decision making (n = 22) CDSS is facilitating decision making about referral Communication CDSS helps focus on patient education (n = 18)
CDSS eases patient-PCP communication (n = 13)CDSS helps increase patient engagement Clinical practice CDSS is a way to update PCP’s knowledge (n = 17)
CDSS leads to better teamwork in primary care (n = 7)
CDSS increases PCPs’ self-confidence (n = 7)Error reduction CDSS helps PCPs to identify unrecognized information needs (n = 17) CDSS = clinical decision support system; EHR = electronic health record; HOT-fit = human, organization, technology, net benefits; PCP = primary care professional.
↵a Main facilitators are ranked by the number of CDSSs concerned.
- Table 3.
Main Barriers Reported in at Least 7 CDSSs, and Their Explanatory Elements, Classified According to the HOT-Fit Framework
HOT-Fit Framework Main Barriersa (No. CDSSs Concerned) Explanatory Elements Factors and Dimensions (No. CDSSs Concerned) Evaluation Measures Human (n = 41)
System use (n = 39)
Resistance or reluctance
Conflicts between CDSS recommendations and PCP expertise or beliefs (n = 18)
CDSS recommendations do not reflect the complexity of the situationReport acceptance Alert fatigue (n = 13)
Information overload (n = 8)Lack of a concise synthesis of the CDSS recommendation Training Training before use is needed (n = 11) The training session to the CDSS is inadequate or too short Attitude PCPs don’t need help with the targeted health issue (n = 8) Lack of engagement from PCPs (inertia of previous practice) (n = 8) Knowledge and expertise Lack of computer skills (n = 7) Motivation to use Ask for financial compensation to use the CDSS (n = 7) Organization (n = 41) Clinical process Using CDSS disrupts usual workflow (n = 25) Structure (n = 39) Teamwork Need of more teamwork with other PCPs to help physicians with CDSS’s increased workload (n = 13) Physicians fear more the CDSS workload than assistants or nurses Hardware Lack or computers or tablets (n = 7) Environment (n = 18) Inter-organizational relationship Difficulty to use CDSSs for patients comanaged by other specialists (n = 11) Information is sometimes missing or not integrated from external sources Technology (n = 45)
System quality (n = 45)Ease of use The CDSS is not user-friendly (n = 21) Need to switch windows in the EHR while using CDSSs Location of CDSS recommendations should be changed Need to switch windows between the EHR and the CDSS Turnaround time CDSS slowness (n = 16) CDSS’s slowness impairs the interaction with the patient and increases the consultation time Usefulness of system features and functions CDSS not fully integrated in the EHR (n = 14) A CDSS not fully integrated in the EHR is time consuming and disrupts workflow The most current information collected in the EHR is sometimes not updated in the CDSS Database contents The CDSS should target more health issues (n = 11) Questioning validity of CDSS’s knowledge database (n = 7) Concerns about the CDSS’s independence from pharmaceutical industry Flexibility Need of customization options (n = 8) Information quality (n = 40) Format Format of recommendations (length, structure, font colors) (n = 13) Reliability Doubtful reliability of the recommendations (n = 12) The reliability of the recommendations depends on the quality and completeness of the information collected Relevance Recommendations are not relevant (n = 11) Conflicts between patient complaints and unrelated CDSS recommendations
General recommendations are often irrelevantUsefulness Recommendations are not helpful (n = 8) Net benefits (n = 42) Efficiency Increased workload during the consultation (n = 33) Lack of time to use the CDSS during the consultation
Structured data collection takes too much time
Duplication of data collection
Coping strategies: increased consultation time, need of additional time to use the CDSS outside the consultation, scheduling follow-up consultationsNegative effect on patient-PCP communication (n = 7) CDSS = clinical decision support system; EHR = electronic health record; HOT-Fit = human, organization, technology, net benefits; PCP = primary care provider.
↵a Main barriers are ranked by the number of CDSSs concerned.
Human Organization Technology Net Benefits Mean impact of HOT-fit categories on CDSS use Slightly negative Slightly negative Neutral Positive Mean difference between barriers and facilitators (95% CI) −1.5 (−2.2 to −0.8) −1.9 (−2.6 to −1.1) −0.5 (−1.5 to 0.5) + 3.1 (2.2 to 3.9) CDSS = clinical decision support system; HOT-fit = human, organization, technology, net benefits; PCP = primary care professional.
Note: In the human factor, there was 1.5 additional barriers per CDSS than there were facilitators. In the net benefits dimension, there was 3.1 additional facilitators per CDSS than there were barriers.
Intrinsic features Including preventive care Covering a large array of conditions Providing reminders personalized to the patient Minimizing information overload and alert fatigue Providing educational materials to patients Integrated in the EHR, with the fewest possible duplicate data entries Fast processing Contextual features Developed in close collaboration with PCPs Providing the rationale for the selection of sources of its knowledge base With teamwork for data collection and use of the CDSS With systematic training for its use CDSS = clinical decision support system; EHR = electronic health record; PCPs = primary care professionals.
SUPPLEMENTAL MATERIALS IN PDF FILE BELOW
- Meunier.pdf -
PDF file
- Meunier.pdf -
In this issue




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Barriers to and facilitators of clinician acceptance and use of artificial intelligence in healthcare settings: a scoping review
- HIV Pre-exposure Prophylaxis (PrEP) Practices in Florida, USA: Clinicians Perceptions of Initiation, Risk Identification, Barriers, and Facilitators
- 'Do they care?: a qualitative examination of patient perspectives on primary care clinician communication related to opioids in the USA
- Barriers and facilitators to implementing imaging-based diagnostic artificial intelligence-assisted decision-making software in hospitals in China: a qualitative study using the updated Consolidated Framework for Implementation Research
- Barriers and Facilitators to Using a Clinical Decision Support Tool for Opioid Use Disorder in Primary Care