
Article Figures & Data
Figures
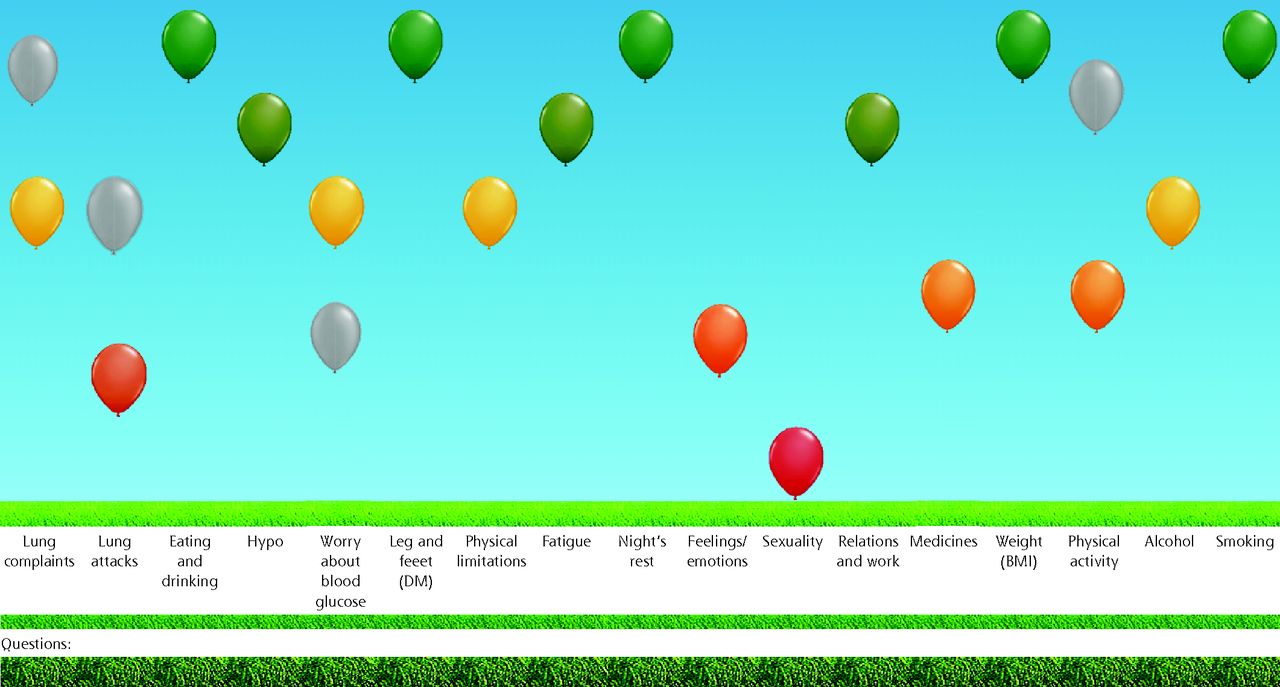
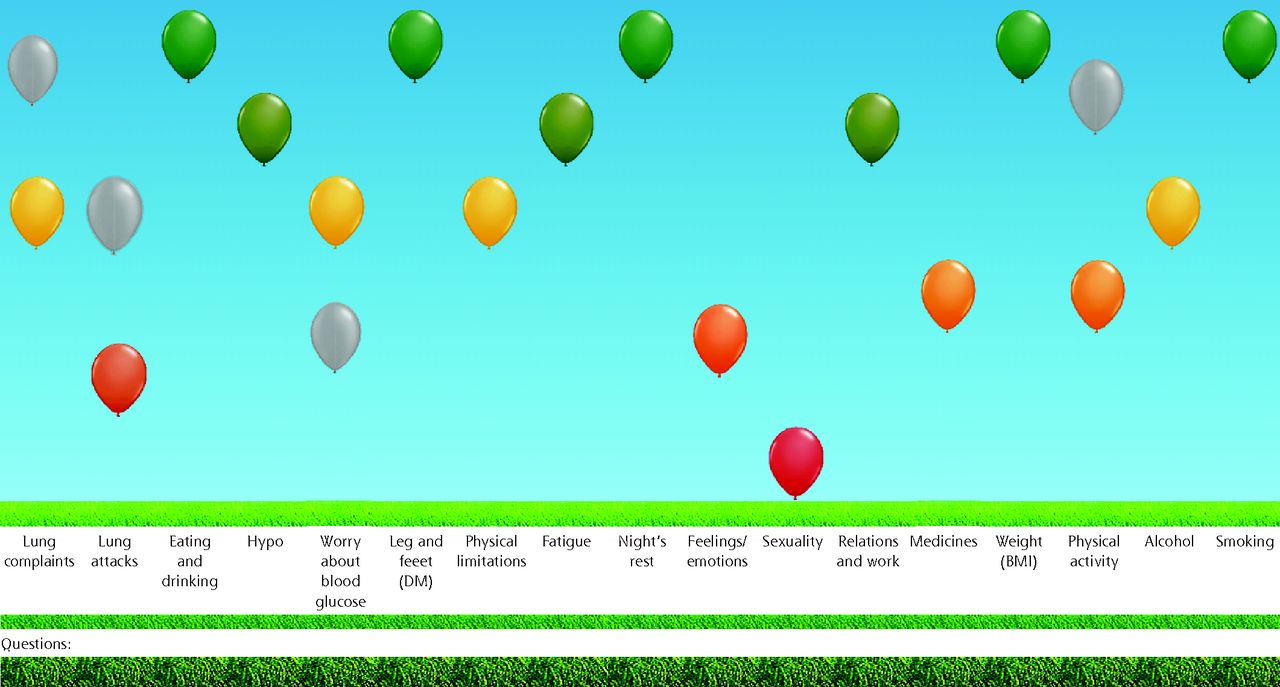
- Figure 1.
Visual representation of the ABCC scale outcomes.
ABCC = Assessment of Burden of Chronic Conditions; BMI = body mass index; DM = diabetes mellitus; Hypo = hypoglycemia.
The outcomes of the ABCC scale are visualized into a balloon chart. High green balloons indicate low burden. Low red balloons indicate high burden. Orange and yellow balloons indicate changes between red and green. The results from the previous visit are depicted in gray for easy monitoring.
Tables
Outcome COPD Asthma T2D Convergent validity Comparator instrument SGRQ AQLQ-S ADDQoL19 Comparisons ABCC total SGRQ total ABCC total AQLQ-S total ABCC total ADDQoL19 total Physical limitations All subscales Physical limitations Total Symptoms Activity Feelings and emotions Self confidence
Feelings about the futurePulmonary complaints All subscales Feelings and emotions Emotional functioning Physical limitations Physical
Depend on others… … … … Sexuality Sex life … … … … Eating and drinking Freedom to eat
Freedom to drinkThreshold for validity, r r ≥0.7 r ≤−0.7a Total score r <−0.7a
Subscores −0.7 < r <−0.3a,bKnown group validityc Known group 1 Exacerbation count:
<2 vs ≥2dExacerbation count:
0 vs ≥1dInsulin use:
none vs anyHypothesized distinguishable ABCC domains Total score
Night’s rest
Physical limitation
Relations and work
Pulmonary complaintsTotal score
Night’s rest
Feelings and emotions
Relations and work
Asthma complaintsTotal
Feelings and emotions
Physical limitations
Relations and work
Hypoglycemia
Worry about futureKnown group 2 Depression:
HADS <8 vs HADS ≥8GINA:
Controlled vs notComplications:
none vs anyeHypothesized distinguishable ABCC domains Total score
Fatigue
Feelings and emotions
Physical limitations
Relations and work
Pulmonary complaintsTotal score
Night’s rest
Feelings and emotions
Physical limitations
Relations and work
Sexuality
Asthma complaintsTotal
Feelings and emotions
Physical limitations
Relations and workKnown group 3 … … Obesity:
BMI <30 vs ≥30Hypothesized distinguishable ABCC domains … … Total
Feelings and emotions
Physical limitations
Relations and work
Eating and drinkingInternal consistency
Accepted threshold, αTotal scale α ≥0.9; subscales α ≥0.7 Test-retest reliability
Accepted threshold, ICCICC ≥0.9 α = Chronbach’s alpha; ABCC = Assessment of Burden of Chronic Conditions; ADDQoL19 = 19-item Audit of Diabetes-Dependent Quality of Life; AQLQ-S = Standardized Asthma Quality of Life Questionnaire; BMI = body mass index; COPD = chronic obstructive pulmonary disease; GINA = Global Initiative for Asthma; HADS = Hospital Anxiety and Depression Scale; ICC = intraclass coefficient; QoL = quality of life; r = Pearson correlation coefficient; SGRQ = Saint George Respiratory Questionnaire; T2D = type 2 diabetes.
↵a As the ABCC scale implies high burden at high scores, and both the AQLQ and ADDQoL19 imply high burden (or low QoL) at low scores, the correlation between these scales is inverse and thus negative.
↵b Both scales have single-item domains/subscores, therefore the hypothesized correlation is expected to be moderate.
↵c Significant difference in groups, P ≤.05.
↵d Based on Dutch medical guidelines.14,15
↵e Any of the following complications: nephropathy, neuropathy, retinopathy, sexual dysfunction, amputation of any limb, diabetic foot, cardiovascular disease.
Characteristic COPD
(n = 65)Asthma
(n = 62)T2D
(n = 60)Male sex, No. (%) 39 (60.0) 19 (30.6) 30 (50.0) Age, mean (SD), y 66 (6.9) 56 (13.4) 66 (9.5) Highest level of education, No. (%)a Lowb 26 (40.0) 18 (29.0) 29 (48.3) Middlec 3 (4.6) 10 (16.1) 6 (10.0) Highd 36 (55.4) 34 (54.8) 25 (41.7) Diagnosed since, No. (%), y <1 1 (1.5) 1 (1.6) 1 (1.7) 1-3 4 (6.2) 4 (6.5) … >3 60 (92.3 57 (91.9) … 1-15 … … 40 (66.7) >15 … … 19 (31.7) Smoking status, No. (%) Never 6 (9.2) 34 (54.8) … Former 58 (89.2) 28 (45.2) … Current 1 (1.5) 0 (0.0) … Treated by, No. (%) General practitioner 11 (17.5) 17 (31.5) 48 (82.8) Medical specialist 52 (82.5) 37 (68.5) 10 (17.2) Unknown 2 8 2 Exacerbations, previous year, No. (%) 0 19 (29.2) 16 (25.8) … 1 19 (29.2) 8 (12.9) … 2 9 (13.8) 15 (24.2) … >2 18 (27.7) 23 (37.1) … Medication, No. (%) No medication 0 (0.0) 1 (1.6) 5 (8.3) Any of the following: SABA/SAMA 40 (61.5) 45 (72.6) … LABA/LAMA 49 (75.4) 22 (35.5) … ICS 17 (26.2) 37 (59.7) … Combination medication (ICS + LABA/LAMA) 35 (53.8) 43 (69.4) … Metformin … … 40 (66.7) Gliclazide, glimepiride, or tolbutamide … … 22 (36.7) Insulin … … 27 (45.0) COPD = chronic obstructive pulmonary disease; ICS = inhaled corticosteroids; LABA = long-acting β2-agonist; LAMA = long-acting muscarinic antagonists; SABA = short-acting β2-agonist; SAMA = short-acting muscarinic antagonists; T2D = type 2 diabetes.
↵a According to the Education Systems in the Netherlands.39
↵b Elementary school, pre-vocational secondary education and training, or secondary vocational education and training.
↵c Senior general secondary education or pre-university education.
↵d Higher professional education or university education.
Convergent validity, SGRQ, r ABCC domains Total Activity Impact Symptoms ABCC total 0.866a 0.797a 0.806a 0.734a Physical limitation 0.829a 0.831a 0.743a 0.668 Pulmonary complaints 0.761a 0.636 0.697 0.773a Known group validity, median (IQR) <2
Exacerbations E
(n = 33)≥2
Exacerbations
(n = 32)P value ABCC total 1.6 (0.9-2.6) 2.6 (2.4-3.6) <.001 Night’s rest 2.0 (0.5-2.5) 2.5 (2.0-3.0) .006 Feelings and emotions 1.0 (0.3-2.0) 2.0 (1.0-2.7) .010 Physical limitations 2.3 (1.0-4.2) 3.7 (3.0-4.9) .003 Relations and work 1.0 (0.5-3.0) 3.0 (2.0-4.0) <.001 Pulmonary complaints 2.3 (1.6-3.0) 3.3 (2.6-3.9) <.001 Not depressedb
(n = 50)Depressedb
(n = 15)P value ABCC total 2.1 (1.2-2.9) 3.1 (2.5-3.9) .001 Fatigue 3.0 (2.0-4.0) 4.0 (3.0-5.0) .022 Feelings and emotions 1.0 (0.3-2.0) 2.0 (1.7-2.7) .001 Physical limitations 3.0 (1.3-4.3) 3.7 (3.0-4.7) .057 Relations and work 2.0 (1.0-3.0) 3.0 (3.0-4.0) .002 Pulmonary complaints 2.6 (1.8-3.5) 3.0 (2.5-4.0) .061 Reliability measures Internal consistency, Cronbach’s α (95% CI) Total scale 0.90 (0.86-0.93) Physical limitations 0.92 (0.88-0.95) Feelings and emotions 0.77 (0.64-0.85) Pulmonary complaints 0.65 (0.49-0.77) Test-retest reliability, ICC (95% CI) (n = 60) 0.95 (0.92-0.97) ABCC = Assessment of Burden of Chronic Conditions; COPD = chronic obstructive pulmonary disease; ICC = intraclass coefficient; IQR = interquartile range; HADS = Hospital Anxiety and Depression Scale; r = Pearson correlation coefficient; SGRQ = Saint George Respiratory Questionnaire.
↵a r >0.7.
↵b Depression determined with HADS score, <8 not depressed, ≥8 depressed.
Convergent validity, AQLQ-S, r ABCC domains Total Symptoms Activity Limitation Emotional Function ABCC total −0.851a −0.842a −0.831a … Feelings and emotions … … … −0.725a Physical limitation −0.777a −0.782a −0.797a … Asthma complaints −0.835a −0.865a −0.805a … Known group validity, median (IQR) No Exacerbations
(n = 16)≥1 Exacerbations
(n = 46)P value ABCC total 1.5 (0.9-1.9) 2.5 (1.8-3.1) <.001 Night’s rest 2.0 (1.0-2.0) 3.0 (2.0-4.0) .001 Feelings and emotions 1.0 (0.8-1.3) 1.3 (0.6-2.0) .049 Physical limitations 1.7 (0.7-2.0) 2.3 (1.7-3.3) <.001 Relations and work 1.0 (0.0-2.0) 3.0 (2.0-4.0) .001 Asthma complaints 0.8 (0.5-1.6) 3.0 (2.0-3.8) <.001 Controlledb
(n = 18)Uncontrolledb
(n =43)P value ABCC total 1.4 (1.0-1.8) 2.7 (2.0-3.2) <.001 Night’s rest 2.0 (1.0-3.0) 3.0 (2.0-4.0) 0.003 Feelings/emotions 0.5 (0.0-1.0) 1.3 (1.0-2.0) <.001 Physical limitations 1.0 (0.7-2.0) 2.3 (1.7-3.3) <.001 Relations and work 1.0 (0.0-2.0) 3.0 (2.0-4.0) <.001 Sexuality 0.5 (0.0-2.0) 2.0 (0.0-3.0) .042 Asthma complaints 0.8 (0.2-1.5) 3.0 (2.3-3.8) <.001 Reliability measures Internal consistency, Cronbach’s α (95% CI) Total scale 0.92 (0.89-0.95) Physical limitations 0.88 (0.82-0.93) Feelings and emotions 0.74 (0.60-0.83) Asthma complaints 0.73 (0.61-0.83) Test-retest reliability, ICC (95% CI) (n = 60) 0.93 (0.87-0.96) ABCC = Assessment of Burden of Chronic Conditions; AQLQ-S = Standardized Asthma Quality of Life Questionnaire; ICC = intraclass coefficient; IQR = interquartile range; GINA = Global Initiative for Asthma; r = Pearson correlation coefficient.
↵a r < −0.7.
↵b Groups determined by GINA guidelines. Well and partially controlled combined into single group.
Convergent validity, ADDQoL19, r ABCC domains ADDQoL19 domains r ABCC total Average WI −0.548 Feelings and emotions Self-confidence −0.260 Feelings about the future −0.379a Physical limitations Physical −0.391a Depend on others −0.459a Relations and work Leisure −0.441a Work −0.664a Family life −0.413a Friendships and social life −0.448a Sexuality Sex life −0.650a Eating and drinking Freedom to eat −0.346a Freedom to drink −0.167 Known group validity, median (IQR) Insulin independent
(n = 32)Insulin dependent
(n = 27)P value ABCC total 1.1 (0.7-1.5) 1.9 (1.4-2.7) .001a Feelings and emotions 1.0 (0.5-1.9) 1.5 (1.0-3.0) .025a Physical limitations 1.0 (0.3-1.7) 2.7 (1.3-3.0) .004a Relations and work 0.0 (0.0-1.0) 2.0 (0.0-3.0) .005a Hypoglycaemia 1.0 (0.0-1.8) 2.0 (0.0-2.0) .038a Worry about future 1.0 (0.0-2.0) 2.0 (1.0-3.0) .051 No complications
(n = 12)≥1 complications
(n = 48)P value ABCC total 0.9 (0.4-1.3) 1.7 (1.1-2.6) .001a Feelings/emotions 0.5 (0.0-1.0) 1.3 (1.0-2.5) .001a Physical limitations 0.5 (0.0-1.5) 1.7 (1.0-3.0) .007a Relations and work 0.0 (0.0-1.0) 1.0 (0.0-2.0) .031a BMI <30
(n = 44)BMI ≥30
(n = 16)P value ABCC total 1.2 (0.8-2.1) 1.9 (1.5-2.8) .008a Feelings and emotions 1.0 (0.5-1.9) 1.8 (1.0-2.5) .003a Physical limitations 1.2 (0.3-2.6) 2.9 (1.4-3.6) .003a Relations and work 0.0 (0.0-2.0) 2.0 (1.0-2.0) .018a Eating and drinking 2.0 (1.0-2.8) 1.5 (1.0-3.8) .830 Reliability measures Internal consistency, Cronbach’s α (95% CI) Total scale 0.91 (0.87-0.94) Physical limitations 0.87 (0.80-0.92) Feelings and emotions 0.76 (0.60-0.85) Test-retest reliability, ICC (95% CI) 0.95 (0.91-0.97) ABCC = Assessment of Burden of Chronic Conditions; ADDQoL19 = 19-Item Audit for Diabetes-Dependent Quality of Life; BMI = body mass index; ICC = intraclass coefficient; IQR = interquartile range; r = Pearson correlation coefficient; WI = weighted impact.
↵a r < −0.7 for total scales or −0.7 < r < −0.3 for single item-correlations.
SUPPLEMENTAL MATERIALS IN PDF FILE BELOW
- ClaessensSuppApps.pdf -
PDF file
- ClaessensSuppApps.pdf -




{kind=link}