
Abstract
This article explains the importance of a communities of practice (CoP) model for continually aligning medical education and clinical transformation with contemporary health issues. It describes the evolution and advantages of using CoP as a model for transforming medical education and clinical practice and applies the CoP methodology to addressing the changing needs of socially vulnerable populations (LGBTQ [lesbian, gay, bisexual, transgender, and queer/questioning], persons experiencing homelessness, and migrant farm workers). In conclusion, this article describes CoP-led activities, achievements, and value creation in medical education by the National Center for Medical Education Development and Research established at the Meharry Medical College.
- communities of practice
- primary care
- medical education, systematic review
- vulnerable populations, LGBTQ
INTRODUCTION
Given the rapid changes in the demographic, social, and personal health landscapes, the health care sector needs to continually update and reinvent itself to meet the evolving needs of people it serves. Changes in health insurance products,1 use of information technology,2 big data analytics,3 and predictive modeling,4 as well as changing diagnostic tools,5 prescription drugs,6 and expectations of consumers7 will continue to revolutionize how health care is delivered in the coming decade. These changes will increase pressures on health professions training programs to keep up with the changes that are occurring in the real world. Training challenges facing the health care sector include new health care delivery methods,8 recruitment of a diverse applicant pool,9 use of new technologies,10 and rapid advancement in bio-medical, clinical, and public health science.11
Mitigating these challenges will require effective knowledge management (KM) initiatives that introduce novel instructional methods and concepts to health professions (medical, dental, nursing, pharmacy, optometry, physician assistant programs, etc) students, residents, fellows, and current health practitioners using novel learning channels.12,13 Knowledge management is the collection of methods relating to creating, sharing, using, and managing knowledge and information. It refers to a multidisciplinary approach for achieving organizational objectives by making the best use of knowledge. Achieving KM objectives within the health care sector will require an ability to create, transfer, and utilize knowledge to prepare trainees for the continually evolving health care ecosystem.14 One of the KM initiatives that has gained prominence in recent years in the health care sector is Communities of Practice (CoP).15 Medical communities have a vested interest in KM/CoP, especially in the health care industry. One area where CoP can have a big impact is evidence-based medical practices (EBMP), which integrate research evidence, clinical expertise, and patient preferences in clinical decision making, throughout the health care delivery process.16,17
Communities of Practice Concept and Structure
Social learning theorists Lave and Wenger,18 early proponents of CoP, define it as groups of people who share a concern or a passion for something they do, and who learn how to do better as they interact regularly. The authors aligned their creation of CoP within social learning theory and embedded it in the science of anthropology and systems theory.19,20 Wenger-Trayner et al21 revealed that the concept of education can be viewed as a simple social system, while the engagement of a CoP in the educational process constitutes a complex social system. According to Wenger-Trayner, CoP must embrace 3 elements: domain, community, and practice. The application of these 3 CoP elements requires the implementation of characteristics that include (1) a community that is pursuing a particular interest in which members are involved, (2) engagement in shared and/or joint activities, and (3) bi-directional interactions that benefit all participants through sharing of information and experiences. According to Wenger et al,22 application of a CoP promotes transformation through engagement of persons with a vested interest in the same cause, different knowledge and experiences, and a common purpose. Common purpose refers to the activity or event that binds a group of interested people.
The business sector was the first to embrace the CoP concept, followed by the health care sector.23 Early health care studies that used CoP focused on learning and exchanging information and knowledge, whereas more recently, CoP has been used as a tool to develop health literacy,24 improve clinical practice and implement evidence-based practice.25,26 Successful application of the CoP model has been used to support decision making in maternal health programs in Mexico and Nicaragua,27 the Michigan Keystone ICU program,28 a lung cancer outcomes project in UK,28 and overall cancer care in Canada.29
Recent technological innovations in the communications sector have created new opportunities for online collaboration that allow individuals to meet in a virtual setting, eliminating geographical barriers (time zones notwithstanding) and transforming the traditional CoP into a virtual CoP (VCoP). Recent results of our own comprehensive review of literature of the successes of VCoP,30 and a web-based survey of health care providers,2 found satisfaction with the quality of shared knowledge, operations, and service provided by VCoP.
Community-oriented medical education (COME) is an emerging strategy for producing health-oriented professionals who are equipped with broad skills and able to integrate health promotion, disease prevention, and treatments. Community-oriented medical education provides a model that not only enables medical schools but also other allied health professions (mentioned above) to be more responsive to the local and broader communities it serves.31 Additionally, COME identifies opportunities for addressing underlying systemic causes of health disparities that are shaped by social, cultural, environmental, and historical context of each community and provide optimal care to both individuals and communities. A CoP model provides an ideal platform for engaging community partners in the transformative re-envisioning of medical education for the future that can be adapted at a local level to address emerging health needs of the diverse, multiple communities it serves.32
Utilizing the CoP to enhance learning endeavors, in the context of clinical education, has been demonstrated to be effective. Studies conducted to test the efficacy of CoP in a nursing school setting revealed significant improvement in learning outcomes of students.33 The findings revealed that creating an environment that fosters dialog with senior members of the community, together with successful mentoring, establishes strong connections within peer groups, and helps students navigate roadblocks and mitigate errors in clinical practice. A mixed methods study conducted by Bing-You and Varaklis34 found that organizing residency and fellowship programs into distinct CoPs yielded positive changes in group identity, availability of resources, and opportunities for professional growth. A systematic review of literature undertaken by Barbour et al35 also revealed that CoP-led interventions have been shown to have a great impact across a range of public health practice, such as nutrition, obesity, mental health, tobacco smoking, etc and communities, including the United States, Canada, Australasia, and the United Kingdom. The interventions assisted in structural problem solving, reflective practice, and creation of networking opportunities for participants. Cruess et al26 proposed use of CoP as the theoretical framework for restructuring medical education.
Advancing Health Equity Through Communities of Practice: The National Center for Medical Education Development and Research
A CoP model offers new opportunities for transforming primary care training in both undergraduate and graduate medical education. Here we report on the success we made in employing CoP in primary care training. In 2016, the National Center for Medical Education Development and Research (NCMEDR) was established in the Department of Family and Community Medicine at Meharry Medical College, with funding from Health Resources and Service Administration (HRSA) to examine the question: How are medical students being taught to provide primary care services to 3 socially vulnerable populations such as lesbian, gay, bisexual, transgender, and queer/questioning (LGBTQ) people, people experiencing homelessness, and migrant farm workers?
The rationale for this program was that there has been a growing recognition that biased attitudes and beliefs of health care clinicians toward LGBTQ patients, and other socially vulnerable populations, contribute to disparities through their impact on health care access and quality of clinical care.36 Socially vulnerable patients face many health challenges including bias, psychosocial issues (discrimination, depression, anxiety, fear, etc), intimate partner violence, addiction to alcohol, and substance abuse that often go unrecognized.37-39 Two other vulnerable populations—people experiencing homelessness40 and migrant farm workers—experience poverty and lack of transportation, as well as chronic health issues.41 Lack of access to care and lack of trained clinical staff to treat patients with compassion are some of the gaps identified in the care provided to these populations.42 The unmet health needs of vulnerable populations warrants foundational knowledge acquisition by students through participation in specifically designed experiential community components in the medical education curriculum43 that include community outreach and health education programs.40 The purpose of this article was to review the various CoP-led activities at NCMEDR with implications for developing a curricular framework and processes for addressing the needs of vulnerable populations.
The NCMEDR initially established guiding principles for selection of members for its CoP practices. These included: (1) recruiting a diverse team of academicians, primary care physicians (from specialties such as family medicine, internal medicine, and pediatrics), psychiatrists, reproductive medicine specialists, surgeons, other allied health professionals, policy makers, and other community partners, members with lived experience, including patients; (2) engaging national organizations such as HRSA, National Institutes of Health (NIH), Agency for Healthcare Research and Quality (AHRQ), American Association of Medical Colleges (AAMC), Internal Association of Medical Science Educators (IAMSE), etc, and academic institutions, faith-based organizations, community groups (National Coalition for the Homeless, Migrant Clinician Network), lay persons, medical students, and residents; (3) conducting regular meetings (weekly) to identify, translate, and disseminate evidence-based best practices in medical education curriculum; (4) convening webinars, developing certification programs, providing clinic experiences, and hosting an annual CoP conference; (5) identifying/designing evidence-based strategies for teaching medical students about addressing the health care needs of these 3 vulnerable populations; and (6) evaluating effectiveness of dissemination strategies in transmitting research results to persons involved with medical education across the nation.
In this section, specific examples are reported on how we at NCMEDR have applied the CoP concept since 2017 by conducting monthly CoP meetings and hosting annual CoP conferences every year to revise primary care medical education curriculum with special reference to meeting the needs of these 3 socially vulnerable populations. We adopted Wenger’s22 classification of 3 characteristics of CoP that started by identifying domain, community, and practice.
Domain
The shared domain, or purpose, was identified as persons committed to improving health outcomes for 3 vulnerable populations through medical education curriculum transformation.
Each year, 2 different health topics were explored for each vulnerable population. Research topics, per year, were:
Year 1: physician implicit bias and pre-exposure prophylaxis
Year 2: adverse childhood experiences and interpersonal violence across the life course
Year 3: opioid misuse and sexual violence
Year 4: immunization disparities and affirming care
Year 5: telehealth and mental health
We focused on these topics to expand our understanding of the unique health care needs of vulnerable populations and identify strategies for transforming primary care curriculum in medical education and clinical practice. The NCMEDR staff conducted surveys to identify if and how medical education curriculum across medical schools in United States addressed the needs of LGBTQ individuals, persons experiencing homelessness, and migrant farmer workers. Specifically, we sought to identify that the topic was addressed, the course in which the subject was covered, how many hours were devoted to the topic, and what teaching methods were used during which year of medical school. For each of the research topics, NCMEDR conducted a systematic review, which enabled the NCMEDR staff and CoP to assess the evidence base on teaching models and identify the curricular gaps in medical education.
Community
The CoP community was identified as group of individuals who possess the required knowledge and skills. Members were recruited by identifying national experts, both from reviewing the literature on health issues experienced by each of the 3 vulnerable populations and recommendations from clinicians, peers, and scientific societies. CoP members included persons with expertise in medical education, service providers for each of the 3 vulnerable populations, persons with lived experience, leaders from faith-based organizations, policy analysts, patients, caregivers, allied health professionals, and lay persons. The charge of the CoP was to inform the research through the sharing of discipline-specific content knowledge, and work and lived experiences.
Practice
Practice was identified as a set of activities/events to achieve the outcomes. The practice adopted by the CoP was to guide and review the research undertaken by NCMEDR investigators, translate findings into public health, clinical, and policy recommendations, to develop model curriculum modules and policy briefs, and to assist with the dissemination of research products to institutional and professional colleagues and community partners, through presentations, peer-reviewed articles, a website (www.NCMEDR.org), and social media.
The CoP conducted a systematic review of the literature on each research topic to identify how medical schools in United States have addressed the topics in their educational curriculum and to identify the effectiveness of educational programs in addressing the needs of LGBTQ patients, people experiencing homelessness, and migrant farm workers on a series of topics, including: medical student/physician implicit bias,44 interpersonal violence,45 adverse childhood experiences,46 opioid use,47 pre-exposure prophylaxis,48 affirming and inclusive care.30 As part of our systematic reviews, we conducted searches of online databases (eg, MEDLINE/ PubMed, PsycINFO, Web of Science, Scopus, Ingenta, Science Direct, and Google Scholar) for original articles published in English and collected various study characteristics, including sample, study design, program format, program target, and pertinent outcomes. Effectiveness of interventions included those that increased knowledge about the health care needs of each of the 3 vulnerable populations, promoted positive attitudes toward them, increased comfort in working with them, and/or resulted in behavioral change. Although support was found for promising interventions for behavioral change, overall results found minimal to moderate evidence for educational interventions that addressed the needs of socially vulnerable populations or resulted in improved clinical outcomes of the target population.
Our interdisciplinary research team, guided by the CoP, also completed an online survey of 141 US medical schools to determine if and how the school’s medical education curriculum addressed Pre-Exposure Prophylaxis (PrEP)47 and implicit biases49 toward the 3 vulnerable patient groups. The survey was structured using the Research Electronic Data Capture (REDCap) web-based platform and branching logic. If the survey respondent indicated that medical students received training on implicit bias relevant to a specific patient group in the vulnerable populations’ category, then several follow-up questions were shown in a drop-down menu format. Seventy-one medical schools responded to our survey. Our findings revealed that almost one-half of the medical school respondents implemented bias reduction training in their curriculum. Implicit bias training most frequently addressed LGBTQ persons (39%), followed by migrant farmworker patients (14%) and patients experiencing homelessness (11%).49 Responses about training on PrEP was limited to curricular discussions about LGBTQ persons (15.4%). No medical schools indicated that their curriculum on PrEP addressed the unique needs of either migrant farmworker patients or patients experiencing homelessness.48 Study findings underscored the need for formulating curriculum strategies that address both specific emerging topics (eg, the reduction of implicit bias or the introduction of patient discussions about PrEP), as well as strategies that were specific to the unique conditions and circumstances experienced by each of the vulnerable populations. Our recommendations supported the engagement of faculty, trainees, and stakeholders (service providers and vulnerable patient groups) in the development of the curriculum to provide students with opportunities to recognize the importance of the different perspectives offered by engaging both interdisciplinary professionals and persons with lived experiences.
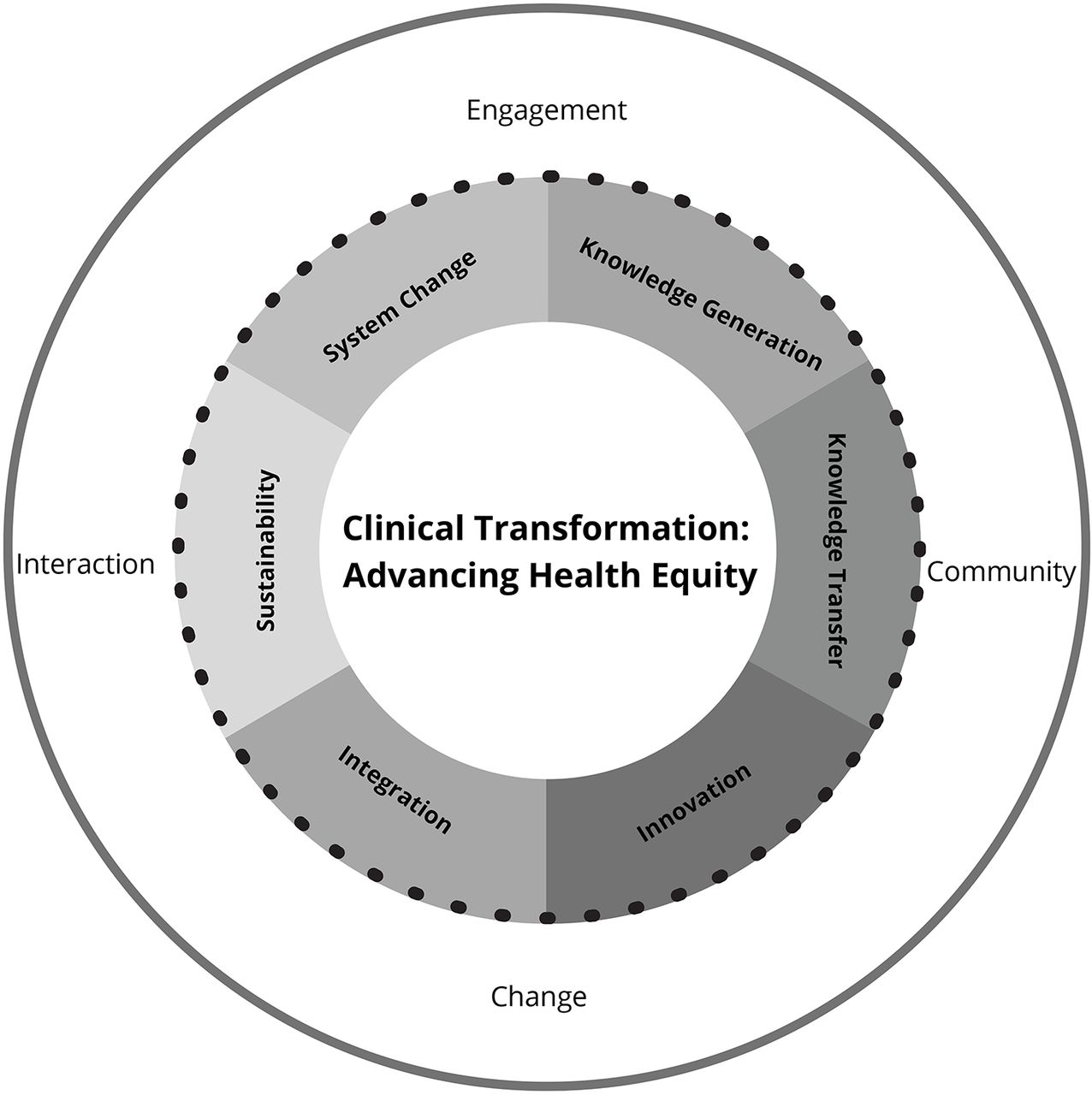
We have identified 7 developmental steps to carry out CoP practice, which are schematically depicted in Figure 1. These steps were created to measure the maturity of communities of practice (the practice) and transform primary care educational curriculum and clinical practice. Individual and group value was created through member participation and personal commitment.32 The 7 CoP development steps50 are: (1) knowledge generation (using evidence-based research in medical education); (2) knowledge transfer (sharing through disseminations, such as publications in peer-reviewed journals, public policy briefs, presentations in conferences, and webinars); (3) innovations (philosophical shift: from basic science foundation to clinical science foundational teaching; from disease-focused to patient-centered care; fee-for-services to value-based pricing); (4) integration (interprofessional health care team); (5) systems change (care coordination, cost reduction, quality improvement/continuous quality improvement/rapid cycle quality improvement, including Plan, Do, Study, Act [PDSA]); (6) curriculum transformation (curriculum changes, use of the electronic health record for clinical decision making); and (7) sustainability (integrated foundational courses and rotations in medical education; understanding and implementing culturally and linguistically appropriate health services to advance health equity). By applying a CoP model as a strategic approach, our national center used the CoP to make curricular transformation recommendations for addressing the needs of each of 3 vulnerable populations regarding a specific health topic. This process recognized that current health topics vary across communities and of the importance of being able to tailor the medical education curriculum to address the local needs of socially vulnerable populations.

The developmental steps in the communities of practice created by the NCMEDR.
NCMEDR = National Center for Medical Education Development and Research
Reprinted with permission from Brown KYB, Ramesh A, Juarez PD, Matthews-Juarez P. Innovation in medical education: a communities of practice approach. In: Interprofessional Education and Collaborative Practice: International Approaches at Micro, Meso, and Macro Levels. Joosten-Hagye D and Khalili H, eds. Cognella Academic Publishing; 2022:244-253.
Value-Creation Participation
Monitoring practice success with metrics increased the value created by the center. Metrics included participation, creation of a research action plan that identified benefits for CoP members, reports of CoP activities and events, and managing CoP activities. The CoP provided an opportunity to engage cross-sectional and diverse groups of more than 600 academic and community stakeholders who shared their perspectives on what medical schools must do to train the next generation of students to provide high-quality, patient-centered care to socially vulnerable populations. Additionally, the CoP provided a platform to discuss the curricular and clinical transformations required to train medical students to effectively address the needs of socially vulnerable populations. At each CoP annual conference, content experts and keynote speakers were invited, including Etienne Beverly Wenger-Trayner.
Outcomes/Lessons Learned
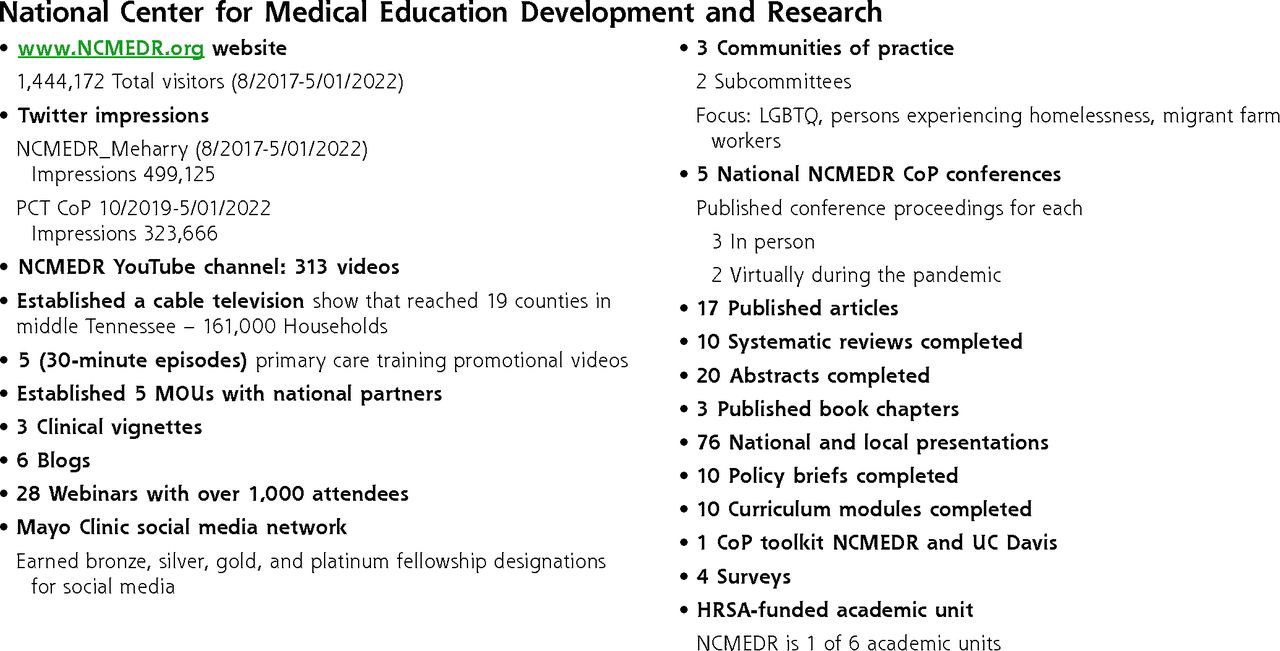
Employment of a CoP enabled the NCMDR to achieve its aims to: identify evidence-based best practices; conduct systematic reviews and surveys; translate research findings into primary care training, practice, and policy recommendations; and disseminate information about best practices in medical and clinical transformation to academic, clinical, and lay audiences. NCMEDR outcomes of the center are presented in Figure 2. The impact of our CoP was shared during the debriefings at each conference. The successes of the NCMEDR can be attributed to the work of the CoP.

Outcomes of the NCMEDR research activities on vulnerable populations.
CoP = communities of practice; HRSA = Health Resources and Service Administration; LGBTQ = lesbian, gay, bisexual, transgender, and queer/questioning; MOU = memorandum of understanding; NCMEDR = National Center for Medical Education Development and Research; PCT = primary care training; UC = University of California.
Project outputs included: community stakeholders who were current or past patients participated in the development of 4 clinic-based LGBTQ educational vignettes that supported problem-based learning that used real-life stories of both patients and experiences of CoP members, including persons who had experienced homelessness and others who identified as LGBTQ. Facilitated discussions of medical students using clinic-based LGBTQ educational vignettes were recommended by the CoP to incorporate into medical education curriculum. Vignettes were integrated into the training of medical students and have been presented at our annual CoP conferences and at national conferences (AAMC, National Healthcare for the Homeless Council).
More recently, the NCMEDR has worked with the Schools of Medicine and Dentistry to integrate project outputs into their respective curricula which has transformed the delivery of high-quality patient-centered care in Meharry clinics, and led to savings in health care costs and improved health outcomes.51-55 We are working with the Schools of Medicine and Dentistry to integrate other curricular models within the comprehensive Patient-Centered Medical Home (PCMH) training program that will directly impact 420 medical students, 200 dental students, and 72 residents (18 family medicine/45 medicine/9 general practice). The CoPs impact on curriculum transformation and clinical care has been very effective in promoting optimal health56,57 and ensuring the needs of socially vulnerable populations are addressed.58
CONCLUSION
The NCMEDR CoP provided an effective strategy for engaging academic and community partners in a review and transformation of current medical school practice with recommendations for curriculum and clinical transformation. CoP offers a knowledge management process for ensuring that medical school curriculum keeps pace with the rapid changes we are witnessing in health care. It has important implications for providing quality care, finding innovative ways to deliver care, and achieving health equity for socially vulnerable populations.
Acknowledgments
We are thankful to our CoP members for their proactive participation in our meetings and offering constructive criticism.
Footnotes
Conflicts of interest: authors report none.
Funding support: This work was funded by the US Department of Health and Human Services (HHS), Health Resources and Services Administration (HRSA) under cooperative agreement UH1HP30348.
Disclaimer: The contents are those of the author(s) and do not necessarily represent the official views of, nor an endorsement, by HRSA, HHS or the US Government.
- Received for publication May 28, 2022.
- Revision received October 19, 2022.
- Accepted for publication October 27, 2022.
- © 2023 Annals of Family Medicine, Inc.




{kind=link}
{kind=link}