
Article Figures & Data
Figures
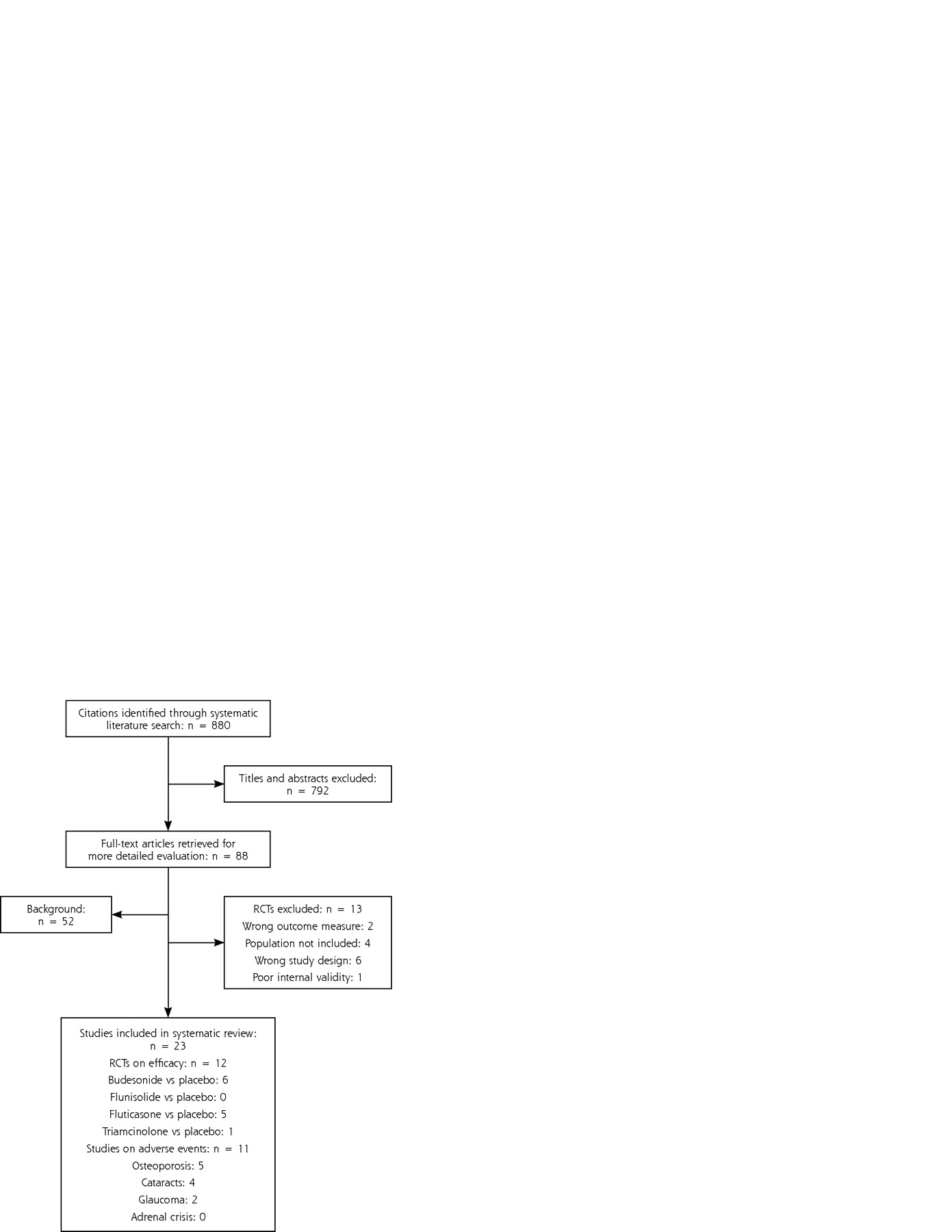
- Figure 1.
Results of literature search.
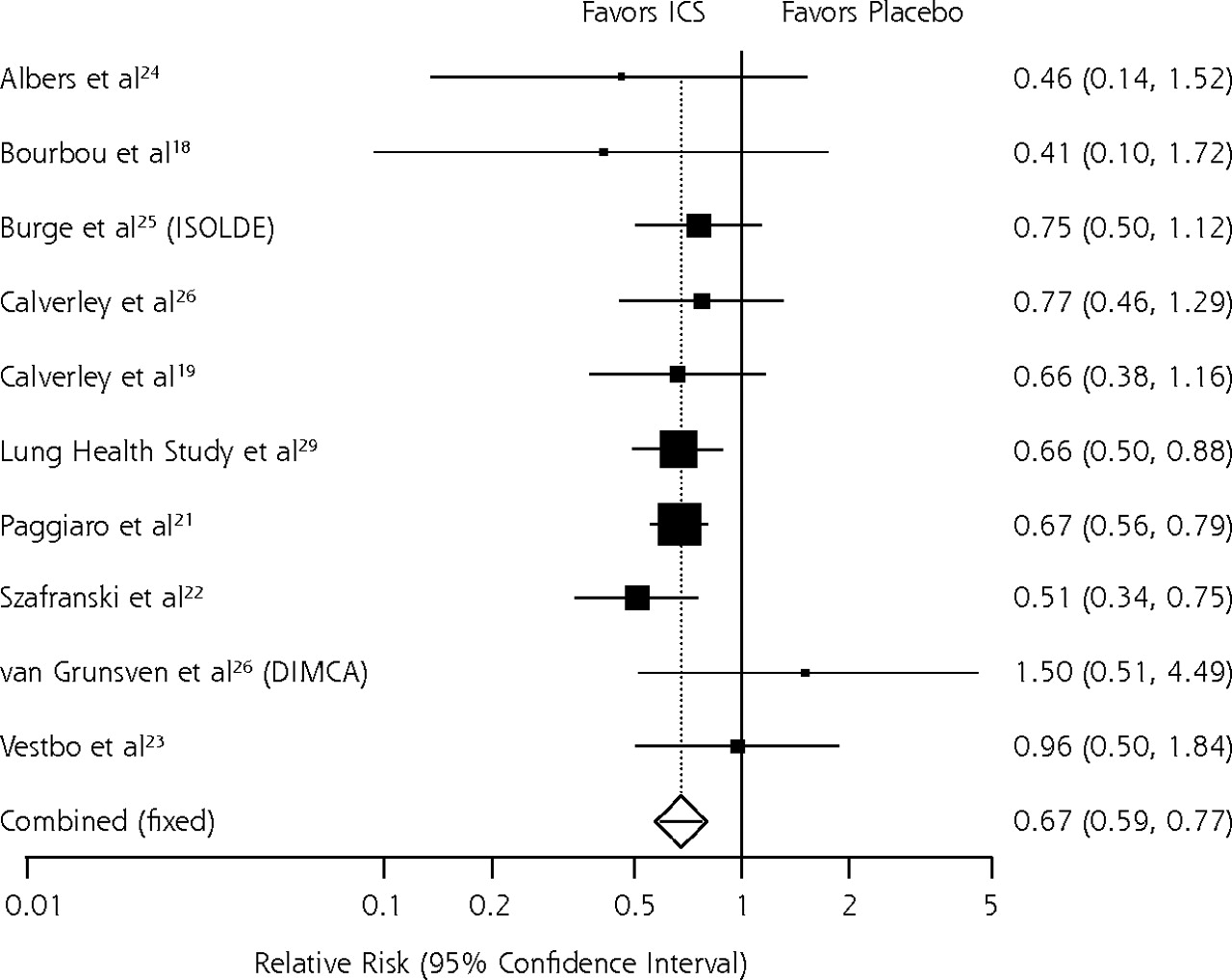
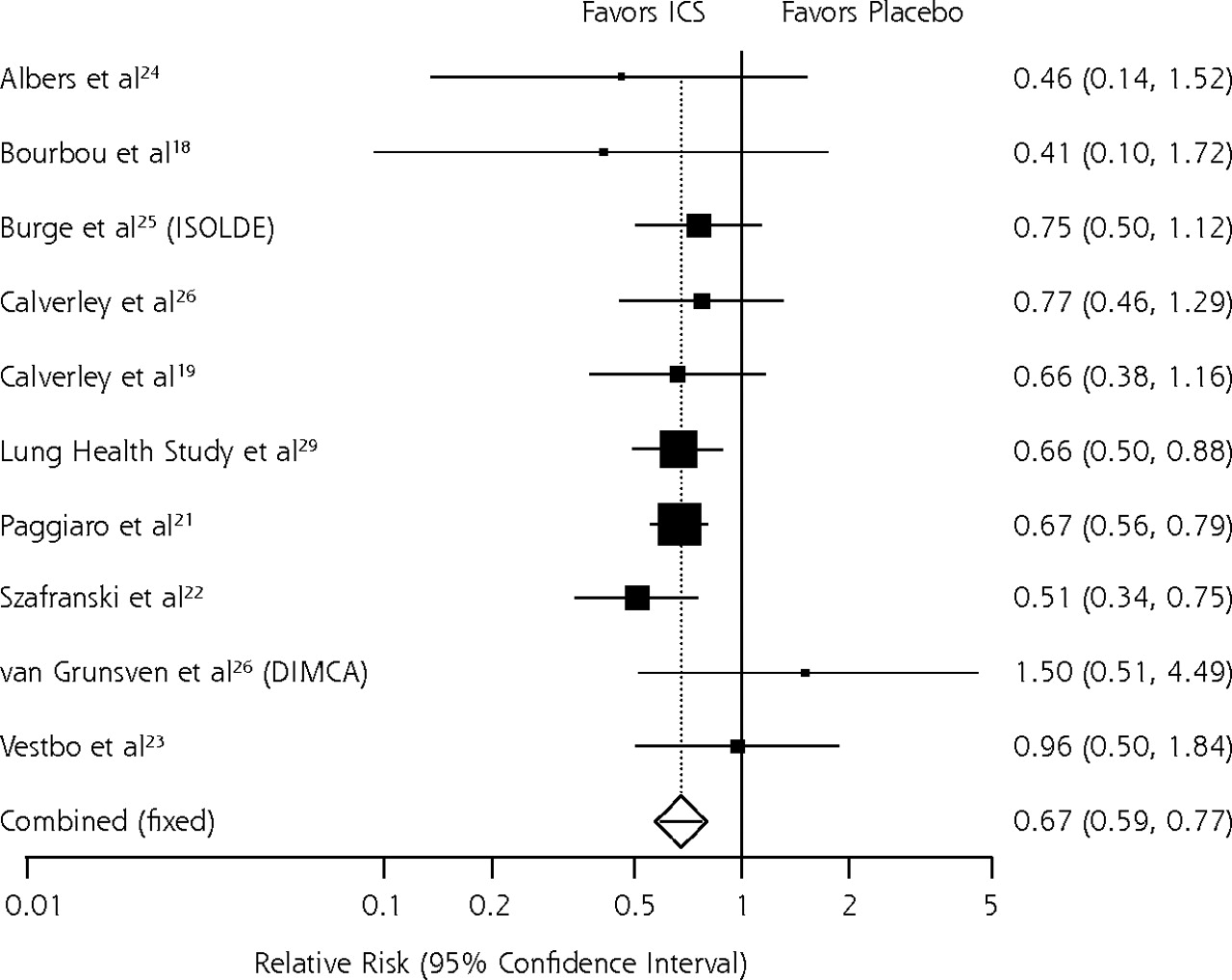
- Figure 2.
Relative risk meta-analysis of effects of inhaled corticosteroids on exacerbations.
COPD = chronic obstructive pulmonary disease; DPI = dry powder inhaler; MDI = metered dose inhaler.
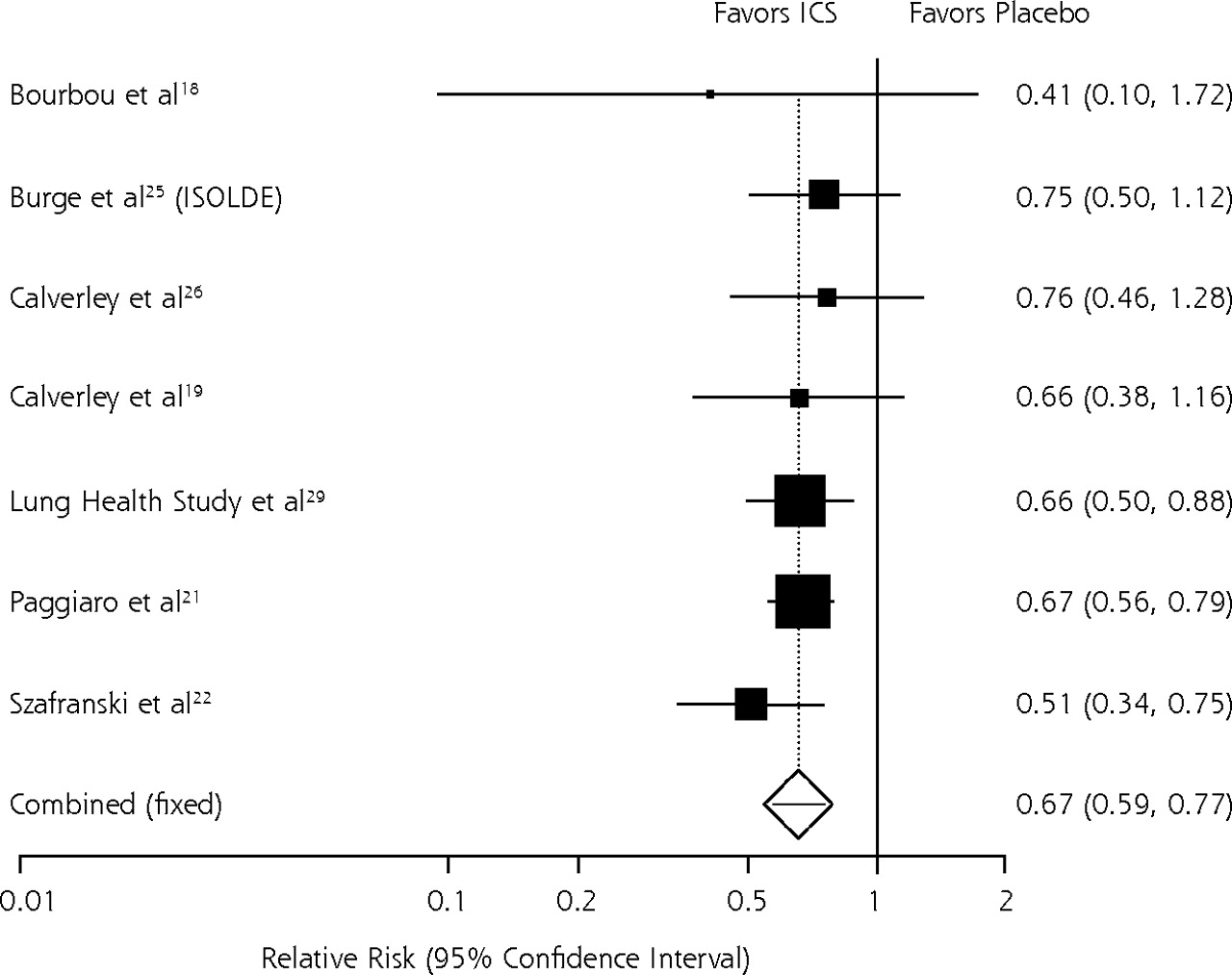
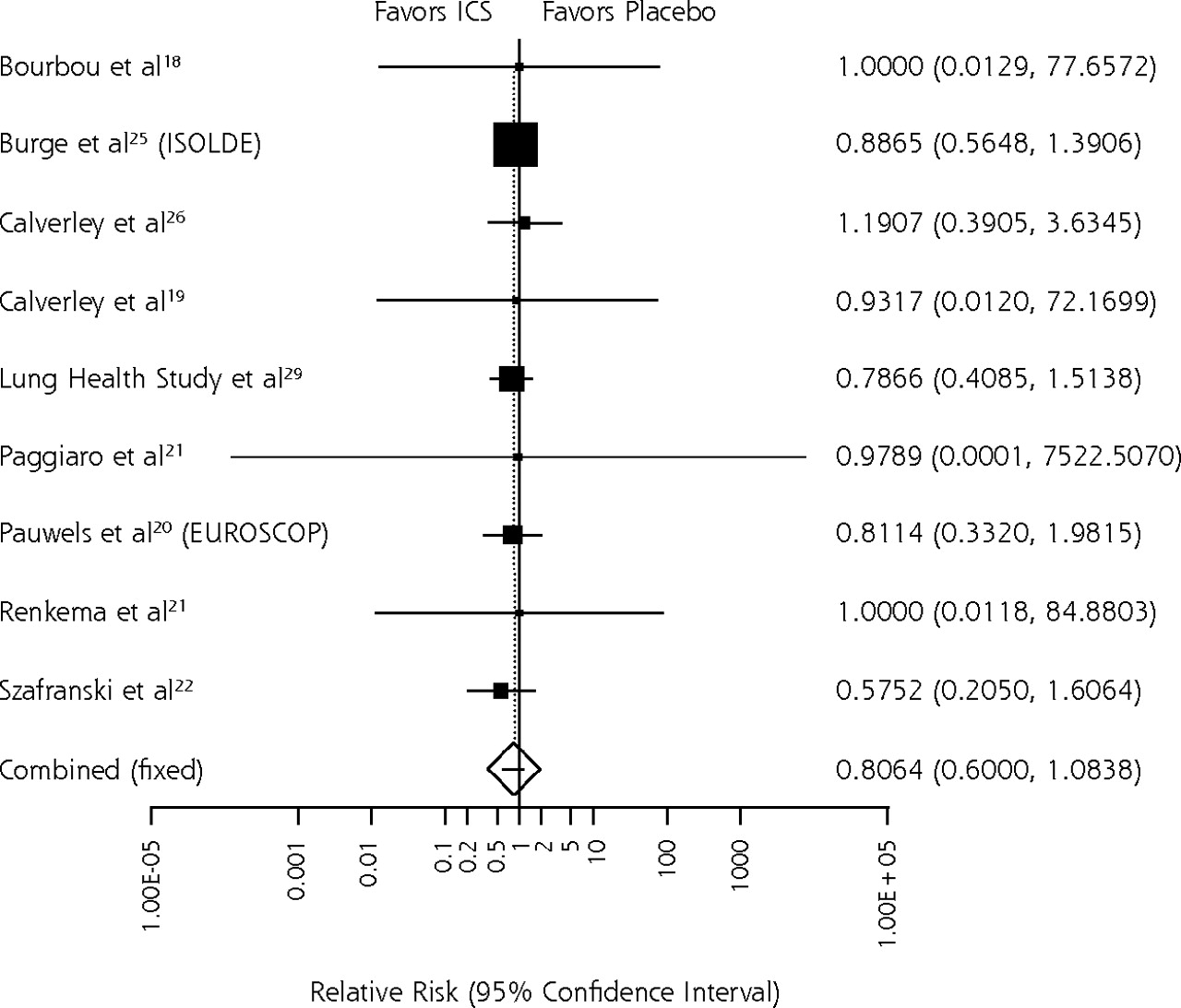
- Figure 3.
Relative risk meta-analysis of effects of inhaled corticosteroids: all-cause mortality.
ICS = inhaled corticosteroid; COPD = chronic obstructive pulmonary disease.



Tables
- Table 1.
Inhaled Corticosteroid Trade Names, Manufacturers, Formulations, and Labeled Uses
Generic Name US Trade Name Manufacturer Dosage Form, Device Strength Labeled Uses MDI = metered dose inhaler; HFA = hydrofluoroalkane propellant; DPI = dry powder inhaler. * Currently not available from the manufacturer. † Contains chlorofluorocarbons. ‡ Not available in the United States. § Discontinued by manufacturer; supplies should be depleted by end of first quarter 2005, at which time Flovent HFA will replace Flovent. Beclomethasone dipropionate QVAR Ivax /3M MDI (HFA) 40 μg/puff 80 μg /puff Asthma (aged ≥5 y) Maintenance Systemic corticosteroid reduction Vanceril* Schering-Plough MDI† 42 μg /puff 84 μg /puff Asthma (aged ≥5 y) Maintenance Systemic corticosteroid reduction Budesonide Pulmicort Turbuhaler AstraZeneca DPI 200 μg/dose Asthma (aged ≥6 y) Maintenance Systemic corticosteroid reduction Pulmicort Respules AstraZeneca Inhalation suspension 500 μg 1,000 μg 2,000 μg Asthma (aged 1–8 y) Flunisolide AeroBidAeroBid-M Forest /3M MDI† MDI-menthol† 250 μg/puff Asthma (aged ≥6 y) Maintenance Systemic corticosteroid reduction Bronalide‡ Boehringer Ingelheim (Canada) MDI† 250 μg/puff Asthma (aged ≥6 y) Maintenance Systemic corticosteroid reduction Fluticasone propionate Flovent GlaxoSmith-Kline MDI† 44 μg/puff 110 μg/puff 220 μg/puff Asthma (aged ≥12 y) Maintenance Systemic corticosteroid reduction Flovent§ Rotadisk GlaxoSmith-Kline DPI – blister pack for use in diskhaler 50 μg/dose 100 μg/dose 250 μg/dose Asthma (aged ≥4 y) Maintenance Systemic corticosteroid reduction Flovent Diskus* GlaxoSmithKline DPI – breath-activated inhalation device 50 μg/dose 100 μg/dose 250 μg/dose Asthma (aged ≥4 y) Maintenance Systemic corticosteroid reduction Mometasone furoate Asmanex Twisthaler Schering-Plough DPI 220 μg/dose Asthma (aged ≥12 y) Maintenance Systemic corticosteroid reduction Triamcinolone acetonide Azmacort Aventis MDI† – with spacer mouthpiece 100 μg/dose Asthma (aged ≥6 y) Maintenance Systemic corticosteroid reduction - Table 2.
Summary of Included Randomized Controlled Trials on Efficacy of Inhaled Corticosteroids in COPD
Author, Year Mean Age (years) No. Duration Dosage, Device Mean Baseline FEV1 (% of predicted) Quality Rating COPD = chronic obstructive pulmonary disease; DPI = dry powder inhaler; MDI = metered dose inhaler. Budesonide vs placebo Bourbeau et al,18 1998 66 79 6 mo 1,600 μg/d, DPI 36.5 Fair Calverley et al,19 2003 64 513 1 y 800 μg/d, DPI 36 Fair Pauwels et al,20 1999 (EUROSCOP) 52 1,277 3 y 800 μg/d, DPI 77 Fair Renkema et al,21 1996 55 40 2 y 1,600 μg/d, MDI 64 Fair Szafranski et al,22 2003 64 403 1 y 800 μg/d, MDI 36 Fair Vestbo et al,23 1999 59 290 3 y 1,200 μg/d, DPI 86 Fair Fluticasone vs placebo Albers et al,24 2004 50 85 2 y 500 μg/d, MDI 90 Good Burge et al,25 2000 (ISOLDE) 64 751 3 y 1,000 μg/d, MDI 50 Fair Calverley et al,26 2003 63 735 1 y 1,000 μg/d, DPI 45 Good Paggiaro et al,27 1998 63 281 6 mo 1,000 μg/d, MDI 57 Good van Grunsven et al,28 2003 47 48 2 y 500 μg/d, DPI 96 Fair Triamcinolone vs placebo Lung Health Study29 56 1,116 3 y, 4 mo 1,200 μg/d, MDI 64 Fair Author, Year N Design Population Results Quality Rating COPD = chronic obstructive pulmonary disease; NA = not applicable; BDP = beclomethasone dipropionate; BMD – bone mineral density; ICS = inhaled corticosteroid; RCT = randomized controlled trial; BUD = budesonide; PSC = posterior subcapsular cataracts; RAMQ = regi de l’assurance maladie du Quebec database; GPRD = general practice research database; IOP = intraocular pressure. Bone density and osteoporotic fractures Jones et al,30 2004 NA Systematic review Asthma and COPD No difference in BMD and osteoporotic fractures between ICS and placebo Fair Hubbard et al,31 2002 16,341 Case-control Asthma and COPD Nonspecific ICS use associated with a small increase in the risk of hip fracture Good Israel et al,32 2001 109 Prospective cohort Women (aged 18–45 y) Triamcinolone associated with dose- related decline in BMD (total hip and trochanter) of 0.00044 g/cm2 per puff/year Fair Johnell et al,33 2002 1,277 RCT COPD No difference in bone density between BUD and placebo over 3 y; no difference in bone density or vertebral fractures in subgroup of 912 smokers Fair Lee & Weiss,34 2004 8,525 Nested case-control COPD Nonspecific ICS use associated with increased risk of fractures at high doses Good Posterior subcapsular cataracts Cumming et al,35 1997 3,654 Cross-sectional Adults; asthma and COPD; aged 49–97 y Increased risk of nuclear and PSC among ICS users N/A Garbe et al,36 1998 25,545 Case-control RAMQ; asthma and COPD; aged ≥70 y Increased risk of cataract extraction for ICS users only at high dose and duration Good Jick et al,37 2001 201,816 (3,581) Cohort + case-control GPRD; asthma and COPD; aged 3–90 y Dose-, duration-, and age-related increased risk of cataracts among ICS users; no increase in risk for age <40 Good Smeeth et al,38 2003 30,958 Case-control GPRD; asthma and COPD; aged ≥40 y Dose- and duration-related increased risk of cataracts among ICS users Good Ocular hypertension and open-angle glaucoma Garbe et al,39 1997 48,118 Case-control RAMQ aged ≥66 y ≥3 mo high-dose ICS associated with increased risk of open-angle glaucoma and ocular hypertension Fair Mitchell et al,40 1999 3,654 Cross-sectional Adults; asthma and COPD; aged 49–97 y Dose-related increased risk of elevated IOP and open-angle glaucoma for ICS users with glaucoma family history N/A
The Article in Brief
Efficacy and Safety of Inhaled Corticosteroids in Patients With COPD: A Systematic Review and Meta-Analysis of Health Outcomes
Gerald Gartlehener, MD, MPH, and colleagues
Background Chronic obstructive pulmonary disease (COPD) is a leading causes of illness and death worldwide. Caused primarily by smoking, COPD refers to a group of lung diseases in which airflow to and within the lungs becomes partially blocked, making it hard to breathe. This study examines existing research to determine the risks and benefits of inhaled corticosteroids in treating COPD.
What This Study Found Inhaled corticosteroids appear to help patients with moderate to severe COPD. Patients treated with inhaled corticosteroids experienced 33 percent fewer exacerbations (a sudden worsening of COPD symptoms) than patients who received a placebo. Inhaled corticosteroids do not appear to benefit patients with mild COPD.
Implications
- This study is the first comprehensive assessment of the risks and benefits of treating COPD with inhaled corticosteroids. The findings contribute information to the ongoing controversy about the use of inhaled corticosteroids in treatment of patients with COPD.




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Inhalation devices and inhaled corticosteroids particle size influence on severe pneumonia in patients with chronic obstructive pulmonary disease: a nationwide cohort study
- Inhaled corticosteroids and the risk of lung cancer in COPD: a population-based cohort study
- Where current pharmacological therapies fall short in COPD: symptom control is not enough
- Statin use is associated with reduced mortality in COPD
- On TRACK: Medical Research Must Consider Context and Complexity
- In This Issue: Communication in the Era of 'Personalized' Medicine