
Article Figures & Data
Figures
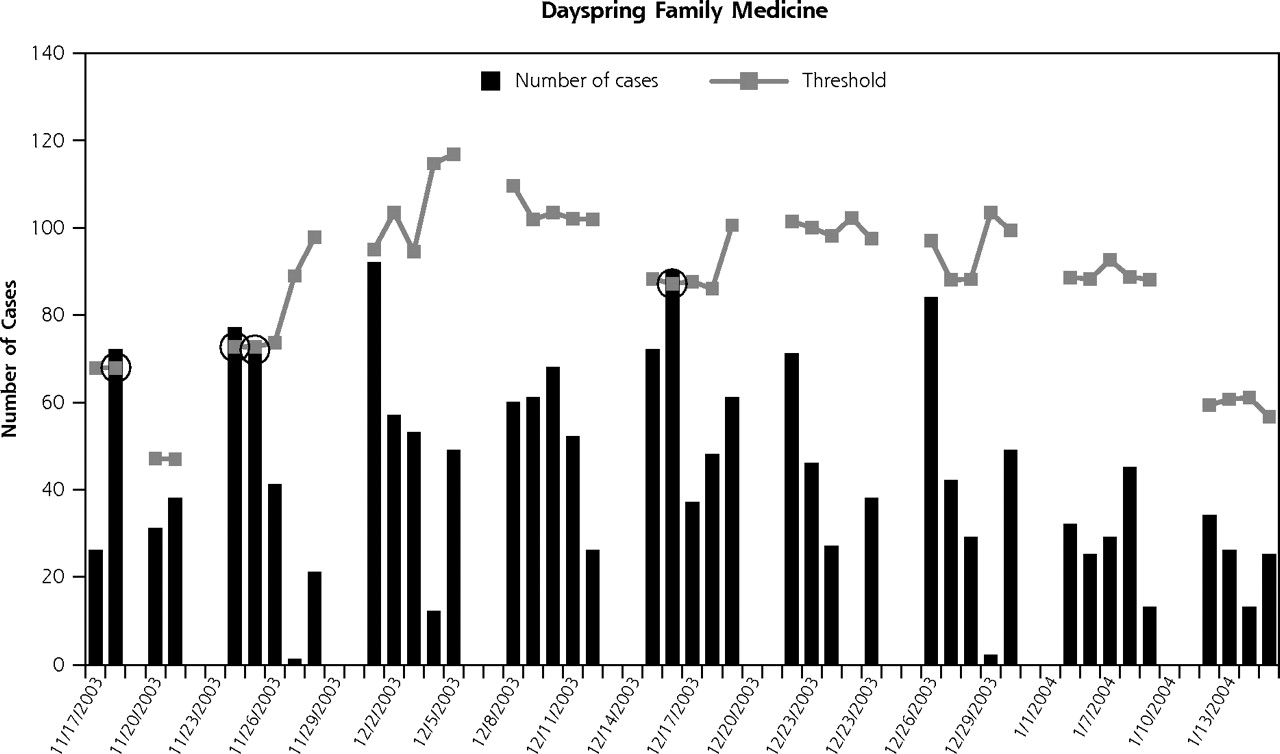
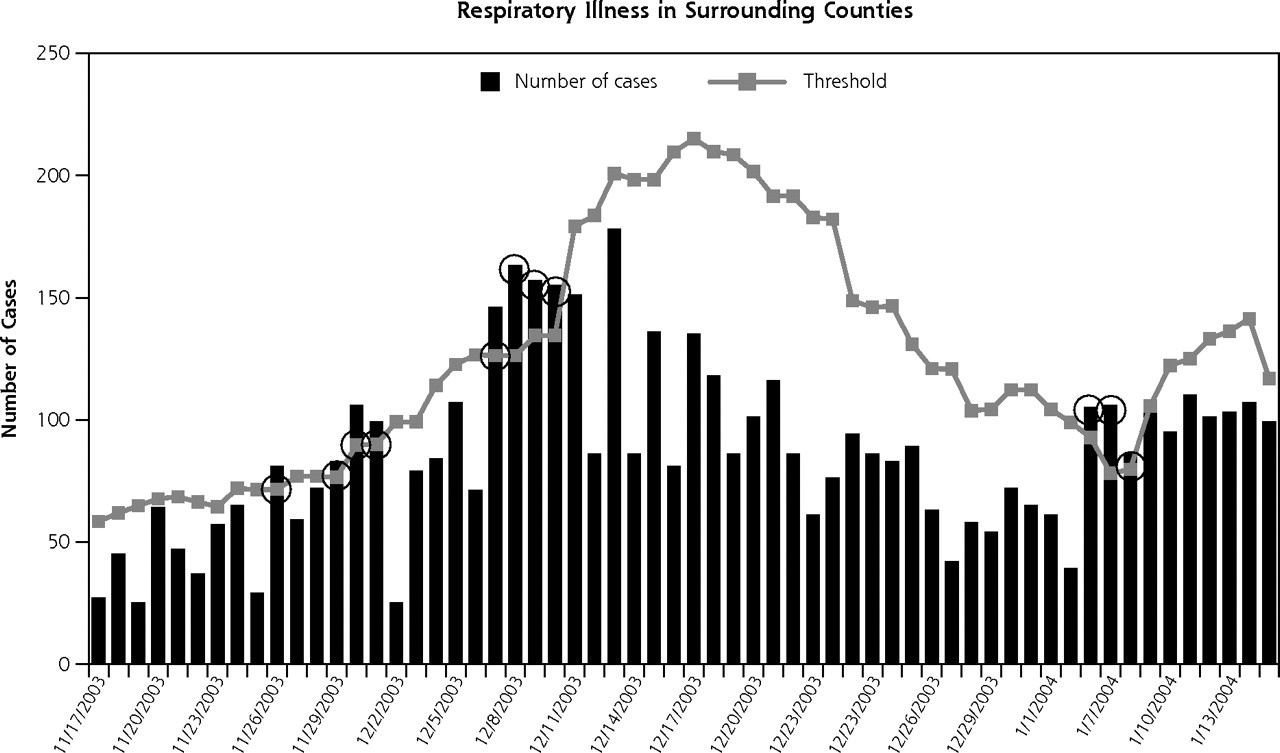
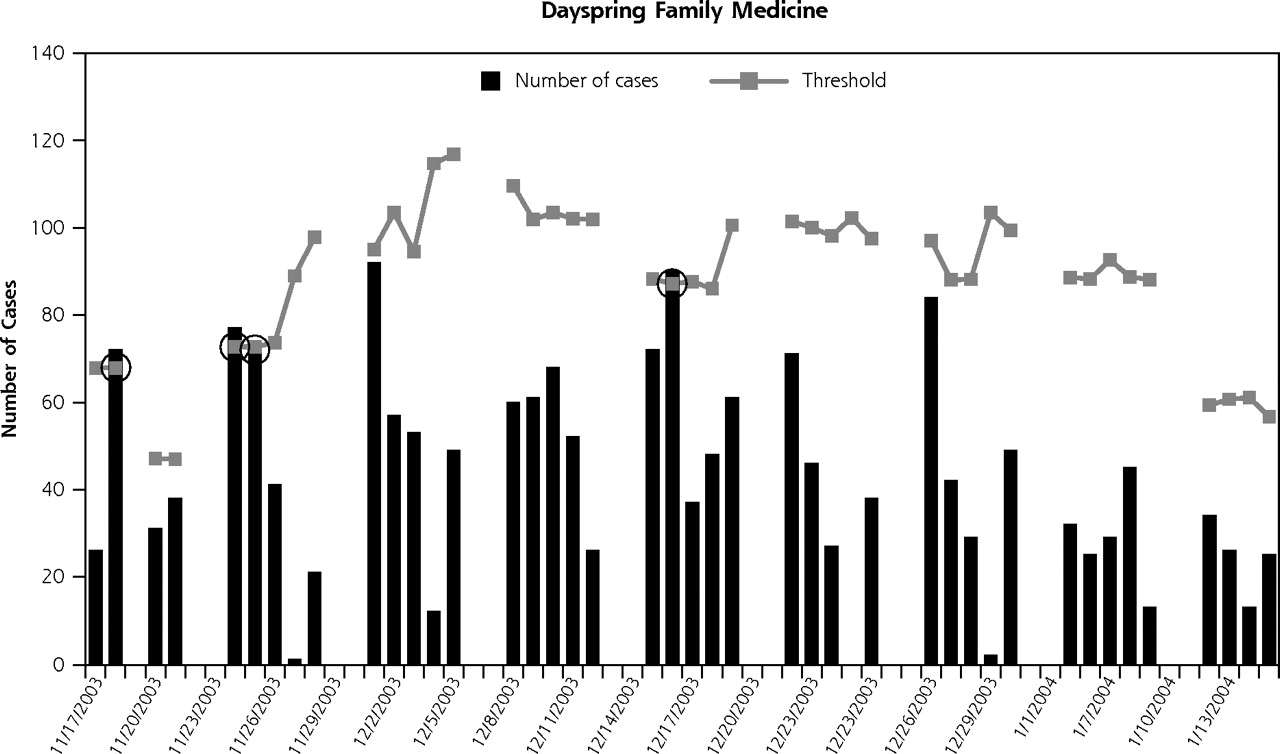
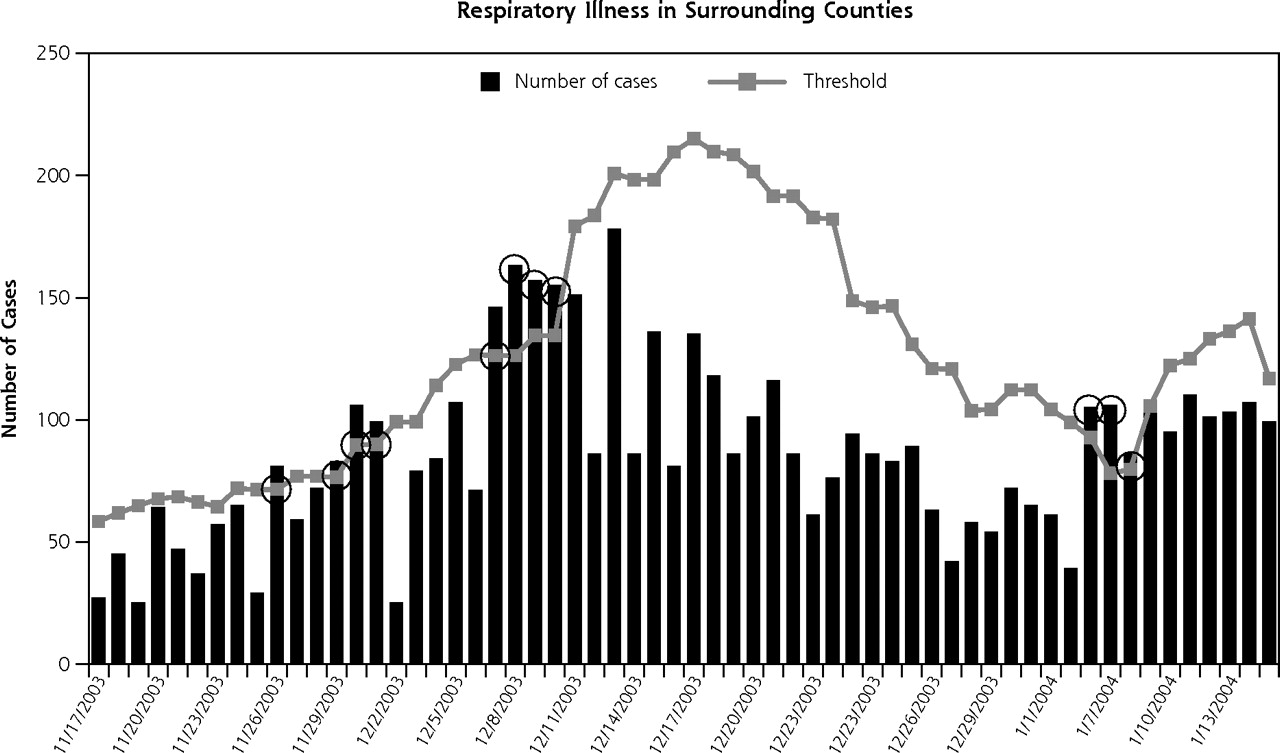
- Figure 1.
Daily number of respiratory syndrome codes reported by Dayspring Family Medicine and by emergency departments in the 6 surrounding counties, 15 November 2003 through 15 January 2004.
Note: Circles represent days when the surveillance threshold of 2 SD was exceeded.
- Figure 2.
Flow chart of proposed primary-care–based syndromic surveillance system.
ICD-9 = International Classification of Diseases, Ninth Revision.

Tables
Syndrome Definition ICD-9 codes CDC = Centers for Disease Control and Prevention; ICD-9 = International Classification of Diseases, Ninth Revision. Note: CDC Web link with syndrome definitions: http://www.bt.cdc.gov/surveillance/syndromedef/index.asp. Botulism-like Paralytic conditions consistent with botulism; or other symptoms consistent with botulism: diplopia, dry mouth, dysphagia, difficulty focusing to a near point 005.1, 344.04, 344.09,344.2, 344.89,344.9, 351.9,352.6, 352.9,357.0, 368.2,374.30, 378.51,378.52, 378.53,378.54, 378.55 Hemorrhagic illness Specific diagnosis of any virus that causes viral hemorrhagic fever (VHF), such as yellow fever, Lassa, or Ebola; or any acute condition with multiple organ involvement or acute blood abnormalities that may be consistent with exposure to a virus that causes VHF 287.1, 287.2, 287.8, 287.9, 511.8, 790.01, 790.92 Lymphadenitis Acute regional lymph node swelling and/or infection (painful bubo), particularly in groin, axilla, or neck 020.0, 021.0, 021.3, 075, 289.3, 683, 785.6 Localized cutaneous lesion Cutaneous lesion, ulcer, or localized edema consistent with cutaneous anthrax or tularemia. 020.0, 020.1, 021.0, 022.0, 680.0, 680.1, 680.2, 680.3, 680.4, 680.5, 680.6, 680.7, 680.8, 707.11, 707.12, 707.13, 707.14, 707.19 Gastrointestinal Acute upper and/or lower gastrointestinal (GI) tract infection; or acute nonspecific symptoms of GI distress such as nausea, vomiting, or diarrhea 005.89, 005.9, 008.49, 008.5, 008.69, 008.8, 009.0, 009.1, 009.2, 009.3, 022.2, 078.82, 535.00, 535.01, 535.40, 535.41, 535.50, 535.51, 535.60, 535.61, 536.2, 555.0, 555.1, 555.2, 558.2, 558.9, 569.9, 787.01, 787.02, 787.03, 787.3, 787.91 Respiratory Specific diagnosis of any acute infection of the upper and/or lower respiratory tract; or acute nonspecific diagnosis or symptoms of respiratory tract infection 020.3, 020.4, 020.5, 021.2, 022.1, 460, 462, 463, 464.00, 464.01, 464.10, 464.11, 464.20, 464.21, 464.30, 464.31, 464.4, 464.50, 464.51, 465.0, 465.8, 465.9, 466.0, 466.11, 466.19, 478.9, 480.8, 480.9, 482.9, 483.8, 484.5, 484.8, 485, 486, 490, 511.0, 511.1, 511.8, 513.0, 513.1, 518.4, 518.84, 519.2, 519.3, 769, 786.00, 786.06, 786.1, 786.2, 786.3, 786.52, 799.1 Neurological Acute infection of the central nervous system (CNS) with a specific diagnosis, such as pneumococcal meningitis; or acute nonspecific symptoms of CNS infection 047.8, 047.9, 048, 049.0, 049.9, 320.9, 321.2, 322.0, 322.1, 322.9, 323.8, 323.9, 348.3, 781.6 Rash Acute condition having signs or symptoms consistent with smallpox; specific diagnosis of acute infectious rash (eg, chicken pox); or nonspecific infectious rash. Excludes noninfectious skin rashes, such as eczema, seborrheic dermatitis, and contact dermatitis 050.0, 050.1, 050.2, 050.9, 051.0, 051.1, 052.7, 052.8, 052.9, 057.8, 057.9, 695.0, 695.1, 695.2, 695.89, 695.9 Fever Acute febrile illness of unspecified origin 020.2, 020.8, 020.9, 021.8, 021.9, 022.3, 022.8, 022.9, 038.3, 038.40, 038.49, 038.8, 038.9, 079.89, 079.99, 780.31, 780.6, 790.7, 790.8, Severe illness or death potentially due to infectious disease Acute onset of shock or coma from potentially infectious causes 780.01, 785.50, 785.59, 798.1, 798.2, 798.9, 799.9 - Table 2.
Daily Frequency of Syndrome Codes in 1 Family Medicine Practice for 1 Calendar Year (n = 239 days)*
Syndrome Mean (SD) Range * Weekend days and holidays omitted. Botulism-like 0.0 (0.0) 0 Hemorrhagic illness 0.01 (0.09) 0–1 Lymphadenitis 0.63 (0.97) 0–5 Localized cutaneous lesion 0.03 (0.17) 0–1 Gastrointestinal 4.05 (2.97) 0–14 Respiratory 26.73 (15.91) 2–92 Neurological 0.03 (0.23) 0–3 Rash 0.38 (0.74) 0–4 Fever 1.75 (1.89) 0–10 Severe illness or death 0.0 (0.0) 0 Number of codes recorded per day 252.55 (59.36) 56–394 - Table 3.
Frequency and Distribution of Significant Aberrations (Signals) by Threshold Level and Site
Percentage of Days With Significant Aberrations* in the Number of Observed Cases, by Syndrome Threshold for Dayspring Clinic Threshold for Emergency Department, UNC Hospitals Syndrome 2 SD 3 SD 2 SD 3 SD ICD-9 = International Classification of Diseases, Ninth Revision. * A significant aberration (signal) occurs when the number of cases recorded for that day exceeds the statistically determined threshold, based on observed cases from the previous week. Botulism-like 0 0 12.6 6.2 Hemorrhagic illness 0.9 0.9 13.2 6.2 Lymphadenitis 11.3 5.6 7.6 3.7 Cutaneous lesion 3.0 2.6 9.0 5.6 Gastrointestinal 6.1 3.5 8.7 2.8 Respiratory 6.9 2.2 9.0 1.7 Neurological 2.2 2.2 11.8 5.9 Rash 11.3 7.4 10.7 5.1 Fever 11.3 5.6 7.6 3.9 Severe illness/death 0 0 8.7 5.3 Any of the above syndromes 40.0 24.3 63.5 36.5 Average ICD-9 codes per day 244 641
The Article in Brief
Syndromic Surveillance for Emerging Infections in Office Practice Using Billing Data
Philip D. Sloane, MD, MPH, and colleagues
Background Syndromic surveillance is the monitoring of health data to identify possible outbreaks of diseases associated with bioterrorism or pandemic illness. Since patients often visit their primary care doctors when they first become sick, primary care practices could provide timely information, yet there has been little research on syndromic surveillance in primary care settings. This study tested whether it is practical to conduct syndromic surveillance in a primary care office using billing data.
What This Study Found This 1-year study of a primary care practice finds that it is practical to convert billing data into daily summaries of diagnosis codes, which can be used for rapid surveillance of disease patterns in a community. These systems can be easily implemented at a low cost and with minimal effort.
Implications
- Further development of syndromic surveillance systems should include primary care offices.
- This type of surveillance could be used to detect bioterrorism attacks and emerging infections, especially those that are not lethal and resemble common infections.
- Rapid conversion of primary care practices to electronic medical records opens up the possibility of new, potentially low-cost systems for early detection of emerging infectious diseases.




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Clinical Population Medicine: Integrating Clinical Medicine and Population Health in Practice
- Physician surveillance of influenza: Collaboration between primary care and public health
- Observing the Spread of Common Illnesses Through a Community: Using Geographic Information Systems (GIS) for Surveillance
- On TRACK: 'Allows Readers and Authors to Go One Step Further'
- In this Issue: Mixed Methods and Diverse Perspectives