
Article Figures & Data
Figures
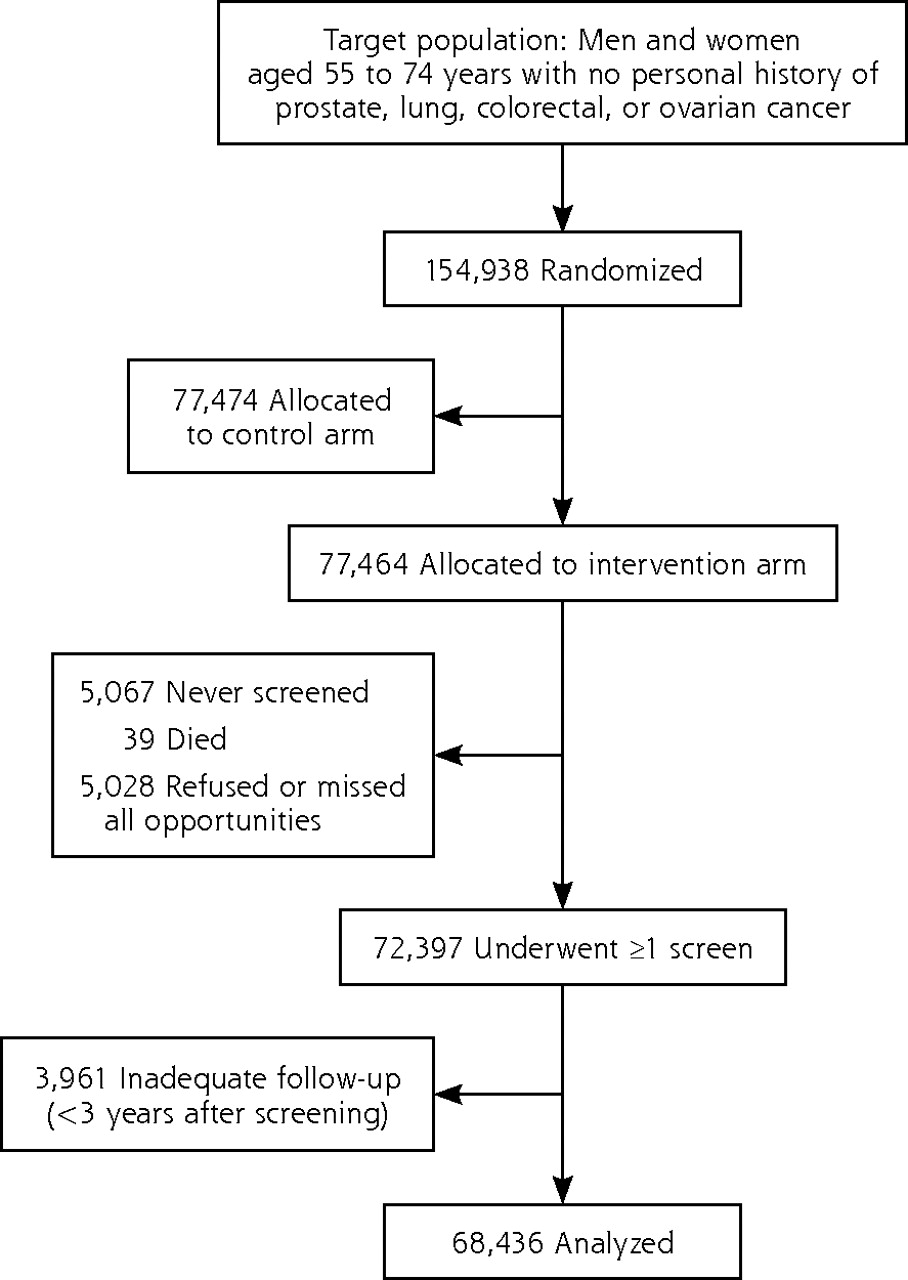
- Figure 1.
Study population selection.
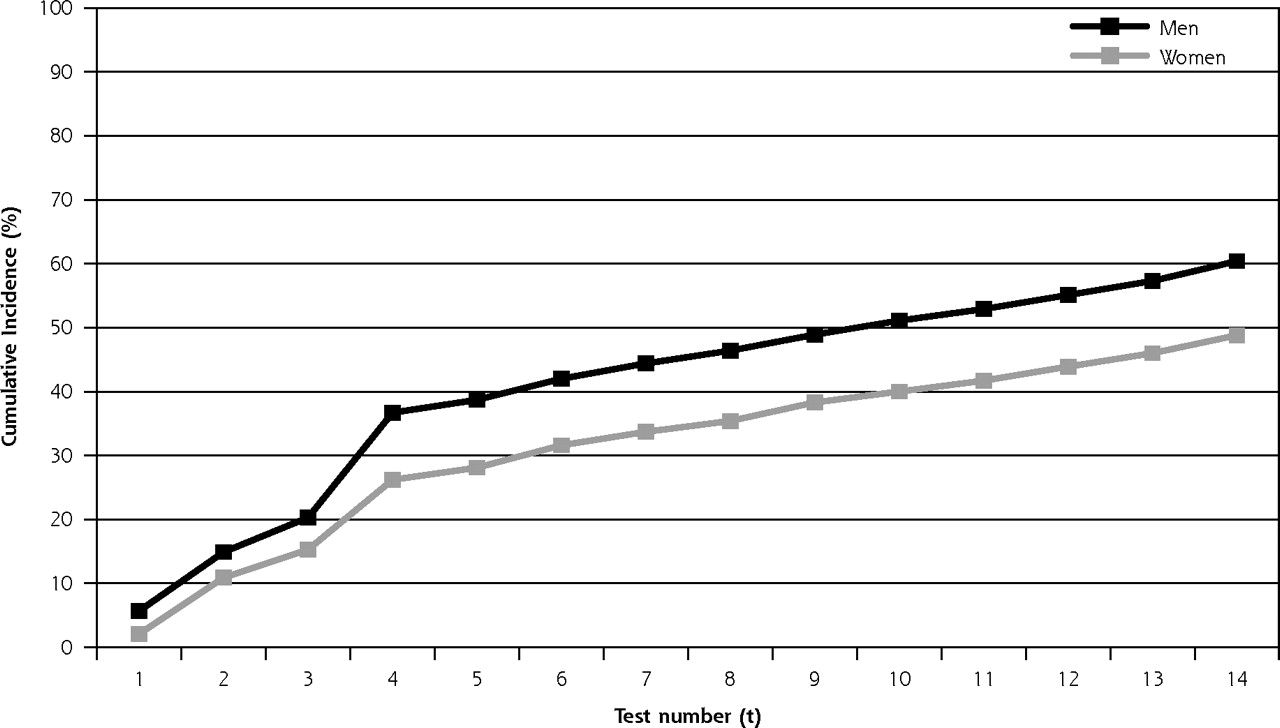
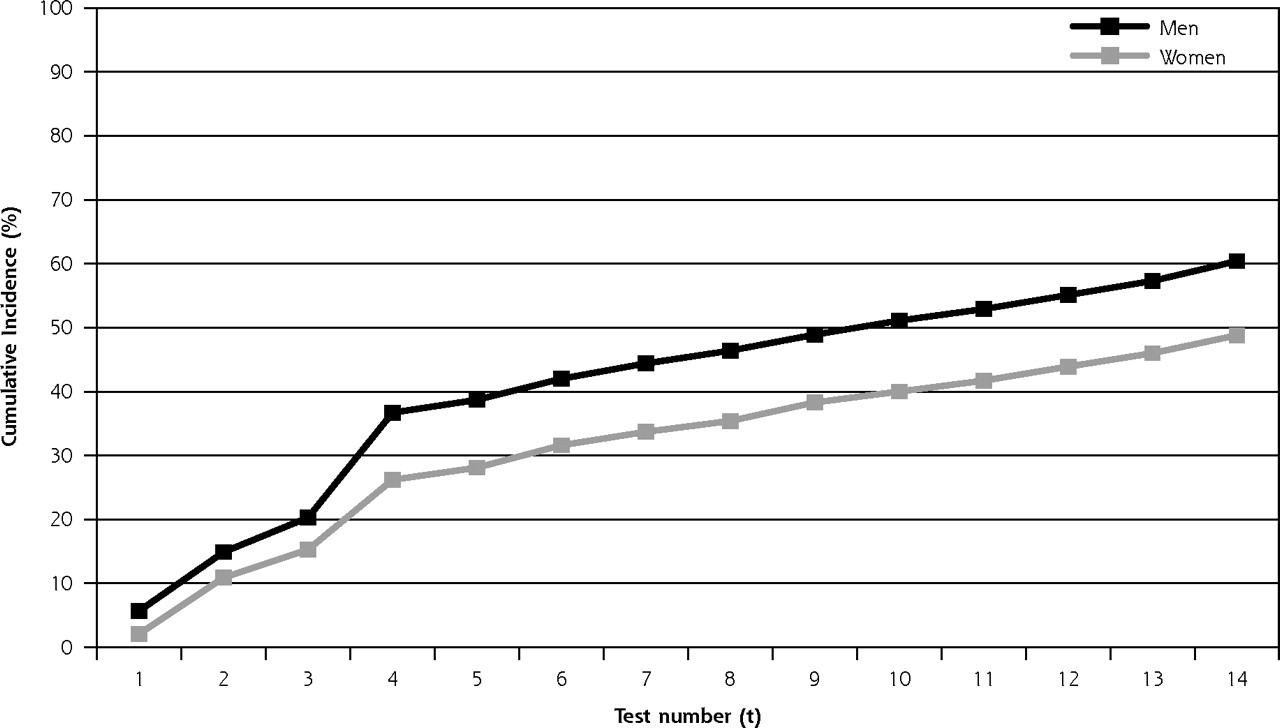
- Figure 2.
Cumulative probability of a false-positive result for a multimodal cancer screening regimen.
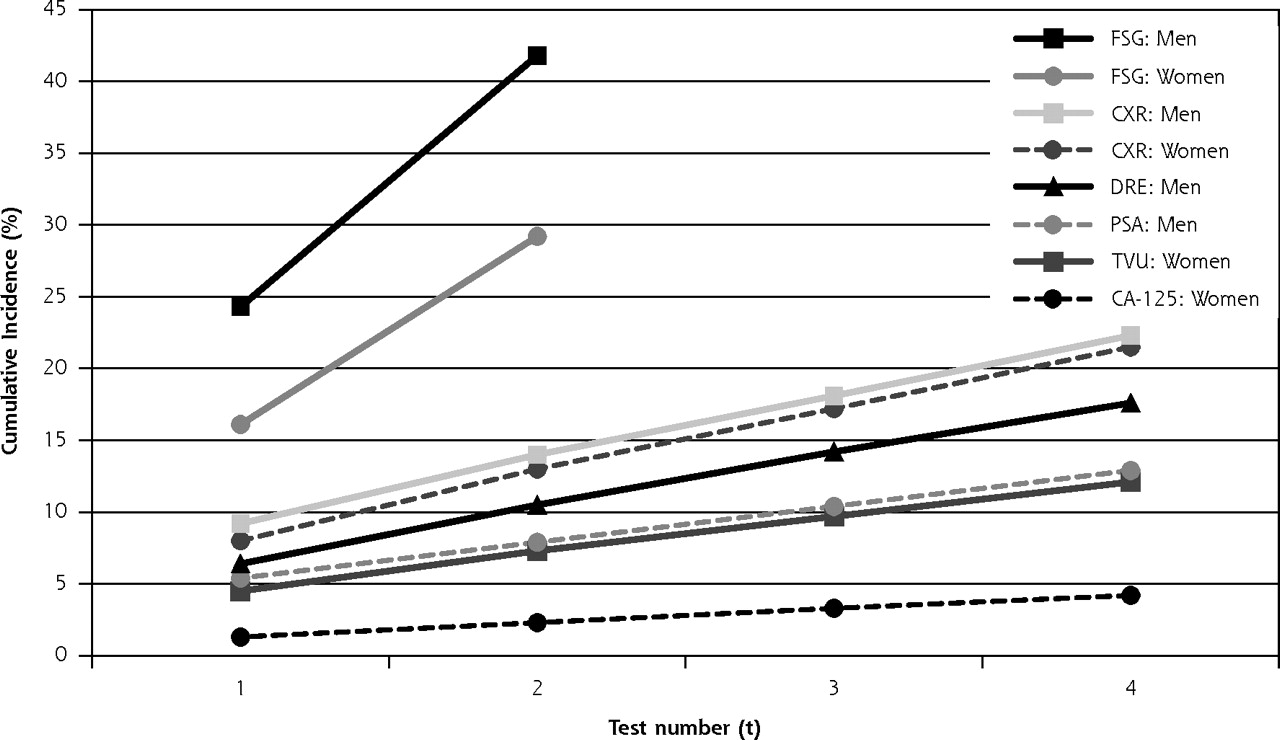
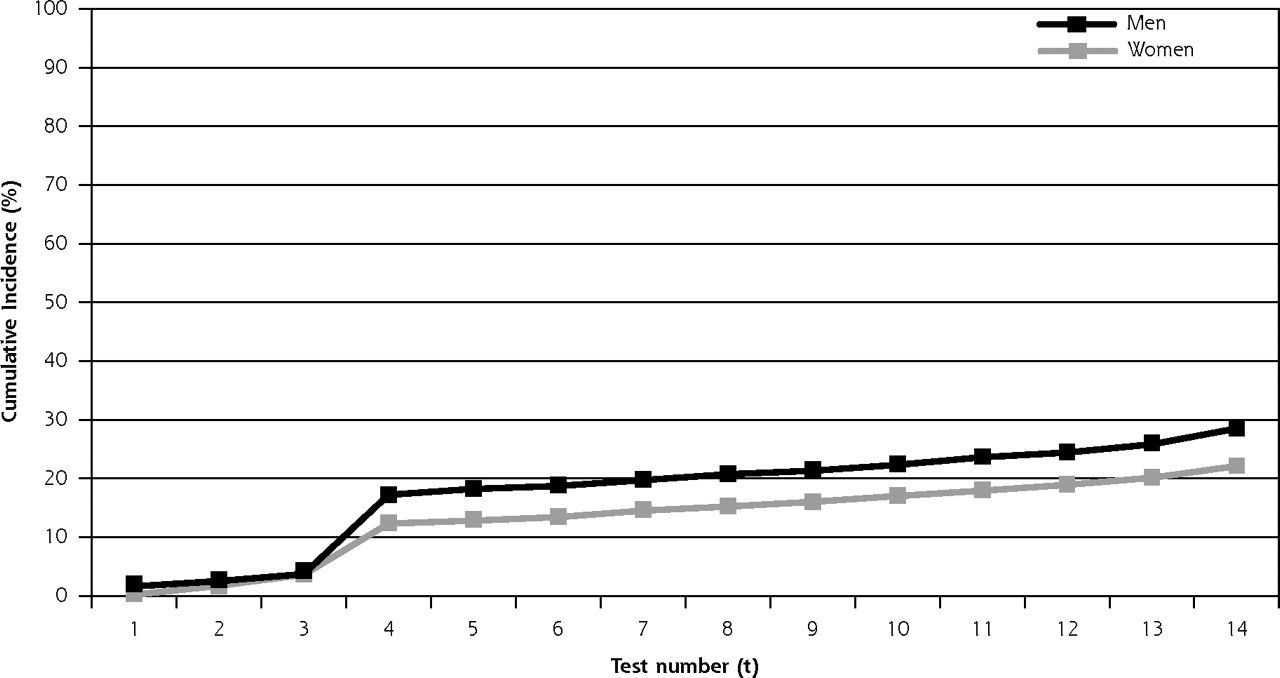
- Figure 3.
Cumulative probability of receiving an invasive diagnostic procedurea as a direct result of a false-positive test in a multimodal cancer screening regimen.




Tables
- Table 1.
Criteria for a Positive Screening Examination and Classification of Diagnostic Follow-Up Procedures
Diagnostic Follow-Up Procedures Screening Modality Definition of a Positive Screening Result Minimally Invasive Procedures Moderately Invasive Procedures Major Surgical Procedures CA-125 = cancer antigen 125; CXR = chest radiograph; DRE = digital rectal examination; FSG = flexible sigmoidoscopy; PSA = prostate-specific antigen; TVU = transvaginal ultrasonography. a Assuming a perfect sphere and using the prolate ellipsoid formula, this volume correlates to an approximate diameter of 2.67 cm. A 10-cc cutoff was chosen, as it corresponds to 2 standard deviations above mean ovarian volume for postmenopausal women.24 b We define a true-positive FSG as both overt cancer and advanced adenomas (lesions with villous histologic findings, severe cellular dysplasia, and/or ≥1 cm in diameter). PSA >4 ng/mL Endoscopy Biopsy Prostatectomy Cystourethroscopy Cystoscopy Cystopanendoscopy Lymphadenectomy Ureterogram Transurethral resection of the prostate (TURP) DRE One or more of the following findings: As for PSA As for PSA As for PSA Nodularity Induration Asymmetry Loss of anatomic landmarks CA-125 >35 U/mL Colonoscopy Biopsy Hysterectomy Culdocentesis Laparotomy Hysteroscopy Omentectomy Intra-abdominal washings Oophorectomy Laparoscopy Ovarian lymphadenectomy (with laparotomy) Paracentesis TVU One or more of the following findings: As for CA-125 As for CA-125 As for CA-125 Ovary or cyst >10 cca Solid area or papillary projection extending into the cavity of a cystic ovarian tumor of any size Mixed (solid/cystic) component within a cystic ovarian tumor CXR One or more of the following findings: Bronchoscopy Biopsy Lung resection Nodule Lymphadenectomy Thoracotomy Mass Mediastinoscopy Hilar or mediastinal lymph node enlargement Thoracoscopy Major atelectasis or lobar collapse Transbronchial aspiration Infiltrate, consolidation, or alveolar opacity Transthoracic aspiration FSG One or more of the following findingsb: Colonoscopy (with- out biopsy) Biopsy Colon resection Rectal nodule(s) Cystoscopy Hemicolectomy Rectal and/or colon mass(es) Endoscopy Lymphadenectomy Laparotomy Colon polyp(s) Rigid sigmoidoscopy False-Positive Result Participants No. (%) 1 18,394 (26.9) 2 6,043 (8.8) 3 2,531 (3.7) 4 1,535 (2.2) 5 642 (0.9) 6 228 (0.3) 7 78 (0.1) 8 53 (0.1) 9 11 (0.0) 10 2 (0.0) 11 0 (0.0) 12 0 (0.0) 13 0 (0.0) 14 0 (0.0) - Table 3.
Initial Entry Round (Year 1) Through Last Entry Round (Year 4) of Screening: False-Positive and Resulting Diagnostic Follow-Up Rates
Physician Response Repeated Screening Imaging Minimally Invasive Procedurea Moderately Invasive Procedureb Major Surgical Procedurec Subgroup Ever False Positive No. (%) No. (%)d % of FPse No. (%)d % of FPse No. (%)d % of FPse No. (%)d % of FPse No. (%)d % of FPse CA-125 = cancer antigen 125; CXR = chest radiograph; DRE = digital rectal examination; FP = false positive; FSG = flexible sigmoidoscopy; PSA = prostate-specific antigen; TVU=transvaginal ultrasonography. Note: These percentages reflect only the subset of diagnostic procedures directly caused by a false-positive result; they do not include procedures associated with a true-positive or negative. a Example: simple endoscopy with conscious sedation (see Table 1 for the complete list of procedure classifications). b Example: tissue removal, more involved instrumentation, or general anesthesia, including laparoscopy. c Example: prostatectomy, or laparotomy with colectomy or oophorectomy. d Percentage among participants in the intervention arm that took at least 1 screening examination. e Percentage among participants in the intervention arm that received at least 1 false-positive examination (change in denominator). This percentage (and the accompanying crude numbers) does not include procedures that resulted in a true positive (diagnosis of cancer). f In each case, the denominator is the total number of participants taking examinations for a given screening modality; this number varied depending on differences in compliance with different tests. Overall rates 29,517 (43.1) 13,576 (19.8) 46.0 7,306 (10.7) 24.8 2,049 (3.0) 6.9 10,822 (15.8) 36.7 1,062 (1.6) 3.6 Men 17,432 (50.9) 9,251 (27.0) 53.1 4,056 (11.9) 23.3 1,088 (3.2) 6.2 6,972 (20.4) 40.0 47 (0.1) 0.3 Women 12,085 (35.3) 4,325 (12.6) 35.8 3,250 (9.5) 26.9 961 (2.8) 8.0 3,850 (11.3) 31.9 1,015 (3.0) 8.4 By screening modality: menf PSA 3,388 (10.4) 2,884 (8.9) 85.1 1,494 (4.6) 44.1 1 (0.0) 0.0 1,491 (4.6) 44.0 6 (0.0) 0.2 DRE 4,882 (15.0) 3,881 (12.0) 79.5 1,326 (4.1) 27.2 0 (0.0) 0.0 1,259 (3.9) 25.8 1 (0.0) 0.0 CXR 6,320 (18.6) 3,216 (9.5) 50.9 1,466 (4.3) 23.2 52 (0.2) 0.8 77 (0.2) 1.2 35 (0.1) 0.6 FSG 8,186 (26.8) 645 (2.1) 7.9 157 (0.5) 1.9 1,036 (3.4) 12.7 4,821 (15.8) 58.9 5 (0.0) 0.1 By screening modality: womenf CA-125 888 (3.0) 567 (1.9) 63.9 349 (1.2) 39.3 0 (0.0) 0.0 103 (0.4) 11.6 125 (0.4) 14.1 TVU 2,310 (7.8) 745 (2.5) 32.3 1,394 (4.7) 60.4 1 (0.0) 0.0 677 (2.3) 29.3 874 (3.0) 37.8 CXR 5,531 (16.3) 2,907 (8.6) 52.6 1,498 (4.4) 27.1 56 (0.2) 1.0 93 (0.3) 1.7 40 (0.1) 0.7 FSG 5,239 (17.2) 321 (1.1) 6.1 151 (0.5) 2.9 906 (3.0) 17.3 3,072 (10.1) 58.6 7 (0.0) 0.1
Supplemental Tables 1-4
Supplemental Table 1. Estimators and 95% Confidence Intervals of the Cumulative Risk of Receiving at Least 1 False-Positive Result in 14 Tests; Supplemental Table 2. Estimators and 95% Confidence Intervals of the Cumulative Risk of Receiving at Least 1 False-Positive Result, by Screening Modality; Supplemental Table 3. Estimators and 95% Confidence Intervals of the Cumulative Risk of Receiving at Least 1 Invasive Diagnostic Procedure as a Result of a False-Positive Screening Test; Supplemental Table 4. Estimators and 95% Confidence Intervals of the Cumulative Risk of Receiving at Least 1 Invasive Diagnostic Procedure as a Result of a False-Positive Screening Test, by Screening Modality
Files in this Data Supplement:
- Supplemental data: Tables 1-4 - PDF file, 4 pages, 89 KB
The Article in Brief
Cumulative Incidence of False-Positive Results in Repeated, Multimodal Cancer Screening
Jennifer Miller Croswell , and colleagues
Background Although cancer screening tests play an important role in early detection of the disease, they can produce false-positive results (incorrect results that mistakenly identify cancer). This study examines the costs, in resources and human terms, of false-positive test results over time.
What This Study Found A large study that screened for cancers of the prostate, lung, colon and ovary found that the risk of a false-positive result increases with the number of screening tests. Specifically, by the fourth test, the risk of having at least one false-positive is about 37 percent for men and 26 percent for women. By the 14th test, the risk is approximately 60 percent for men and 49 percent for women. The risk of undergoing an invasive diagnostic procedure because of false-positive results is about 17 percent for men and 12 percent for women after four tests and 29 percent for men and 22 percent for women after 14 screening tests.
Implications
- This study provides a clearer picture of the burdens and risks associated with multiple cancer screening programs.
- Physicians and patients should discuss the likelihood of false-positive results in cancer screening, and they should examine the balance of risks and benefits in deciding on a patient's best course of action.
Annals Journal Club Selection:
May/Jun 2009
The Annals of Family Medicine encourages readers to develop the learning community of those seeking to improve health care and health through enhanced primary care. You can participate by conducting a RADICAL journal club, and sharing the results of your discussions in the Annals online discussion for the featured articles. RADICAL is an acronym for: Read, Ask, Discuss, Inquire, Collaborate, Act, and Learn. The word radical also indicates the need to engage diverse participants in thinking critically about important issues affecting primary care, and then acting on those discussions.1How it Works
In each issue, the Annals selects an article or articles and provides discussion tips and questions. We encourage you to take a RADICAL approach to these materials and to post a summary of your conversation in our online discussion. (Open the article online and click on "TRACK Comments: Submit a response.") You can find discussion questions and more information online at: http://www.AnnFamMed.org/AJC/.
Article for Discussion
- Croswell JM, Kramer BS, Kreimer AR, et al. Cumulative incidence of false-positive results in repeated, multimodal cancer screening. Ann Fam Med. 2009;7(3):212-222.
Discussion Tips
This analysis of a large cancer screening trial2 shows a negative aspect of cancer screening: the risk of a false-positive test and resulting further invasive testing. As a background for reviewing this article, it might be helpful to think of a range of patients: patients who have experienced a false-positive test, patients who did or did not do screening and were found to have cancer, patients who want every test. You also may wish to use discussion of this article to prime participants to look for further publications of results from the Prostate, Lung, Colorectal, and Ovarian (PLCO) Cancer Screening Trial.Discussion Questions
- What question is addressed by the article? How does the question fit with what already is known on this topic?
- How strong is the study design for answering the question?
- What is the degree to which can the findings be accounted for by:
- How participants were selected? The exclusion criteria and loss to follow-up? Are any biases likely to be important?
- How outcomes were measured?
- Confounding (false attribution of causality because two variables discovered to be associated actually are associated with a 3rd factor)?
- Chance?
- What are the main findings? How large is the effect for individual tests? What is the cumulative effect of repeated screening tests?
- What is the downside of screening tests in terms of follow-up invasive testing? What are possible other unintended consequences (both negative and positive)?
- What are the implications for how we talk with patients about screening tests?
- How might the forthcoming results of other outcomes of the PLCO trial affect how we interpret and use these findings?
- How transportable are the findings to your clinical setting? To other types of screening tests? What factors might affect this transportability?
- What are some next steps for applying the findings or answering other questions that this study raises?
References
- Stange KC, Miller WL, McLellan LA, et al. Annals journal club: It�s time to get RADICAL. Ann Fam Med. 2006;4(3):196-197. http://annfammed.org/cgi/content/full/4/3/196.
- Early Detection Research Group (EDRG). Prostate, Lung, Colorectal and Ovarian (PLCO) Cancer Screening Trial. http://prevention.cancer.gov/programs-resources/groups/ed/programs/plco. Accessed Feb 1, 2009.




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Screening for multiple cancers: evaluation must go beyond aggregate measures
- Assessing the rates of false-positive ovarian cancer screenings and surgical interventions associated with screening tools: a systematic review
- Evaluation of the Multi-Cancer Early Detection (MCED) value of YiDiXie™-HS and YiDiXie™-SS
- Modeled Reductions in Late-stage Cancer with a Multi-Cancer Early Detection Test
- False-Positive Results in a Population-Based Colorectal Screening Program: Cumulative Risk from 2000 to 2017 with Biennial Screening
- Diagnostic PET Imaging of Mammary Microcalcifications Using 64Cu-DOTA-Alendronate in a Rat Model of Breast Cancer
- Time to benefit for colorectal cancer screening: survival meta-analysis of flexible sigmoidoscopy trials
- Recommendations on screening for prostate cancer with the prostate-specific antigen test
- Identification of Potential Glycan Cancer Markers with Sialic Acid Attached to Sialic Acid and Up-regulated Fucosylated Galactose Structures in Epidermal Growth Factor Receptor Secreted from A431 Cell Line
- Lung Cancer Screening
- UK Lung Screen (UKLS) nodule management protocol: modelling of a single screen randomised controlled trial of low-dose CT screening for lung cancer
- Clinical Cancer Advances 2009: Major Research Advances in Cancer Treatment, Prevention, and Screening--A Report From the American Society of Clinical Oncology
- In This Issue: The Science, Art, and Policy of Primary Care