
Article Figures & Data
Figures
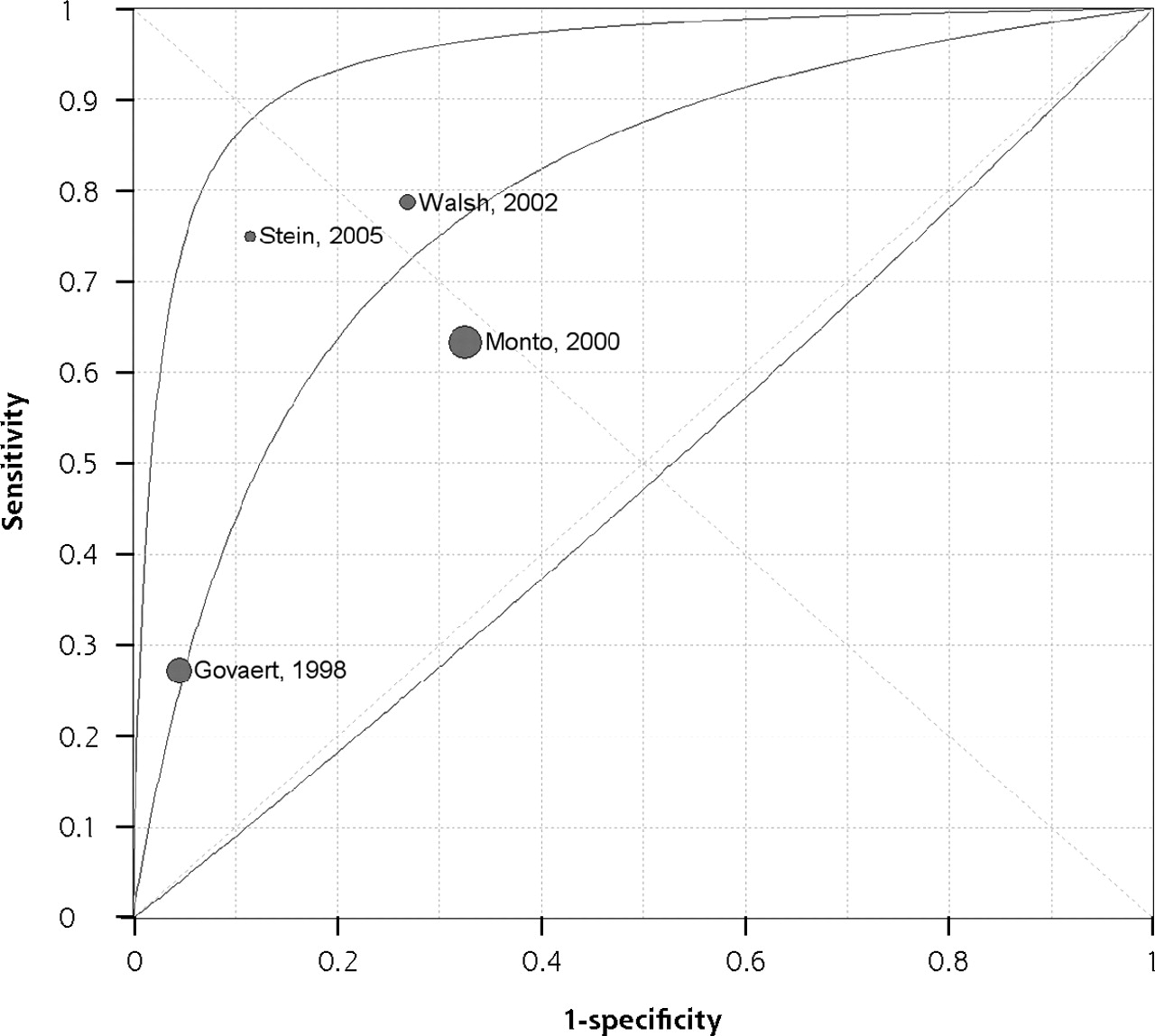
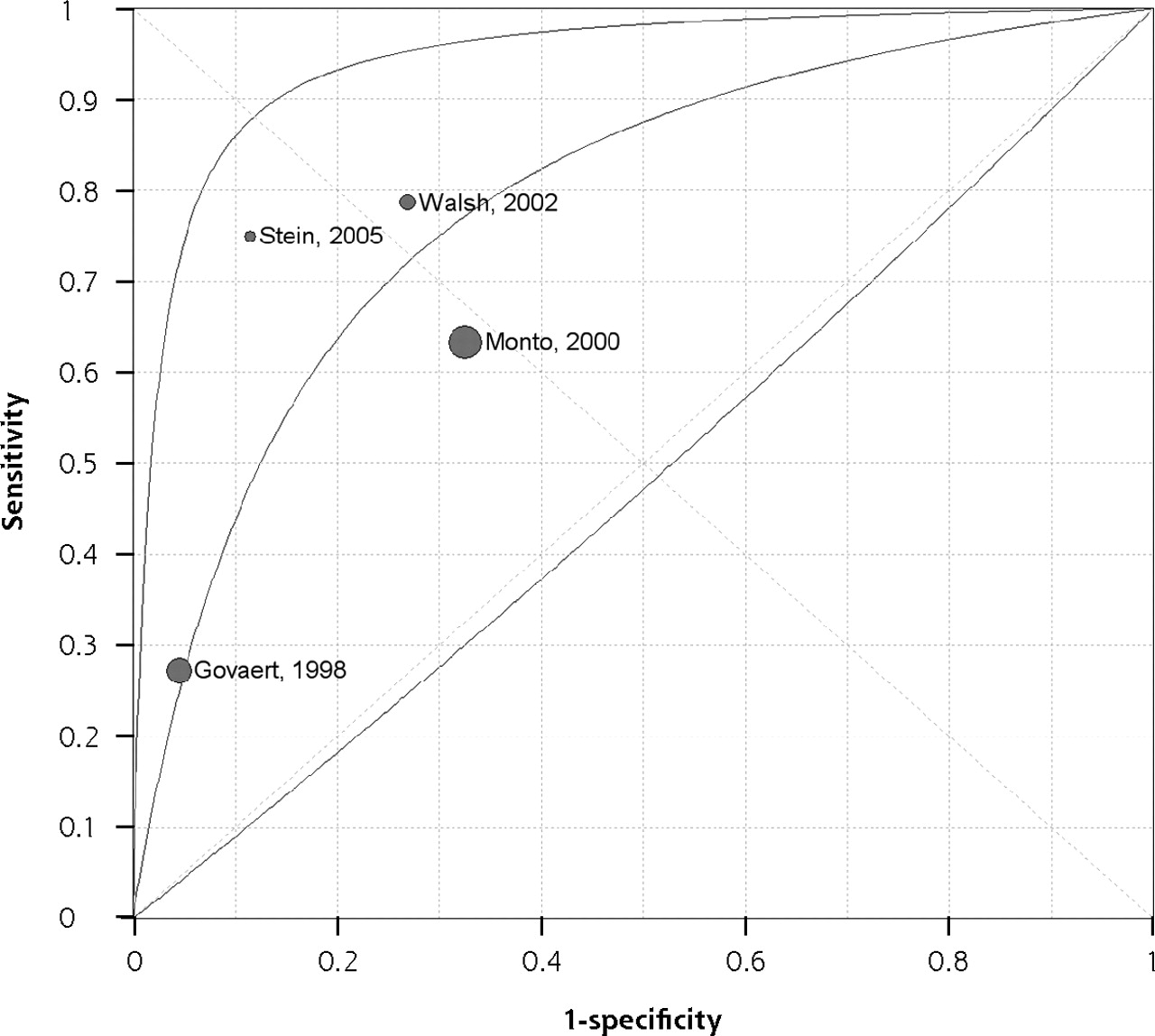
- Figure 1.
Summary ROC curve for the fever and cough rule.
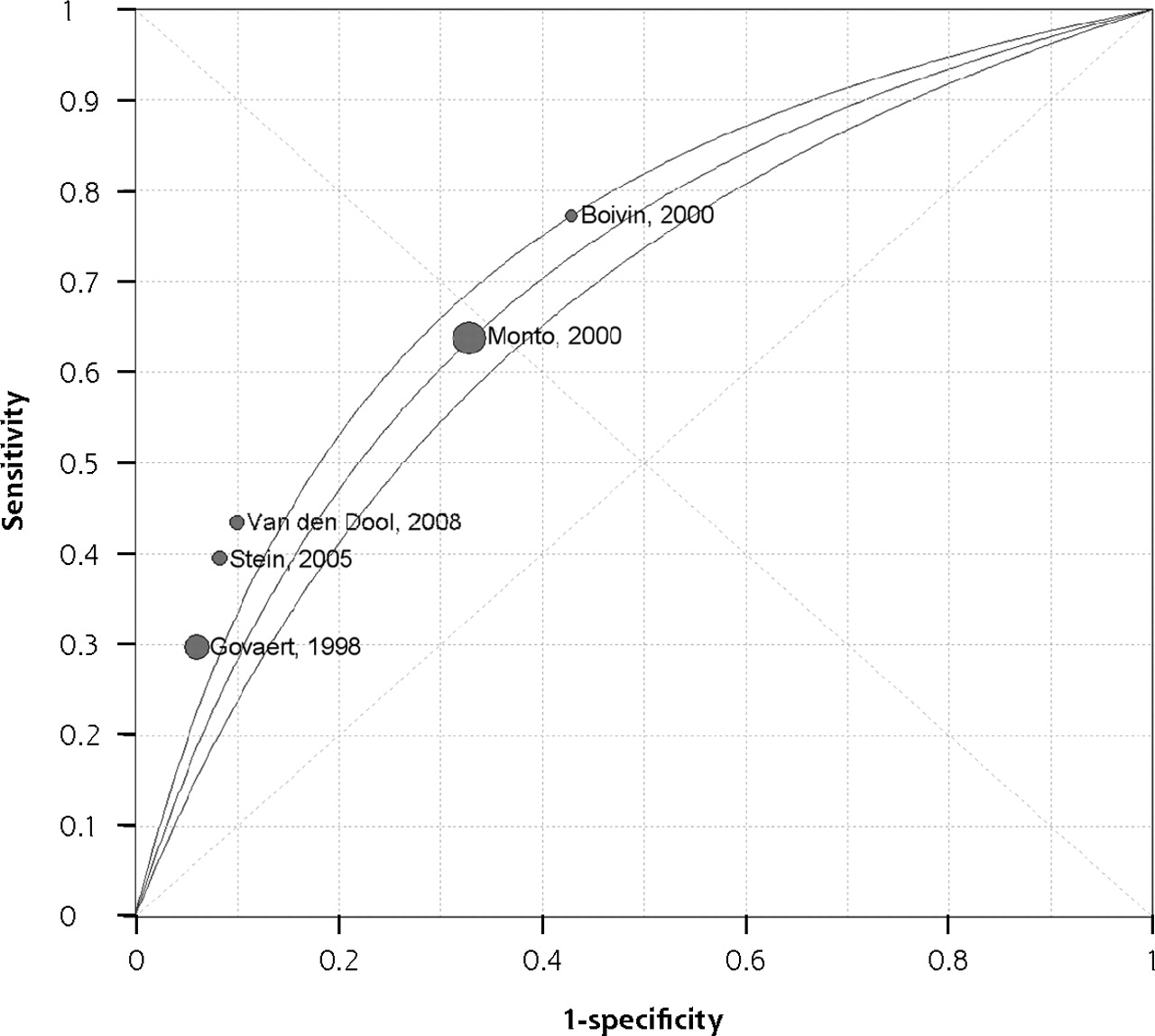
- Figure 2.
Summary ROC curve for the fever, cough, and acute onset rule.
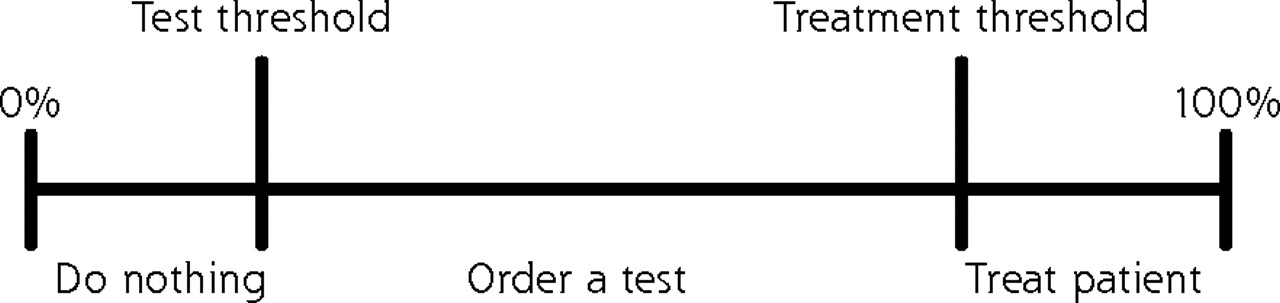
- Figure 3.
Threshold model for diagnosis of influenza.

Tables
- Table 1.
Results From a Previous Systematic Review of the History and Physical Examination for the Diagnosis of Influenza
Likelihood Ratio for Influenza Clinical Finding Positive Negative Note: Data from Ebell et al.2 Rigors 7.2 0.9 Sweating 2.9 0.6 Being confined to bed 2.5 0.5 Inability to cope with daily activities 2.3 0.4 Fever (subjective) 1.7 0.5 Absence of systemic symptoms 1.5 0.4 Headache 1.3 0.6 Cough 1.3 0.4 Myalgia 1.3 0.6 Nasal congestion 1.2 0.7 Chills 1.1 0.7 Sore throat 1.1 0.9 Sputum 1.1 0.9 Study and Year Population and Season(s) N Influenza Prevalence, % Country Reference Standard Comment DIF=direct immunofluorescence; ED = emergency department; ELISA = enzyme-linked immunosorbent assay; ILI = influenza-like illness; NPV = negative predictive value; PCR = polymerase chain reaction; RSV = respiratory syncytial virus; RTI = respiratory tract infection. Govaert et al,13 1998 Average-risk, unvaccinated primary care patients older than 60 y with ILI during 1991–1992 flu season 1,838 (logistic regression); 1,791 (heuristics) 6.6 Netherlands Increase in antibody titer Any symptoms reported during study period were included; part of randomized trial of vaccination. Carrat et al,23 1999 Primary care patients older than 1 y with ILI, RTI syndrome, and/or fever >38°C without signs of other infections during 1995–1996 flu season 600 26 France DIF and ELISA; if disagreement, further testing with PCR and culture Separate models created for H1N1 and H3N2 subtypes, and for all influenza. Monto et al,11 2000 Adolescent or older with fever and ≥2 other symptoms (headache, myalgia, cough, or sore throat) during fall or winter of 1994–1998 3,744 66 North America, Europe, southern hemisphere Culture or increase in antibody titer (in some studies PCR or immunofluorescence) High prevalence of influenza. Data from 6 randomized trials of zanamivir vs placebo. Boivin et al,12 2000 Patients with ILI (fever ≥37.8°C and ≥2 other symptoms) seeking care at an outpatient clinic during 1998–1999 flu season 100 79 Canada PCR and culture – van Elden et al,10 2001 Primary care patients with fever (≥38°C), ≥1 constitutional symptom (malaise, headache, myalgia, chills), and ≥1 respiratory symptom (coryza, sneeze, cough, sore throat, hoarseness) seeking care within 48 hr of onset during 1997–1998 flu season 81 51 Netherlands PCR and culture Only PCR results were used for model development. Zambon et al,19 2001 Persons aged 12 y or older seen within 48 hr of onset of ILI as part of a multicenter international clinical trial of an influenza drug 1,033 77 (any test positive); 67 (all 3 tests positive) Europe, North America PCR, culture, or increase in antibody titer Reference standard was abnormal finding on all 3 tests. Walsh et al,21 2002 Inpatients older than age 65 y or with underlying cardiopulmonary conditions with a respiratory diagnosis during 1999–2000 flu season 332 18 United States Culture, rapid antigen test, increase in antibody titer, or PCR A model with 2 variables (temperature >38°C and absence of dyspnea) reportedly did not discriminate well; results not reported by authors. Friedman and Attia,20 2004 Children (0–17 y) seen in the ED with suspected ILI (fever and coryza, cough, headache, sore throat, or muscle aches) during 2002 flu season 128 35 United States Culture – Senn et al,7 2005 Persons with ILI seeking care at an outpatient clinic during 1999–2000 flu season 201 52 Switzerland Culture Cutoff for logistic model presumably probability of influenza >50%. Stein et al,8 2005 Consecutive adults with RTI in past 3 wk with cough, sinus pain, congestion/ rhinorrhea, sore throat, or fever seen in the ED during 2002 flu season 258 21 United States PCR Validated previously developed fever and cough rule.11 Ohmit and Monto,24 2006 Study 1 (zanamivir): children aged 5–12 y with fever and duration of illness <36 hr during flu season Study 2 (oseltamivir): children aged 1–12 y with fever and cough or nasal symptoms, and duration <48 hr during flu season Study 1: 468 Study 2 (1–4 y): 255 Study 2 (5–12 y): 221 Study 1: 74 Study 2: 67 United States Culture and/or 4-fold increase in antibody titer (or PCR in zanamivir trial only) Validated previously developed fever and cough rule.11 RSV infection excluded. Unable to calculate sensitivity, specificity, NPV from data for fever and cough rule. van den Dool et al,22 2008 Adult inpatients in the general medicine, pulmonology, and infectious disease wards of a tertiary care hospital during 2006–2007 flu season 264 8.7 Netherlands PCR Included all patients regardless of symptoms; validated previously developed fever and cough rule.11 - Table 3.
Quality Assessment of Included Studies Based on the QUADAS Tool for Studies of Diagnostic Accuracy27
Criterion Govaert et al,13 1998 Carrat et al,23 1999 Monto et al,11 2000 Boivin et al12, 2000 van Elden, et al,10 2001 Zambon et al,19 2001 Walsh et al, 21 2002 Friedman and Attia,20 2004 Senn et al,7 2005 Stein et al,8 2005 Ohmit and Monto,24 2006 van den Dool et al,22 2008 N=no; NA=not applicable; QUADAS=Quality Assessment of Diagnostic Accuracy; U=unknown; Y=yes. a Participants were classified as being representative of patients who will receive the test in practice if they were undifferentiated outpatients with symptoms of respiratory tract infection. Participants were classified as not being representative if they were a subset of inpatients. b No temperature cutoff was given for definition of fever. c Although not explicitly stated, it is unlikely that diagnostic laboratories verifying the presence of influenza had access to the clinical data of each patient. 1. Was the spectrum of participants representative of the patients who will receive the test in practice? Ya Y a Ya Ya Y a Ya Na Ya Y a Ya Ya Na 2. Were selection criteria clearly described? Y Y Y Y Y Y Y Y Y Y U Y 3. Was the reference standard likely to classify the target condition correctly? Y Y Y Y Y Y Y Y Y Y Y Y 4. Was the period between performance of the reference standard and the index test short enough to be reasonably sure that the target condition did not change between the 2 tests? Y Y Y Y Y Y Y Y Y Y Y Y 5. Did the whole sample or a random selection of the sample receive verification using the reference standard? Y Y Y Y Y Y Y Y Y Y Y Y 6. Did participants receive the same reference standard regardless of the index test result? Y Y Y Y Y Y Y Y Y Y Y Y 7. Was the reference standard independent of the index test? Y Y Y Y Y Y Y Y Y Y Y Y 8. Was the execution of the index test described in sufficient detail to permit its replication? Yb Y Y Y Y Y Y Y Y Y Y Y 9. Were the index test results interpreted without knowledge of the results of the reference test? Y Y Y Y Y Y Y Y Y Y Y Y 10. Were the reference standard results interpreted without knowledge of the results of the index test? Uc Uc Uc Uc Uc Uc Uc Uc Uc Uc Uc Uc 11. Were the same clinical data available when the test results were interpreted as would be available when the test is used in practice? U U U U U U U U U U U U 12. Were uninterpretable, indeterminate, or intermediate test results reported? U Y Y Y Y Y Y U Y Y U Y 13. Were withdrawals from the study explained? NA NA NA NA NA NA NA NA NA NA NA NA - Table 4.
Multivariate Models, Point Scores, and Symptom Combinations Reported by Included Studies
Study Model Accuracy AUC = area under the receiver operating characteristic curve; CI = confidence interval; LR+ = positive likelihood ratio, LR− = negative likelihood ratio; NPV = negative predictive value; OR = odds ratio; PPV = positive predictive value. Govaert et al,13 1998 Variable: OR Not reported Cough: 5.25 Fever: 2.18 Vaccinated: 0.56 Constant: 0.041 Govaert et al,13 1998 Symptom count (fever, cough, acute onset, malaise, rigors or chills, myalgia, headache, sore throat) Not reported other than data shown Score (n): % influenza 0 (1,155): 3.2 1–2 (145): 6.2 ≤3 (491): 15 Carrat et al,23 1999 Variable: OR Goodness of fit: P=.98 All influenza Temperature >38.2°C: 2.45 Rhinorrhea: 1.83 Temperature >38.9°C, respiratory signs, and stiffness or myalgia Temperature >37.7°C and cough or sore throat Any 3 of temperature >37.7°C, cough, chills, moderate/severe fatigue, cervical or dorsal pain, pharyngitis, and another case at patient’s home PPV: 40%; NPV: 80% PPV: 30%; NPV: 86% PPV: 27%; NPV: 91% Monto et al,11 2000 Variable: OR (95% CI) Accuracy of multivariate model not reported Fever >37.7°C: 3.26 (2.75–3.87) Cough: 2.85 (2.21–3.68) Nasal congestion: 1.98 (1.54–2.54) Age ≥55 y: 1.60 (1.18–2.16) Weakness: 1.54 (1.07–2.22) Onset >36 hr: 1.53 (1.24–1.90) Loss of appetite: 1.43 (1.10–1.86) Sex, male: 1.27 (1.08–1.50) Sore throat: 0.72 (0.57–0.91) Boivin et al,12 2000 Variable: OR (95% CI) PPV: 87%; NPV: 39% Cough: 6.68 (1.4–34.1) Temperature ≥38°C: 3.06 (1.35–8.02) van Elden et al,10 2001 Period of increased influenza activity, cough, headache at onset, feverishness at onset, and not vaccinated During an outbreak, abrupt onset (<5 days), temperature >38°C, and at least 1 of cough, coryza, headache, retrosternal pain, or myalgia At least 4 of sudden onset, contact with influenza, fever, cough, chills, malaise, myalgia, or hyperemic mucous membranes of the nose and throat (≥6 required if not in outbreak) PPV: 75%; NPV: 80% PPV: 52% PPV: 54%; NPV: 85% Senn et al,7 2005 Week of consultation (49–50 vs ≥51), duration of symptoms (≤48 hr vs >48 hr), temperature >37.8°C, and cough AUC=0.74 Sensitivity: 80%; specificity: 59% LR+: 1.95; LR−: 0.34 PPV: 67%; NPV: 73% LR+/LR−=5.7 Ohmit and Monto,24 2006 Study 1, zanamivir—variable: OR (95% CI) Accuracy not reported; only variables significant at P <.05 level included Age, y: 1.11 (1.00–1.23) Fever: 2.67 (1.66–4.30) Cough: 5.19 (2.66–10.10) Myalgia: 0.61 (0.38–0.99) Sore throat: 0.41 (0.24–0.70) Study 2, oseltamivir (age 1–4 y)—variable: OR (95% CI) Myalgia: 2.32 (1.22–4.39) Study 2, oseltamivir (age 5–12 y)—variable: OR (95% CI) Cough: 10.94 (2.90–40.80) Headache: 2.24 (1.15–4.37) Rule and Studya Heuristic Sensitivity, % Specificity, % PPV, % NPV, % LR+ LR− LR+/ LR− ILI=influenza-like illness; LR− = negative likelihood ratio; LR+ = positive likelihood ratio; NPV = negative predictive value; PPV = positive predictive value; RTI=respiratory tract infection. a Study population and prevalence of influenza are shown in Table 2. b Odds ratio in logistic regression model was 6.7 for cough and 3.1 for temperature greater than 38°C. c Odds ratio in logistic regression model was 7.2 for cough, 4.3 for headache, and 3.9 for pharyngitis. Fever and cough rule Stein et al,8 2005 Fever (≥37.8°C) and cough 40 92 58 84 5.1 0.7 7.3 Govaert et al,13 1998 Fever (>38°C) and cough 30 94 26 95 5.0 0.74 6.8 Boivin et al,12 2000b Fever (≥37.8°C) and cough 78 55 87 39 1.7 0.4 4.3 Monto et al,11 2000 Fever (≥37.8°C) and cough 64 67 79 49 1.94 0.54 3.6 van den Dool et al,22 2008 Fever (>38.3°C) and cough 42 90 26 95 4.2 0.64 6.5 Fever, cough, and acute onset rule Stein et al,8 2005 Fever (≥37.8°C), cough, and duration ≤48 hr 75 89 65 93 6.5 0.3 21.7 Walsh et al,21 2002 Fever (≥38°C), cough, and duration <7 days 78 73 47 91 2.9 0.3 9.7 Govaert et al,13 1998 Fever (>38°C), cough, and acute onset 27 95 30 95 5.9 0.76 7.8 Monto et al,11 2000 Fever (≥37.8°C), cough, and acute onset 63 68 77 51 1.95 0.54 3.6 Cough, headache, and pharyngitis rule Friedman and Attia,20 2004c Cough, headache, and pharyngitis 80 78 77 81 3.7 0.26 14.2
The Article in Brief
A Systematic Review of Clinical Decision Rules for the Diagnosis of Influenza
Mark H. Ebell , and colleagues
Background Clinical decision rules to accurately identify patients at low, moderate, or high risk of influenza could help doctors determine appropriate treatment and avoid unnecessary tests. The goal of this analysis of previous research is to identify and evaluate the accuracy and validity of existing clinical decision rules for the diagnosis of influenza.
What This Study Found This systematic review of 12 articles regarding clinical decision rules for the diagnosis of influenza found that, although influenza is a common cause of illness and death, studies about diagnosing this infection are largely small, use varied inclusion criteria and reference standards, and do not report their results in a way that would be helpful to clinicians. No study prospectively evaluated a clinical score or multivariate model for diagnosing influenza. Rather, the studies validated only simple clinical heuristics, such as �fever and cough� and �fever, cough, and acute onset,� and even then, the sensitivity and specificity varied considerably, and it was not possible to calculate summary measures of accuracy for these rules.
Implications
- Future research is needed to validate multivariate models for the diagnosis of influenza, as well as point scores that are easier for clinicians to use at the point of care.




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Accuracy of individual signs and symptoms and case definitions for the diagnosis of influenza in different age groups: a systematic review with meta-analysis
- Diagnostic models predicting paediatric viral acute respiratory infections: a systematic review
- A Systematic Review of Clinical Prediction Rules for the Diagnosis of Influenza
- Leveraging UMLS-driven NLP to enhance identification of influenza predictors derived from electronic medical record data
- Clinical presentation and microbiological diagnosis in paediatric respiratory tract infection: a systematic review
- Development and Validation of a Clinical Decision Rule for the Diagnosis of Influenza
- In This Issue: Clinical Decision Support