
Abstract
PURPOSE We wanted to determine the diagnostic value of an oral prednisolone test for chronic obstructive pulmonary disorders.
METHODS Two hundred thirty-three patients with cough for longer than 14 days, without known chronic obstructive pulmonary disease (COPD) or asthma, participated in a diagnostic study in Dutch primary care between 2006 and 2009. These patients used a 14-day prednisolone test of 30 mg/d and recorded before-after bronchodilator measurements of forced expiratory volume in 1 second (FEV1). An expert panel determined the presence or absence of COPD and asthma based on an extensive diagnostic workup. The proportion of responders to the prednisolone test (increased FEV1 exceeding 200 mL or 12% of baseline) per diagnosis group was compared, and the diagnostic value of the test was quantified by logistic regression and analysis of the area under the receiver operating characteristic curve (ROC area).
RESULTS In patients with COPD, 23% (14 of 61) responded to the test; in patients with asthma 4% (1 of 25) responded; in patients with asthma and COPD, 7% (1 of 14) responded; and in those without asthma or COPD, 11% (14 of 133) responded. Being a responder was, unexpectedly, associated with COPD (OR = 2.4; 95% confidence interval [CI], 1.1–5.2). After multivariate analysis, adjusting for age, sex, and smoking, the OR = 2.0 (95% CI, 0.8–5.0) and the ROC area did not increase (0.78; 95% CI, 0.72–0.85 vs 0.79; 95% CI, 0.72–0.85).
CONCLUSION A response to a prednisolone test was suggestive of COPD, but added no diagnostic value to more easily obtainable characteristics.
INTRODUCTION
Diagnosing chronic obstructive lung disorders, such as chronic obstructive pulmonary disease (COPD) and asthma, is important, because adequate treatment improves quality of life and reduces exacerbations.1,2 In primary care a diagnosis of COPD or asthma is mainly based on the results of history, physical examination, and spirometry.1–3 The interpretation of spirometry results is not straightforward, however, as there are no fixed values for (obstructive) spirometry results that confirm COPD or asthma, and results often vary with time.4,5
It has been suggested that repeating spirometry after a test treatment with oral corticosteroids might be helpful in the diagnostic workup of chronic lung disorders. A substantial improvement—or reversibility—of spirometry results, usually quantified as the forced expiratory volume in 1 second (FEV1), is often assumed to suggest reversible airway disorders, such as asthma,1,2 whereas a lack of improvement is considered indicative of COPD. Whether this assumption is true is unclear. There are no studies reporting the diagnostic value of the prednisolone test in patients with suspected asthma or COPD. Moreover, a meta-analysis showed that a positive response (a greater than 20% increase in FEV1) was common after a short course of oral corticosteroids in patients with known stable COPD.6
The extent to which a test treatment of oral corticosteroids is of diagnostic value in patients with complaints suggestive of COPD or asthma remains to be established.7 The aim of our study was to quantify the added diagnostic value of this test treatment in a large primary care population of patients with complaints of cough.
METHODS
Design and Study Population
For the present study 400 persons who were participating in a diagnostic study of COPD performed in Dutch primary care from January 2006 to May 2009 were eligible for inclusion. The protocol of this diagnostic study is described in detail elsewhere.8 Inclusion criteria were age older than 50 years and consulting a general practitioner for complaints of cough lasting 14 days or longer. Exclusion criteria were known COPD or asthma, physician-suspected pneumonia, and terminal illness. All participants gave written informed consent, and the medical ethics committee of the University Medical Centre Utrecht approved the study.
All 400 participants underwent an extensive standardized diagnostic work-up, including history, physical examination, spirometry, and whole body plethysmography. Our study focused on a subgroup of these participants who underwent a diagnostic test treatment with oral prednisolone (the prednisolone test).
Test Treatment With Prednisolone
For the prednisolone test the participants were prescribed 14 tablets of prednisolone 30 mg to take once a day for 14 days. To prevent potential gastroduodenal toxicity,9 omeprazol 20 mg daily was prescribed when a participant reported a history of gastrointestinal ulcer or hemorrhage or was using nonsteroidal anti-inflammatory drugs, anticoagulants, or serotonin reup-take inhibitors. Participants with diabetes mellitus were instructed to measure fasting glucose after 1 week and adjust their diabetes medication, if necessary.
Participants underwent spirometry on the day before the start of the 14-day prednisolone test, as well as 14 days later. Spirometry measurements included forced vital capacity (FVC), FEV1, and the FEV1/FVC ratio after bronchodilation with 400 μg of salbutamol, using multi-window Spida 5 software combined with a SpiroUSB hand-held spirometer(ML2525; CareFusion, Chatham Maritime, Kent, United Kingdom). Participants were instructed not to use inhaled medication on the days of spirometry. We started the prednisolone test and thus the first spirometry on day 42 after participant inclusion rather than on day 1, because spirometry results are often unreliable during episodes of cough.10 Participants were asked to consult a research physician in case of presumed side effects. After the prednisolone test, participants reported how many prednisolone tablets were used. Participants who did not undergo the prednisolone test, underwent the subsequent study tests according to the protocol as much as possible.
Diagnostic Outcome
As described elsewhere,8 the presence or absence of COPD and asthma (diagnostic outcome) was determined by an expert panel of 2 physicians, using the results of all tests—except those of the prednisolone test—according to international guidelines.1,2
The panel also determined the severity of COPD according to the criteria of the Global Initiative for Chronic Obstructive Lung Disease (GOLD),1 as well as other possible diagnoses.
A diagnosis of COPD required recurrent complaints of cough, sputum, or breathlessness, in addition to lung obstruction after bronchodilator use, defined as a lowered FEV1/FVC ratio and a concave dip in the second part of the spirometry curve. According to the GOLD guidelines, a postbronchodilator FEV1/FVC ratio of less than 70% confirms airflow limitation.1 Because the FEV1/FVC ratio physiologically decreases with age, however, COPD was not diagnosed in every participant with an FEV1/FVC ratio of less than 70%. For the same reason a diagnosis of COPD was allowed without this index being less than 70% in young people.11 A history of smoking was supportive but not required for COPD. A diagnosis of asthma required recurrent episodes of wheezing, cough, or dyspnea, as well as an increase of FEV1 of more than 200 mL or more than 12% of baseline2 after bronchodilation. Allergy and eczema were supportive for asthma. According to the Dutch guidelines for general practitioners, both asthma and COPD could be diagnosed when FEV1 increased by more than 12% or 200 mL and the postbronchodilator FEV1/FVC ratio was less than 70%, in combination with complaints suggestive of both disorders.12,13
Data Analysis
The response to the prednisolone test was quantified as the increase of the postbronchodilator FEV1, and expressed in milliliters and percentage of the baseline postbronchodilator FEV1. The mean increase was determined in patients with and without COPD and asthma.
The participants were categorized as responders or nonresponders to the prednisolone test. A participant was considered a responder if the increase of FEV1 exceeded 200 mL or 12% of the baseline value.14 We further quantified the diagnostic value of being a responder to the prednisolone test for the presence of absence of COPD. The positive and negative predictive value and the positive and negative likelihood ratio for presence or absence of COPD of being a responder was calculated. The association between being a responder and COPD was also determined using univariate logistic regression analysis, resulting in a univariate odds ratio (OR) with a 95% confidence interval (95% CI). Then, using multivariate logistic regression, this association was quantified after adjustment for differences in age, sex, and current smoking, all known strong risk indicators for COPD,1 to determine the diagnostic value of the prednisolone test in addition to these characteristics. The area under the receiver operating characteristic curve (ROC area) of the multivariate model with and without the prednisolone test was quantified to determine the independent discriminative value of the prednisolone test. Analyses were performed in SPSS 15.0 (SPSS, Inc, Chicago, Illinois) and R 2.8.1.15
RESULTS
Figure 1 displays the flowchart for study participants. Of the 400 study participants who were eligible for study inclusion, 233 agreed to a diagnostic test treatment of oral prednisolone. Participants who refused to undergo the prednisolone test and those without sufficient spirometry results were excluded from the present analysis on the prednisolone test. Medical and spirometry characteristics for the study participants are displayed in Table 1. The included and excluded participants did not differ, except for pack years of smoking and baseline ratio of the FEV1 to the forced vital capacity (FEV1/FVC ratio).
Characteristics of Included and Excluded Participants Measured Before Prednisolone Test Treatment
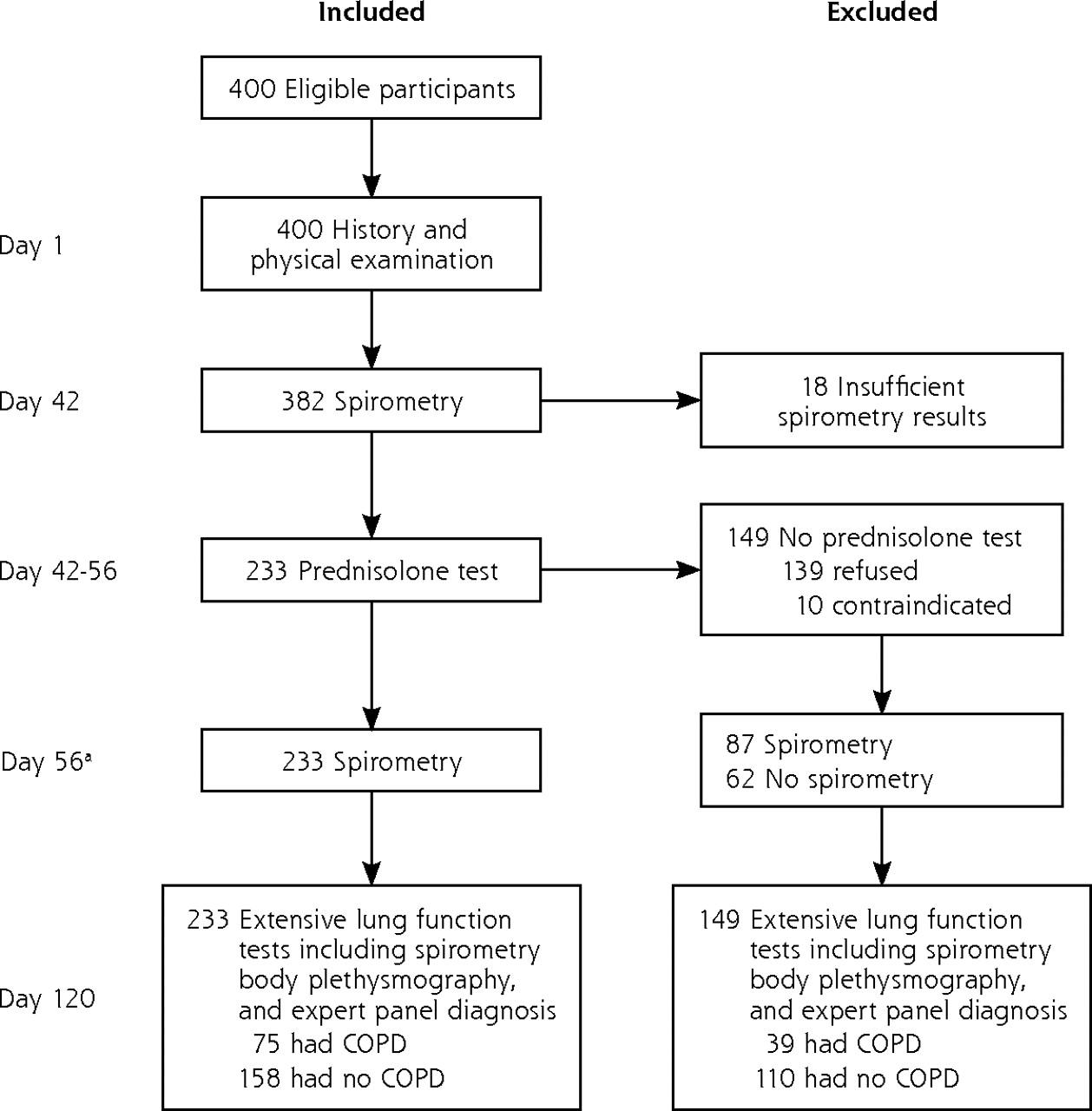
Flowchart of the study and the participants.
COPD = chronic obstructive pulmonary disease.
a Spirometry after the prednisolone test took place maximally 5 days after the 14th day of prednisolone treatment.
Of the 233 included participants who agreed to the prednisolone test, 217 completed the test treatment of 14 tablets. Of the 16 participants using fewer than 14 tablets (average number of tablets used was 7, minimum 2, and maximum 13), 14 did so because of side-effects, mainly gastrointestinal complaints (n = 9) and disordered sleep (n = 4). The mean age of participants was 63 years, and mean duration of cough was 110 days with a median of 42 days. Excluded persons (n = 167) on average smoked fewer pack years and had a higher FEV1/FVC ratio than included participants (Table 1).
Response to the Test Treatment With Prednisolone in 233 Patients With Persistent Cough
Results of Univariate Characteristics of the Prednisolone Test for COPD and Multivariate Analysis of Responder Characteristics
COPD was diagnosed in 61(26%) of the 233 participants; 38 had mild disease (FEV1 was greater than 80% of predicted), and 23 had moderate disease (FEV1 was 50%-80% of predicted). Twenty-five patients (11%) had asthma, and 14 patients (6%) had both (mild) COPD and asthma. The mean increase of FEV1 after the prednisolone test was 1% in all participants (SD = 9%; interquartile range = −4% to 4%). The mean FEV1 increase per diagnosis group is shown in Table 2. The proportion of responders to the prednisolone test was 23% in patients with COPD, 4% in patients with asthma, 7% in patients with both asthma and COPD, and 11% in those without asthma or COPD (P = .04).
Because results showed, contrary to our hypothesis, that the proportion of responders was much larger in patients with COPD than in those without COPD (Table 2), suggesting that the prednisolone test could be helpful to discriminate COPD from no COPD, we further quantified the diagnostic value of being a responder to the prednisolone test for the presence of absence of COPD. The positive predictive value (PPV) and negative predictive value (NPV) of the prednisolone test for COPD were 50% and 70%, respectively (Table 3). Being a responder to the prednisolone test was associated with the presence of COPD (OR = 2.4; 95% CI, 1.1–5.2). After adjustment for age, sex and current smoking, OR = 2.0 (95% CI, 0.8–5.0) (Table 3). The ROC area of the model including age, sex, and current smoking was 0.78 (95% CI, 0.72–0.85), and the ROC area of the model also including the prednisolone test was 0.79 (95% CI, 0.72–0.85). The P value for the difference from a reference value of 0.5 for the ROC area was <.001 for both models, and for the difference between the 2 models, P = .9.
A separate analysis among the 217 patients who completed the test treatment (intention-to-test analysis) yielded similar findings (univariate analysis, OR = 2.6; 95% CI, 1.7–5.8; and multivariate analysis, OR = 2.3; 95% CI, 0.9–5.7) for the association between being a responder and the presence of COPD. An analysis of the increased FEV1 between day 42 and day 56 in 87 of the 167 participants who did not undergo the prednisolone test (Table 1 and Figure 1) showed that the proportion of responders was 9% (2 of 23) in participants with COPD, and 8% (5 of 64) in participants without COPD (P = .9)
DISCUSSION
We studied the response to a 14-day test treatment with oral prednisolone 30 mg/d in 233 patients complaining of cough. Being a responder was associated with COPD. After adjustment for 3 patient characteristics (age, sex, and current smoking), the multivariate association between the prednisolone test and COPD was not statistically significant; hence, the prednisolone test had no relevant added diagnostic value. Our findings were not consistent with our hypothesis that being a nonresponder is more likely in patients with COPD than with asthma.
Some possible limitations of our study should be addressed. First, 39% of participants did not take the prednisolone test, and for only a minority was not taking the test attributable to an established contraindication for corticosteroids, such as insulin dependency or osteoporosis. Because the patients who refused did not differ substantially from those who participated, except for pack years of smoking and the baseline spirometry results, it is highly unlikely that refusal was related to the response to the prednisolone test. We therefore believe that our estimated diagnostic findings are generalizable to patients suspected of having COPD in primary care settings. Even so, 39% of participants suspected to have COPD showed a low level of willingness to undergo the prednisolone test.
Second, one could argue that our analyses should have been limited to those patients who completed the test treatment. Because nonadherence to the full regimen is also likely to occur, however, we decided to take a pragmatic approach and report the findings for those who started the test to enhance generalizability to clinical practice.
Third, one might argue that increased FEV1 after the prednisolone test in this study might also have occurred without prednisolone, as spirometry results can vary largely within patients with pulmonary disease.5 Our results on the patients not undergoing the prednisolone test, however, suggest that the difference between the proportion of responders in participants with and without COPD who underwent the prednisolone test was indeed related to this test.
To our knowledge, the diagnostic value of a test treatment with prednisolone in patients suspected of COPD has not been reported before. In the COOPT study and in the Isolde study, a 14-day test treatment with oral prednisolone was studied in patients with known COPD with the aim to predict benefit from inhaled steroid treatment. Both studies found that the test did not predict beneficial effect of inhaled fluticasone.16,17 These results led to the recommendation not to use a test of oral corticosteroids in patients with proven COPD to decide on prescription of long-term inhaled steroids.1
In our study, the relatively high proportion of responders in participants with COPD could be related to ongoing eosinophil (or other corticosteroid-sensitive) inflammation,18,19 illustrated a subgroup of patients with COPD that respond well to long-term inhaled corticosteroids.20,21 Our findings are in line with the understanding that COPD is a heterogenic disorder, characterized by airflow obstruction that is not fully reversible and an abnormal inflammatory airway response.1,22 In analogy to the improvement or reversibility of spirometric results after a prednisolone test, reversibility after inhaled bronchodilators is currently recognized as a common feature of COPD, whereas earlier a lack of reversibility was considered typical for COPD.21,23–27
The widely acknowledged underdiagnosis and misdiagnosis of chronic lung disorders in primary care underline a need for more consistent criteria than expert opinion to define chronic lung disorders. Moreover, and especially in elderly patients, asthma and COPD often overlap, usually in patients with asthma who are exposed to cigarette smoke or other noxious gases, who develop a COPD-like obstructive spirometry pattern.2,28 Extensive history taking is currently acknowledged as the main tool to differentiate asthma from COPD, and questionnaires were recently developed for this purpose.29,30
Being a responder to a 14-day test treatment with oral prednisolone was suggestive of COPD, contrary to earlier assumptions, but had no clear value for diagnosing or excluding COPD in addition to more easily obtainable diagnostic information. In view of the unwillingness of many patients to undergo the prednisolone test, we do not recommend this test in the diagnostic workup when chronic obstructive lung disorders are suspected.
Acknowledgements
We gratefully acknowledge all participating patients, general practitioners, and other health care professionals who contributed to the study. Chantalle van de Pas and Nanoesjka van Gorcum, research physicians, performed spirometry measurements.
Footnotes
-
Conflicts of interest: Dr Sachs has been a speaker at congresses sponsored by GlaxoSmithKline, Boehringer-Ingelheim, Pfizer or AstraZeneca. Dr Verheij participates in studies that received grants from GlaxoSmithKline and Wyeth.
-
Financial support: This work was funded by the Netherlands Organisation for Health Research and Development (ZonMw), grant No. 945-04-015; and research grants from GlaxoSmithKline, Boehringer-Ingelheim, and Pfizer.
-
Disclaimer: The study sponsors had no involvement in the study design, the collection, analysis, and interpretation of the data, the writing of the report, or in the decision to submit the paper for publication.
- Received for publication May 25, 2010.
- Revision received October 25, 2010.
- Accepted for publication November 5, 2010.
- © Annals of Family Medicine, Inc.




{kind=link}