Table of Contents
PLAIN-LANGUAGE SUMMARIES

Embargoed until 5 p.m. Eastern Daylight Time
Monday, September 23rd, 2024
Original Research
Higher Gonorrhea Rates Observed Among Gay and Bisexual Men in Ontario Using PrEP Compared With Non-Users
Background and Goal: Pre-exposure prophylaxis (PrEP) is a preventive medicine that reduces the risk of contracting HIV. There is concern that PrEP use may be associated with an increase in bacterial sexually transmitted infections (STIs) like gonorrhea, chlamydia, and syphilis among men who are gay or bisexual, or have sex with men, although the reasons for this association are complex. This study aimed to explore the relationship between PrEP use and the rates of bacterial sexually transmitted infections over time.
Study Approach: Researchers used data from the iCruise Study, an online longitudinal study of men who are gay or bisexual, or have sex with men, in Ontario from July 2017 to April 2018, to examine how PrEP use related to the number of self-reported bacterial STIs. For this study, 659 participants in the iCruise Study were randomly selected to participate in a weekly diary survey for up to a three-month study period. Instances of chlamydia, gonorrhea, and syphilis infections were measured as the number of infections per 100 months of participant observation time. The overall infection rate and each type of infection were evaluated separately.
Main Results:
-
535 participants in the iCruise Study were included in the analysis. Participants were followed for a total of 1,623.5 person-months (the total time all participants were in the study). About 13.1% (70 participants) reported using PrEP during the study period.
-
PrEP use was linked to a higher rate of gonorrhea:
-
The initial analysis suggested that the rate of gonorrhea among PrEP users was four times higher than among non-users, with an incidence rate ratio of 4.00 (95% confidence interval: 1.67–9.58).
-
After conducting a bias analysis to account for potential inaccuracies in self-reported data, the association remained, though it was somewhat less pronounced. The adjusted analysis showed that rates of gonorrhea were still higher among PrEP users, with a median incidence rate ratio of 2.36 (simulation interval: 1.08–5.06).
-
There was no significant increase in the rates of chlamydia or syphilis among PrEP users.
-
19 interviews were analyzed. Participants averaged 54 years old, and 53% were female. Most participants were infected with COVID-19 for the first time in 2020 (32%) or 2021 (47%).
-
Patient Expectations: Participants described two categories of expectations: those for their practitioners and those for treatment. Patients expected their primary care practitioners to be knowledgeable about post-COVID conditions, attentive to their individual condition, and to engage in collaborative processes for treatment.
-
Patient Experiences: Patients described two types of experiences. First, interactions with practitioners were perceived as positive when practitioners were honest and validating, and negative when patients felt dismissed or discouraged. Second, patients described challenges navigating the fragmented U.S. health care system when coordinating care, treatment and testing, and payment.
-
There was no significant difference in weight loss between patients in the GEM intervention and those in EUC at 12 months.
-
Participants in the GEM group reported a significant increase in weekly physical activity compared to those in the EUC group.
-
Attendance at weight management programs like MOVE! or DPP did not significantly differ between the GEM and EUC groups.
-
While more frequent health coaching calls were associated with greater weight loss, overall patient engagement with coaching was low.
-
The most common forms of scholarly output were letters to the editor, case reports, and population health projects.
Why It Matters: Individuals who choose to take PrEP are at higher risk for gonorrhea and should be regularly tested and treated to manage this risk effectively. The findings of this study highlight the importance of investing in sexually transmitted infection testing, risk reduction, secondary prevention measures such as Doxycycline Post-Exposure Prophylaxis (a preventive treatment to reduce the risk of bacterial STIs after potential exposure), surveillance, and partner management alongside PrEP to reduce bacterial STI transmission effectively. This approach is necessary regardless of whether the increased risk is due to pre-existing factors or potential behavior changes associated with PrEP use.
Nguyen K. Tran, PhD, MPH, et al
Department of Epidemiology and Biostatistics, Drexel University Dornsife School of
Public Health, Philadelphia, Pennsylvania
Stanford University School of Medicine, Palo Alto, California
Original Research
Disconnect Between Expectations and Care: Long COVID Patients Seek Better Collaboration
with Health Care Providers
Background and Goal: Post-COVID-19 Conditions or “long COVID,” is defined as the continuation or development
of new symptoms three months after initial SARS-CoV-2 infection, with symptoms lasting
at least two months with no other explanation. For many patients with long COVID,
primary care is the first point of interaction with the health care system. Beyond
patients’ expressions of stigmatization and disempowerment, less is known about their
perspectives and expectations for the quality of long COVID care overall. This study
aimed to examine the expectations and experiences of primary care patients seeking
treatment for long COVID.
Study Approach: Twenty interviews were conducted between 2022 and 2023 with primary care patients
from a long COVID triage clinic at the University of Utah. A phenomenological framework,
which focuses on understanding and describing participants’ lived experiences and
perceptions through open-ended, flexible questioning, guided the analysis. The semistructured
interviews were recorded, transcribed, and analyzed using inductive qualitative content
analysis, a method for identifying themes and patterns in the data.
Main Results:
-
19 interviews were analyzed. Participants averaged 54 years old, and 53% were female. Most participants were infected with COVID-19 for the first time in 2020 (32%) or 2021 (47%).
-
Patient Expectations: Participants described two categories of expectations: those for their practitioners and those for treatment. Patients expected their primary care practitioners to be knowledgeable about post-COVID conditions, attentive to their individual condition, and to engage in collaborative processes for treatment.
-
Patient Experiences: Patients described two types of experiences. First, interactions with practitioners were perceived as positive when practitioners were honest and validating, and negative when patients felt dismissed or discouraged. Second, patients described challenges navigating the fragmented U.S. health care system when coordinating care, treatment and testing, and payment.
Why It Matters: The study results highlight a disconnect between the expectations and experiences of long-COVID patients within the U.S. health care system. Despite facing numerous barriers and frustrations, patients show a desire to collaborate with their health care providers to improve treatment outcomes. Primary care practitioners and other health care professionals can better align patients’ experiences with their expectations by listening to their concerns, validating their symptoms, and advocating for their needs. These actions are essential for delivering patient-centered, effective care, and ultimately improving health outcomes for long COVID patients.
Elena Gardner, MPH, et al
University of Utah Family and Preventive Medicine, Salt Lake City, Utah
Visual abstract showcasing key findings from this study:
_____________________________________________________________________________________
Original Research
Technology-Assisted Health Coaching Intervention Does Not Improve Weight Loss in Veterans
and High-Risk Patients
Background and Goal: Obesity is a significant health issue, particularly among veterans and racial/ethnic
minority groups, who experience higher rates of obesity-related health problems. Primary
care is a key setting for addressing obesity, but many barriers, including time constraints
and limited patient engagement, make effective treatment challenging. This study aimed
to evaluate whether a technology-assisted health coaching intervention called Goals
for Eating and Moving (GEM) could help high-risk patients lose weight more effectively
than enhanced usual care (EUC).
Study Approach: Researchers conducted a two-arm, cluster-randomized controlled trial involving 19
primary care teams across two health care systems. Patients with obesity or overweight
conditions and related comorbidities were randomized to receive either the GEM intervention
or EUC. The GEM intervention included one in-person and up to 12 telephone-delivered
coaching sessions. Coaches supported goal setting and weight management program engagement,
facilitated by a software tool and motivational interviewing. Patients randomized
to EUC received educational handouts. The study measured weight changes and other
health outcomes over 12 months.
Main Results:
-
There was no significant difference in weight loss between patients in the GEM intervention and those in EUC at 12 months.
-
Participants in the GEM group reported a significant increase in weekly physical activity compared to those in the EUC group.
-
Attendance at weight management programs like MOVE! or DPP did not significantly differ between the GEM and EUC groups.
-
While more frequent health coaching calls were associated with greater weight loss, overall patient engagement with coaching was low.
Why It Matters: The findings of this study highlight the complexities of managing obesity in high-risk
populations and the limitations of relying solely on technology-assisted health coaching
in primary care settings. More comprehensive approaches are needed to effectively
support weight management. Integrating lifestyle interventions with medical treatments
and addressing social determinants of health are important steps to improve patient
outcomes in these populations.
Melanie R. Jay, MD, MS, et al
Department of Medicine, New York University Grossman School of Medicine, New York,
New York
Department of Population Health, New York University Grossman School of Medicine,
New York, New York
New York Harbor Veterans Health Affairs, New York, New York
____________________________________________________________________________
Original Research
Underrepresented in Medicine Family Physicians Have Critical Role in the Care of Medicaid
Patients
Background and Goal:While underrepresented in Medicine (URiM) physicians are a key to better health outcomes
for minority patients, the proportion of URiM physicians — such as Black, Hispanic/Latino,
and Native American physicians remains low in the U.S. health care system. This study
examines the diversity of the family physician workforce that cares for Medicaid beneficiaries
by linking a unique dataset containing information on family physicians’ race and
ethnicity to national-level Medicaid claims data.
Study Approach:Researchers analyzed data from 13,096 family physicians across 44 states, using 2016
Medicaid claims data from the Transformed Medicaid Statistical Information System
(T-MSIS) and 2016-17 American Board of Family Medicine certification questionnaire
responses. The diversity Family Physicians’ Medicaid patient panel and whether they
saw at least 150 beneficiaries in 2016 was examined.
Main Results:
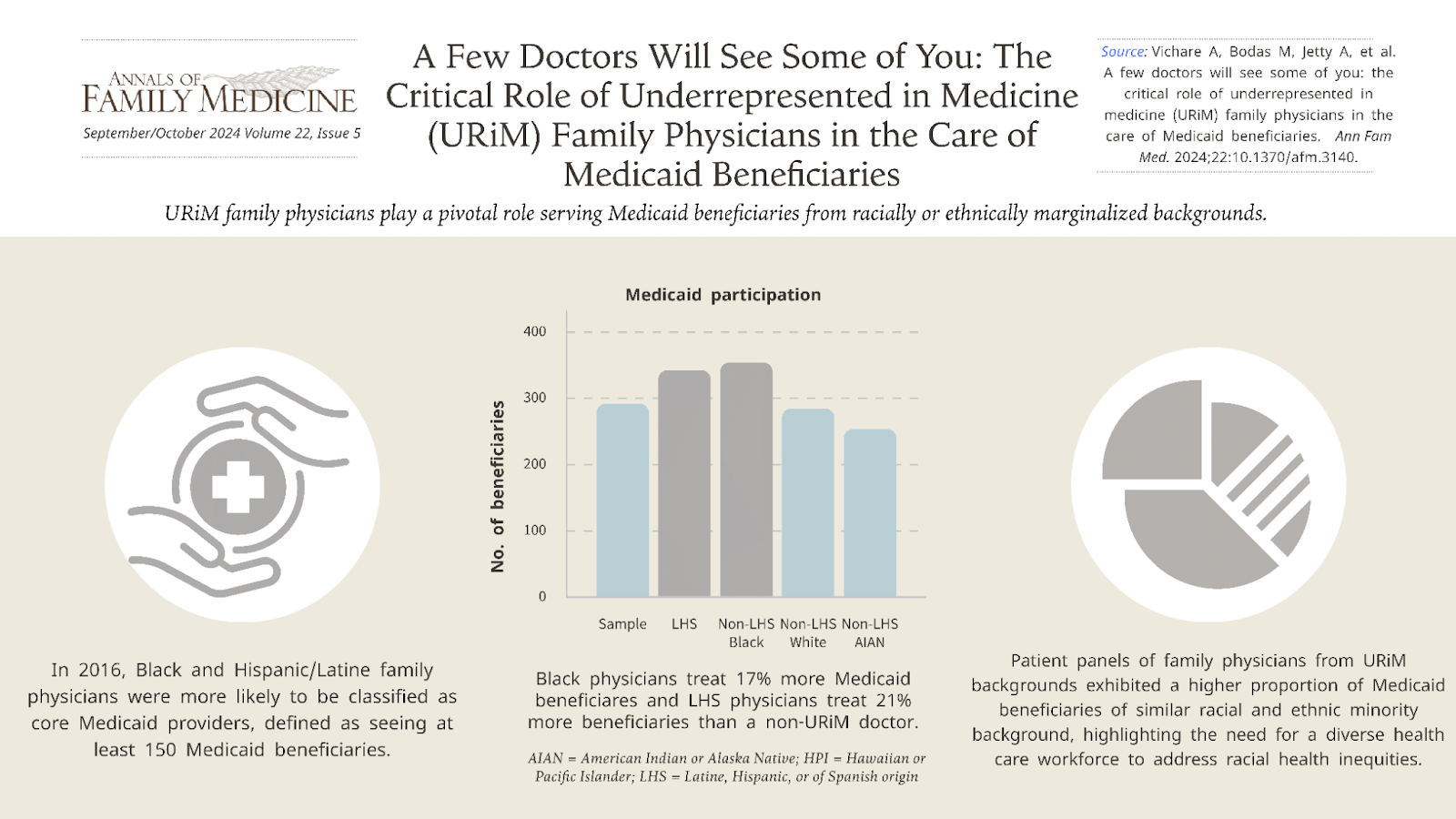
• URiM family physicians, particularly Black and Hispanic/Latino family physicians, are significantly more likely to participate in Medicaid by treating a substantial number of Medicaid patients.
• Black and Hispanic/Latino family physicians were more likely to be core Medicaid providers defined as seeing at least 150 beneficiaries in 2016.
• The patient panels of URiM family physicians had a much higher proportion of Medicaid beneficiaries from racial and ethnic minorities.
Why It Matters:The findings of this study suggest physician race and ethnicity are correlated with Medicaid participation, emphasizing the need to continue efforts to diversify the health care workforce. Policies need to address pipeline problems in medical education, including failures to recruit, nurture and retain URiM students.
Anushree Vichare, PhD, MBBS, MPH, et al
Fitzhugh Mullan Institute for Health Workforce Equity, Department of Health Policy
and Management, Milken Institute School of Public Health, The George Washington University,
Washington, DC
Visual abstract showcasing key findings from this study:
____________________________________________________________________________
Original Research
Strong Infrastructure Associated With Scholarly Activity in Family Medicine Residency
Programs
Background and Goal:Family medicine residency programs are essential for training future primary care
physicians. The current Accreditation Council for Graduate Medical Education (ACGME)
program requirement for scholarly activity was last revised in 2019 and requires family
medicine residents to perform two scholarly projects; one must be a quality improvement
(QI) project and the second project type is at the program's discretion. This study
aimed to assess the scholarly activity output of family medicine residency programs
in the U.S., identify institutional factors associated with increased scholarly activity,
and determine how well these programs meet ACGME standards.
Study Approach: The study surveyed family medicine residency program directors from across the U.S.
to gather data on their programs’ scholarly activity. The survey covered various aspects,
including the types of scholarly work produced by residents, the availability of resources
such as faculty mentorship and access to Institutional Review Boards (IRB), and how
often residents exceeded the minimum scholarly activity requirements. The study also
classified scholarly activities into four categories based on Boyer’s Domains of Scholarship:
discovery, application, integration, and teaching.
Main Results:298 program directors completed the survey.
• More than one-half of the program directors reported that fewer than 25% of their residents performed more scholarly activity than ACGME minimum requirements.
-
The most common forms of scholarly output were letters to the editor, case reports, and population health projects.
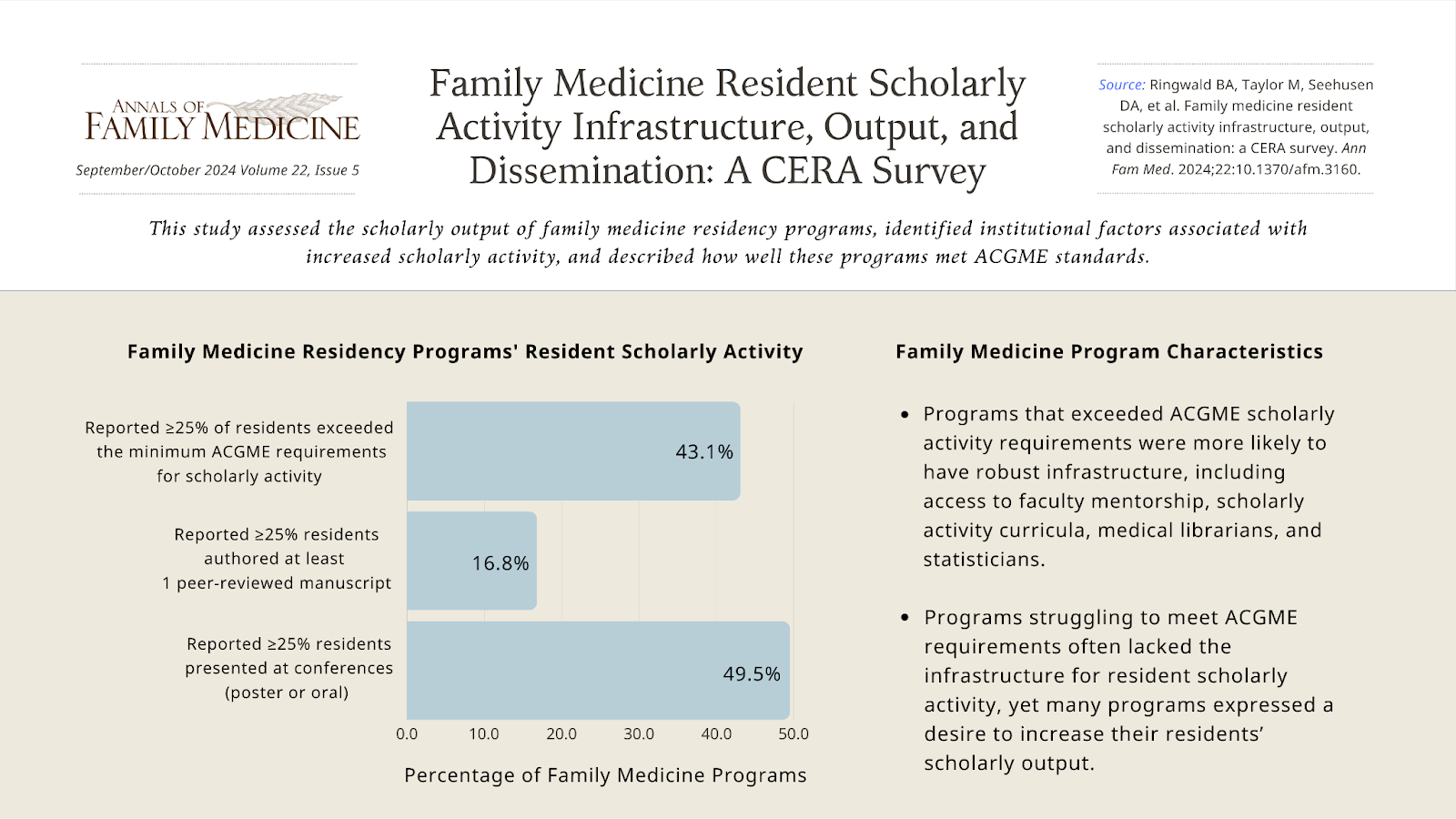
• Only 16.9% of programs reported that more than 25% of their residents published peer-reviewed manuscripts. However, 49.6% reported that over 25% of residents presented their work at conferences, with poster presentations being more common than oral presentations.
• Programs that exceeded ACGME scholarly activity requirements were more likely to have robust infrastructure, including access to faculty mentorship, scholarly activity curricula, IRB, medical librarians, and statisticians.
• Programs struggling to meet ACGME requirements often lacked the necessary infrastructure to support resident scholarly activity. Despite this, many programs expressed a desire to increase their residents’ scholarly output.
Why It Matters:Residency programs that provide strong support for scholarly activity not only help residents meet ACGME requirements but also prepare them for future challenges in their medical careers. Ensuring that all family medicine residency programs have access to essential resources—such as mentorship, research support, and technical assistance—is important for increasing scholarly output. Establishing these infrastructure requirements can also help address disparities in funding and research productivity among programs.
Family Medicine Resident Scholarly Activity Infrastructure, Output, and Dissemination: A CERA Survey
Bryce A. Ringwald, MD, et al
OhioHealth Riverside Methodist Hospital Family Medicine Residency Program, Columbus,
Ohio
Visual abstract showcasing key findings from this study:
___________________________________________________________________________
Original Research
A Blood Pressure Control Intervention Including Remote Monitoring Doubles Success
Among Underserved Patients
Background and Goal:Underserved communities are at higher risk for uncontrolled high blood pressure, or
hypertension, which can lead to heart disease and higher death rates. Digital health
technologies, such as remote monitoring, offer new ways to manage these chronic conditions.
This study, conducted between August and December 2021, evaluated the impact of a
remote monitoring program called DIG IT on blood pressure control in underserved patients
at a Federally Qualified Health Center (FQHC) in Orange County, California.
Study Approach:Researchers compared two groups: patients using the DIG IT program, which includes
digital blood pressure monitoring, medication management, and a team-based care approach,
and a historical control group that received standard care without digital tools.
The study focused on patients aged 40 and older with uncontrolled hypertension. A
total of 140 patients (70 DIG IT, 70 historical control) were included. Blood pressure readings and heart disease risk scores were tracked over three months
to evaluate the program’s effectiveness.
Main Findings:
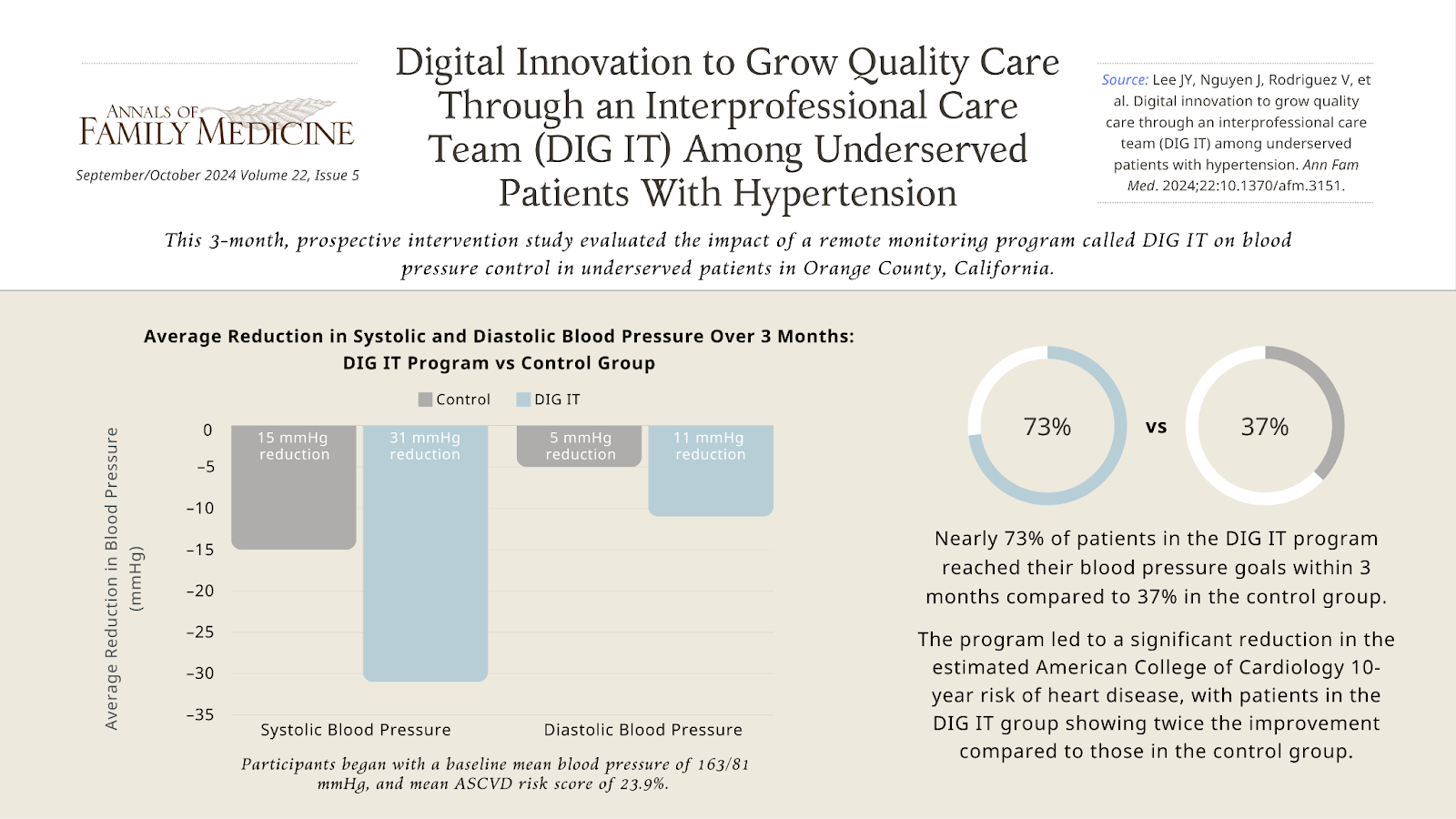
• Patients in the DIG IT program saw their systolic blood pressure (the top number, measuring pressure when the heart beats) drop by an average of 31 points, compared to just 15 points in the control group. Diastolic blood pressure (the bottom number, measuring pressure when the heart is at rest) decreased by 11 points in the DIG IT group, compared to a 5-point reduction in the control group.
• The program led to a significant reduction in the estimated American College of Cardiology 10-year risk of heart disease, with patients in the DIG IT group showing twice the improvement compared to those in the control group.
• Nearly 73% of patients in the DIG IT program reached their blood pressure goals within three months, compared to 37% in the control group.
Why It Matters:These findings show that remote monitoring programs, like DIG IT, can significantly improve blood pressure control and lower heart disease risks in underserved communities. By connecting digital health tools with real-time care, these programs provide timely interventions that are crucial for managing chronic diseases. Expanding access to such innovative care models in underserved areas is key to reducing health disparities and improving overall public health.
Joyce Y. Lee, PharmD, APh, BCPS, BCACP, CDCES, et al
School of Pharmacy and Pharmaceutical Sciences, University of California, Irvine,
California
University of California Irvine Health Family Health Center, Irvine, California
Visual abstract showcasing key findings from this study:
_____________________________________________________________________________________
Systematic Review
High-Sensitivity Troponin Shows Promise in Diagnosing Acute Coronary Syndrome In Primary
Care Settings
Background and Goal:Chest pain is a common but challenging symptom for general practitioners to evaluate,
as it can be caused by both serious conditions like acute coronary syndrome, which
includes heart attacks, and more benign issues. Accurately identifying acute coronary
syndrome is critical to prevent unnecessary hospital referrals and reduce health care
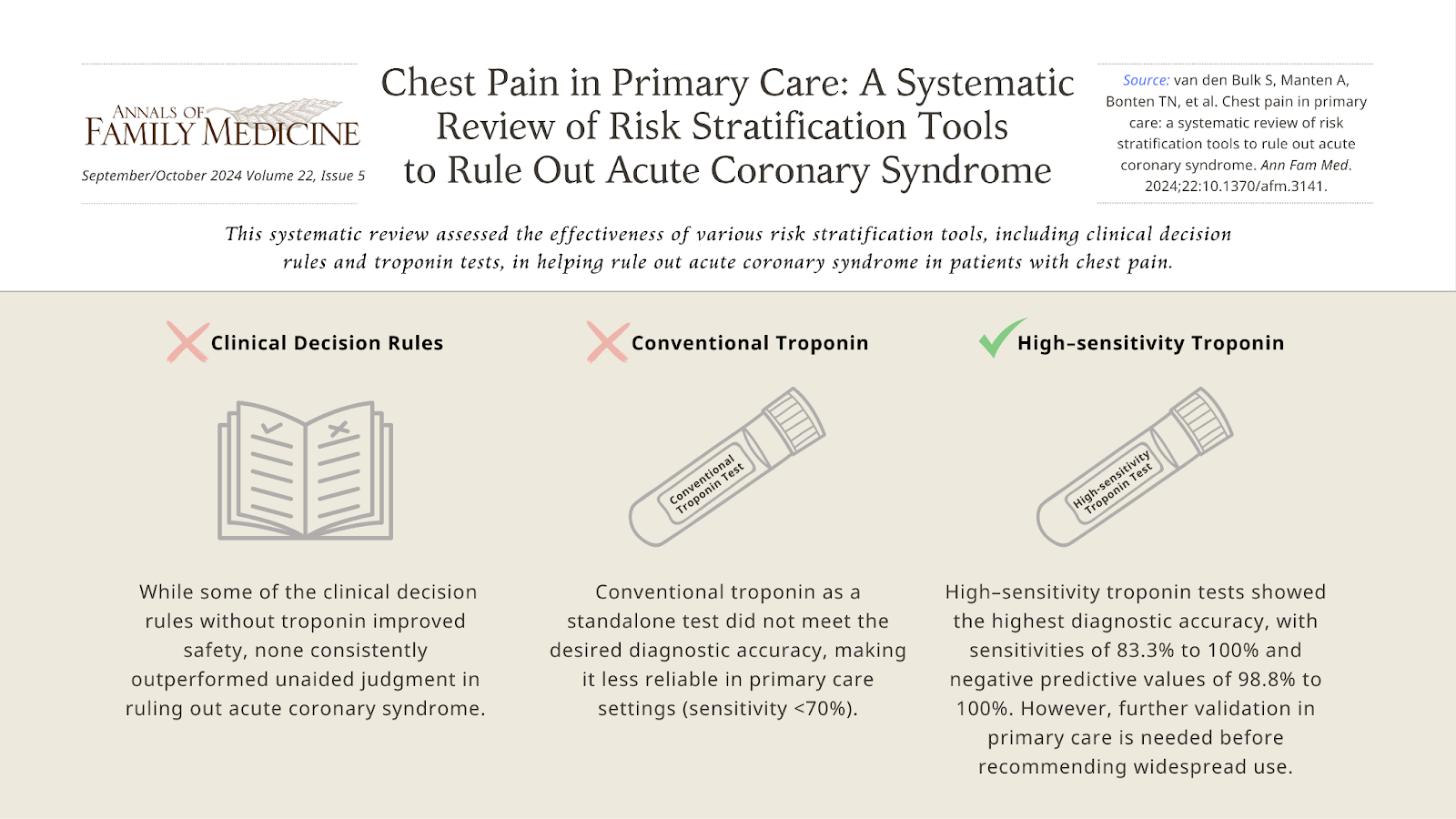
costs. This study aimed to assess the effectiveness of various risk stratification
tools, including clinical decision rules and troponin tests, in helping general practitioners
rule out acute coronary syndrome in patients with chest pain.
Study Approach: Researchers conducted a systematic review of studies involving adult patients presenting
with chest pain in primary care settings. The review included studies that examined
the diagnostic accuracy of different clinical decision rules and troponin point-of-care
tests, both conventional and high-sensitivity, in identifying acute coronary syndrome.
The study compared these tools to the unaided clinical judgment of general practitioners.
Main Findings:14 studies out of 1,204 screened were included in the final review.
• While some of the clinical decision rules without troponin improved safety, none consistently outperformed unaided general practitioner judgment in ruling out acute coronary syndrome.
• Conventional troponin as a standalone test did not meet the desired diagnostic accuracy, making them less reliable in primary care settings.
• High-sensitivity troponin (hs-troponin) tests demonstrated the highest diagnostic accuracy. However, this finding requires further prospective validation in primary care before it can be recommended for widespread use.
Why It Matters:Although high-sensitivity troponin tests hold promise, they are not yet ready to replace clinical judgment or be used independently in primary care settings without further validation. The best diagnostic accuracy might be achieved by combining general practitioners’ risk assessments with these stratification tools, rather than using them as standalone tests. Ensuring the accuracy, additional value and validation of these tools is essential for improving patient outcomes and reducing unnecessary health care costs.
Simone van den Bulk, MD, et al
Department of Public Health and Primary Care, Leiden University Medical Center, Leiden,
The Netherlands
Visual abstract showcasing key findings from this study:
Original Research
Family Physicians Associated With Lower Cesarean Rates and Higher Culture of Safety
in Rural Hospitals
Background and Goal:The U.S. is currently experiencing a maternal health crisis, particularly in rural
areas where access to pregnancy care is diminishing. This issue is compounded by rising
rates of severe maternal morbidity and mortality. Family physicians often fill critical
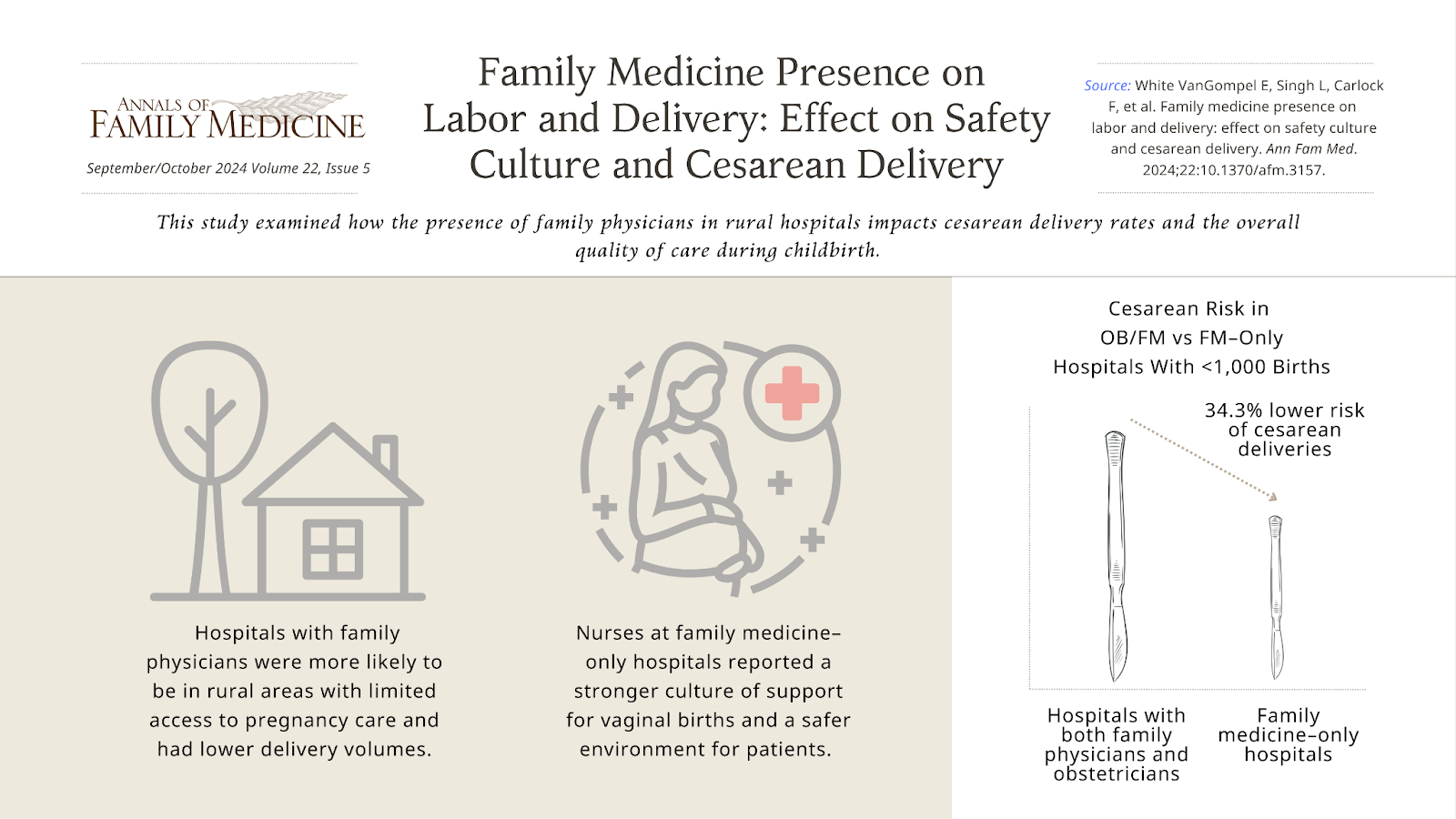
gaps in care in rural areas where obstetricians are scarce. This study aimed to examine
how the presence of family physicians in rural hospitals impacts cesarean delivery
rates and the overall quality of care during childbirth.
Study Approach:The study analyzed data from rural hospitals in Iowa. Researchers collected survey
responses from clinicians including nurses, obstetricians, and family physicians,
about their attitudes and practices related to childbirth. These responses were linked
with hospital data on cesarean delivery rates, patient demographics, and other factors.
The study compared hospitals where only family physicians provide care, hospitals
with both family physicians and obstetricians, and hospitals with only obstetricians.
Main Results:A total of 849 clinicians from 39 hospitals completed the survey: 13 family medicine-only, 11 obstetrician-only, and 15 hospitals with both. All family medicine-only hospitals were rural with fewer than 1,000 annual births.
• Among hospitals with fewer than 1,000 annual births, births at family medicine–only hospitals had a 34.3% lower risk of cesarean deliveries compared to hospitals with both family physicians and obstetricians.
• Nurses at family medicine-only hospitals reported a stronger culture of support for
vaginal births and a safer environment for patients.
• Hospitals with family physicians were more likely to be in rural areas with limited
access to pregnancy care and had lower delivery volumes.
Why It Matters:Family physicians play an important role in providing high-quality pregnancy care in rural areas, where access to specialized obstetric care is limited. The findings of this study suggest that family physicians contribute to lower cesarean delivery rates and a supportive culture for vaginal births, which are key indicators of maternal care quality. Ensuring that family physicians continue to be trained and supported in providing pregnancy care is vital for maintaining and improving maternal health outcomes in underserved rural communities.
Family Medicine Presence on Labor and Delivery: Effect on Safety Culture and Cesarean Delivery
Emily White VanGompel, MD, MPH, et al
Department of Family and Community Medicine, University of Illinois at Chicago College
of Medicine, Chicago, Illinois
Visual abstract showcasing key findings from this study:
_____________________________________________________________________________________
Research Brief
Transparent Capsules in Dry Powder Inhalers Significantly Improve Medication Delivery
Background and Goal: This study examined whether using a transparent capsule in single-dose dry powder
inhalers for patients with non-reversible chronic airway disease affects the amount
of medication delivered. The goal was to determine if patients who use transparent
capsules, which allow them to see if the medication has been fully inhaled, have better
inhalation results compared to those using opaque capsules.
Study Approach: Researchers conducted an observational cross-sectional study at a tertiary university
hospital. The study involved 91 patients using long-acting bronchodilators with single-dose
dry powder inhalers for chronic airway disease. Patients were asked to use their inhalers
under supervision, and the weight of the capsule was measured before and after inhalation
to assess how much of the medication was delivered. The study was conducted between
October 2020 and October 2022.
Main Results:
• Patients using transparent capsules had a significant decrease in capsule weight after inhalation, with a 30.1% reduction compared to an 8.6% reduction for opaque capsules, indicating more medication was delivered.
• The change in capsule weight was consistent regardless of the severity of the patient’s airway disease.
Why It Matters: The findings suggest that using transparent capsules in dry powder inhalers could
improve medication delivery by providing patients with visual feedback on their inhalation
technique. This could lead to better management of chronic airway diseases by ensuring
that patients receive their full dose of medication. Given the high importance patients
place on verifying correct medication intake, these results reinforce the need for
inhalation devices that support effective use.
Evaluation of the Importance of Capsule Transparency in Dry Powder Inhalation Devices
Jose Luis López-Campos, MD, et al
Unidad Médico-Quirúrgica de Enfermedades Respiratorias. Instituto de Biomedicina de
Sevilla (IBiS), Hospital Universitario Virgen del Rocío/ Universidad de Sevilla, Seville,
Spain
Centro de Investigación Biomédica en Red de Enfermedades Respiratorias (CIBERES). Instituto de Salud Carlos III, Madrid, Spain
_____________________________________________________________________________________
Research Brief
Lack of Knowledge of Antibiotic Risks Contributes to Primary Care Patients’ Expectations
of Antibiotics for Common Symptoms
Background and Goal:Patient expectations of receiving antibiotics for common symptoms can trigger unnecessary
use, contributing to antibiotic resistance and other health risks. This study examined
the prevalence of patient antibiotic expectations for common symptoms. It also compared
these expectations between patients in public and private health care settings and
identified factors that influenced patients’ expectations of getting antibiotics for
these symptoms.
Study Approach:This study surveyed 564 primary care patients in Texas between January 2020 and June
2021 across public and private clinics. The survey assessed patients’ expectations
for antibiotics when experiencing five common symptoms—diarrhea, sore throat, cold/flu,
sinus infections, and bronchitis—and their knowledge of the risks associated with
antibiotic use. Researchers also examined how factors like education and health literacy
affected these expectations.
Main Results:Over 93% of the patients surveyed expected antibiotics for at least one of the five
common symptoms. Public clinic patients were nearly twice as likely to expect antibiotics
for sore throat, diarrhea, and cold/flu compared to those in private clinics. Lack
of knowledge about the potential risks of antibiotics was linked to higher expectations
for receiving antibiotics for diarrhea and cold/flu symptoms. Patients with lower
education levels and inadequate health literacy were more likely to expect antibiotics
for diarrhea.
Why It Matters: To reduce unnecessary antibiotic use, future efforts should educate patients on when antibiotics are truly needed and emphasize potential risks. The authors of the study are currently developing a tool to help patients and clinicians discuss appropriate antibiotic use and explore non-antibiotic treatments.
Lindsey A. Laytner, PhD, MPH, et al
Department of Family and Community Medicine, Baylor College of Medicine, Houston,
Texas
Center for Innovations in Quality, Effectiveness, and Safety, Michael E. DeBakey Veterans Affairs Medical Center, Houston, Texas
Special Report
Adapting Opioid Treatment Research Amid COVID-19: The Resilient Journey of the HOMER Study
Background and Goal: The HOMER study was launched to determine the most effective setting for starting buprenorphine treatment for opioid use disorder. Originally designed as a randomized trial comparing home-based versus office-based inductions, the study faced significant challenges due to the COVID-19 pandemic. These included shifts in health care delivery, changes in patient preferences, and the emergence of new practices like telehealth. The goal was to adapt the study to these unprecedented circumstances while maintaining its focus on patient-centered care and effective treatment outcomes.
Key Insights:The HOMER study had to quickly adapt to the unprecedented challenges brought on by the COVID-19 pandemic. Researchers could have made decisions regarding study design purely from a methodological perspective, but they chose to engage the community in decision making. With community input, the study design evolved to include a third arm, telehealth, in response to the rapid shift in health care delivery methods. As the study progressed, it became clear that both patients and clinicians had strong preferences for specific induction methods. This led to an additional significant change in the study’s design, shifting from a purely randomized approach to a comprehensive cohort design. This change allowed the study to accommodate patients who preferred not to be randomized. Despite the numerous challenges, including recruitment delays and shifts in health care priorities, the HOMER study persisted. As of January 2024, HOMER has enrolled nearly 300 study participants, and practices are still participating.
Why It Matters:The experiences and adaptations of the HOMER study shows how research can remain resilient and responsive in the face of unforeseen challenges. Flexibility in research design and active engagement with patients, clinicians, and community advisors can keep studies relevant and patient-centered. The challenges overcome by the research team offer valuable lessons for other researchers, highlighting the importance of adaptability, collaboration, and perseverance in achieving meaningful outcomes, particularly in fields like opioid use disorder treatment.
Linda Zittleman, MSPH, et al
University of Colorado Department of Family Medicine, Aurora, Colorado
_____________________________________________________________________________________
Innovations In Primary Care
Collaborative Program Between University and Clinic Boosts General Practitioner Recruitment
in Deprived Areas of Yokohama, Japan
The “Deep End Kawasaki/Yokohama” program in Japan addresses the critical challenge of recruiting and retaining general practitioners in resource-deprived areas by adapting a model originally developed in Scotland. Launched in 2023 in a socially deprived district of Yokohama, the program establishes a collaboration between a local clinic and a university, both funded by the city. This partnership has successfully increased the number of general practitioners from one to eight, enhancing clinical care, education, and research opportunities. The program also includes innovative community engagement activities for medical students and trainees, aimed at fostering empathy and diverse perspectives. The initiative demonstrates a sustainable approach to improving health care delivery in underserved areas and offers a potential model for similar programs in other countries.
Deep End Kawasaki/Yokohama: A New Challenge for GPs in Deprived Areas in Japan
Makoto Kaneko, MD, MClinSci, PhD, et al
Department of Health Data Science, Yokohama City University, Yokohama, Japan
Yokohama Kotobuki-cho Health and Welfare Exchange Center Clinic, Yokohama, Japan
Innovations in Primary Care
Improving Disability Assessments for Citizenship: Boston Clinic’s Embedded Neuropsychological Program Helps Immigrants
To improve access to specialized disability assessments for U.S. citizenship applicants with cognitive and psychiatric conditions, a primary care clinic at Boston Medical Center’s Immigrant and Refugee Health Center implemented an innovative embedded neuropsychological assessment program. This program supports primary care providers by offering specialized evaluations for patients seeking a Medical Certification for Disability Exception (Form N-648), which is necessary for naturalization. The initiative included cognitive screening tools, direct referrals for neuropsychological assessments, and a multidisciplinary team approach. Over two years, the program provided crucial assessments to 34 patients, with 36% qualifying for N-648 forms through specialized testing despite initially normal cognitive screenings. This innovation highlights the value of integrating neuropsychological services within primary care.
Joelle T. Taknint, PhD, et al
Boston University Chobanian & Avedisian School of Medicine, Boston, Massachusetts
Immigrant & Refugee Health Center, Boston Medical Center, Boston, Massachusetts
_____________________________________________________________________________________
Innovations in Primary Care
EHR Messaging Strengthens Patient-Physician Connection Before First Visit
Inspired by the VA’s My Life, My Story project, this initiative used the electronic health record (EHR) to strengthen the patient-physician relationship by inviting patients to share personal narratives before their first visit with a new primary care physician. Conducted at a regional clinic affiliated with the University of Wisconsin, the project involved sending secure messages to patients, asking them to describe what they wanted their health care team to know about them as a person. The majority of patients responded positively, with some sharing deeply personal information that may not have surfaced during a typical clinical encounter. The study physician reported that these narratives fostered a stronger connection with patients, facilitated more effective agenda setting, and improved the overall efficiency of the visit.
Samantha Barbour, et al
University of Wisconsin School of Medicine and Public Health, Madison, Wisconsin
_____________________________________________________________________________________
Essay
How Trust and Teamwork Kept a Physician from Walking Away
Background:Family medicine is demanding, often taking an emotional toll on physicians as they share in the distress and trauma of their patients. The essay recounts a moment when a family physician, overwhelmed by the complexities of patient care, felt ready to walk away from her duties.
Key Argument:The essay highlights the important role of trust and teamwork in health care settings. When the physician reached out to a team nurse for support, the nurse’s encouragement helped her regain focus and continue caring for her patients. This interaction underscores the strength that health care professionals can draw from one another in moments of vulnerability.
Why It Matters:This story illustrates how the emotional support and solidarity within health care teams can be a powerful antidote to burnout, helping professionals navigate the challenges of patient care. The essay advocates for a work environment where such connections are nurtured, ultimately leading to better patient care and a more resilient health care workforce.
The Day I Almost Walked Away: Trust, Gratitude, and the Power of Teamwork
Colleen T. Fogarty, MD, MSc, et al
Department of Family Medicine, University of Rochester School of Medicine and Dentistry,
Rochester, New York
University of Rochester Medical Center, Rochester, New York
An accompanying episode of the Annals of Family Medicine podcast, featuring Dr. Fogarty and Ms. Schiano, RN, reading their essay aloud, will
be available at 5 p.m. on Sept. 23 here.
Essay
Adding ‘Contiguity’ as a Fifth Core Tenet: The Irreplaceable Value of Face-to-Face
Care in Primary Care
Background:In the early 1990s, Barbara Starfield identified four core tenets of primary care:
first contact, comprehensiveness, coordination, and continuity. However, in today’s
rapidly advancing digital world, where telehealth and artificial intelligence are
becoming more prevalent, the role of physical presence in patient care is being questioned.
Key Argument:This essay argues for the addition of a fifth tenet, “Contiguity,” which highlights
the importance of face-to-face interactions in primary care. Contiguity refers to
the physical proximity between a patient and their clinician, which is essential for
building trust, conducting thorough physical exams, and fostering genuine relationships.
The essay contends that although technology can improve many aspects of care, it cannot
replace the unique human connection that occurs when patients and clinicians are physically
present with one another.
Why It Matters:As health care continues to evolve with digital innovations, it’s important to articulate the value of physical face-to-face interactions in primary care. By naming contiguity as a core tenet of primary care, health care systems, academic primary care departments, and other policy-generating institutions will be held accountable to ensure that clinicians do not lose sight of this foundational component of patient-clinician relationships. Contiguity ensures care remains deeply personal, trusting, and empathic.
Jennifer Y. C. Edgoose, MD, MPH, et al
Department of Family Medicine and Community Health, University of Wisconsin School
of Medicine and Public Health, Madison, Wisconsin
____________________________________________________________________________
Editorial
Family Physicians Play a Vital Role in Improving Maternal Health and Safety in Obstetrics
Background: Pregnancy and childbirth in the U.S. are more dangerous than in any other high-income
country, with particularly high risks for Black individuals and those in rural areas.
To address this, the American Academy of Family Physicians (AAFP) and the White House
have called for expanding and diversifying the perinatal workforce, including training
family physicians to provide critical pregnancy care, especially in rural and underserved
communities.
Key Argument: Building on research by VanGompel et al., which found that nurses on labor and delivery
units had a more favorable attitude about the safety culture and practices that support
lower cesarean section rates in hospitals where family medicine physicians provided
labor and delivery care, the author argues that family physicians significantly improve
the quality of obstetric care through their specialized training. Family medicine
residencies emphasize interprofessional teamwork, communication, and continuity of
care, and frequently include the completion of the AAFP’s Advanced Life Support in
Obstetrics (ALSO) course, which improves skills in handling obstetric emergencies.
These aspects of their training enable family physicians to foster a strong safety
culture and deliver care on par with specialists. The editorial calls for policy changes
such as health system credentialing to increase family physicians’ involvement in
obstetric care and training reforms to prepare the health workforce to improve maternal
outcomes.
Why It Matters:Family physicians are uniquely trained to lead interprofessional pregnancy care teams that promote a safety culture and improve health outcomes. As new training models are developed to support this vision, it is important not only to focus on patient care skills in pregnancy care but also the critical skills for leading and being included in interprofessional teams needed to provide comprehensive pregnancy care.
Family Medicine Obstetrics: Answering the Call
Wendy B. Barr, MD, MPH, MSCE,
Department of Medicine, UMass Chan Lahey Regional Medical Campus, Burlington, Massachusetts
Department of Family Medicine, Tufts University School of Medicine, Boston, Massachusetts
Mario P. DeMarco, MD, MPH
Department of Family Medicine and Community Health, Perelman School of Medicine, University
of Pennsylvania School of Medicine, Philadelphia, Pennsylvania
# # #
Annals of Family Medicine is a peer-reviewed, indexed research journal that provides a cross-disciplinary forum for new, evidence-based information affecting the primary care disciplines. Launched in May 2003, Annals is sponsored by seven family medical organizations, including the American Academy of Family Physicians, the American Board of Family Medicine, the Society of Teachers of Family Medicine, the Association of Departments of Family Medicine, the Association of Family Medicine Residency Directors, the North American Primary Care Research Group, and The College of Family Physicians of Canada. Annals is published six times each year and contains original research from the clinical, biomedical, social and health services areas, as well as contributions on methodology and theory, selected reviews, essays and editorials. Complete editorial content and interactive discussion groups for each published article can be accessed free of charge on the journal’s website, www.AnnFamMed.org.
Media Contact: Julie Hirschhorn
Annals of Family Medicine
jhirschhorn{at}aafp.org