
Abstract
PURPOSE Recent efforts to encourage meaningful use of electronic health records (EHRs) assume that widespread adoption will improve the quality of ambulatory care, especially for complex clinical conditions such as diabetes. Cross-sectional studies of typical uses of commercially available ambulatory EHRs provide conflicting evidence for an association between EHR use and improved care, and effects of longer-term EHR use in community-based primary care settings on the quality of care are not well understood.
METHODS We analyzed data from 16 EHR-using and 26 non–EHR-using practices in 2 northeastern states participating in a group-randomized quality improvement trial. Measures of care were assessed for 798 patients with diabetes. We used hierarchical linear models to examine the relationship between EHR use and adherence to evidence-based diabetes care guidelines, and hierarchical logistic models to compare rates of improvement over 3 years.
RESULTS EHR use was not associated with better adherence to care guidelines or a more rapid improvement in adherence. In fact, patients in practices that did not use an EHR were more likely than those in practices that used an EHR to meet all of 3 intermediate outcomes targets for hemoglobin A1c, low-density lipoprotein cholesterol, and blood pressure at the 2-year follow-up (odds ratio = 1.67; 95% CI, 1.12–2.51). Although the quality of care improved across all practices, rates of improvement did not differ between the 2 groups.
CONCLUSIONS Consistent use of an EHR over 3 years does not ensure successful use for improving the quality of diabetes care. Ongoing efforts to encourage adoption and meaningful use of EHRs in primary care should focus on ensuring that use succeeds in improving care. These efforts will need to include provision of assistance to longer-term EHR users.
- medical record system
- computerized
- diabetes mellitus
- quality of health care
- primary health care
- electronic medical records
- electronic health records
- practice-based research
INTRODUCTION
Encouraging the adoption of electronic health records (EHRs) in primary care settings has been an objective of federal health policy since 2004, when the Bush administration set the goal of universal EHR use within 10 years. Since that time, the use of EHR technology has been identified as a central component of the patient-centered medical home model endorsed by primary care professional organizations in the United States.1,2 Through passage of the Health Information Technology for Economic and Clinical Health (HITECH) Act in 2009, Congress and the Obama administration have reaffirmed the objective of increasing adoption of ambulatory care EHRs. HITECH includes incentives for physicians to implement and “meaningfully use” EHR technology, and has funded Regional Extension Centers (RECs) to assist care providers in meeting these objectives.3,4 Underlying these policy developments is the assumption that EHR use, if meaningful, will improve the safety, quality, and efficiency of the US health care system.
The official definition of meaningful use includes a variety of functional objectives, but Karsh et al5,6 have argued that the true measure of successful use of HIT is in its impact on population health. Few studies outside of those conducted by a small number of leading organizations have demonstrated that typical use of commercially available EHRs in ambulatory settings is associated with improvements in the quality of care, however, and recent research has found that more advanced features of EHRs expected to improve the delivery and quality of care are unevenly available and not widely used.7–12 Additionally, several studies of typical EHR use have found an association with poorer quality of care or no differences when compared with care provided in practices using paper records.13–15 Critics of these studies have noted that cross-sectional or short observational studies are limited and that longer-term users are likely to have learned to more effectively, and successfully, use the technology. To date, there have been no reported comparisons of longer-term observation of quality of care in practices using EHRs with those using paper records. To address this gap, we examined data collected over 3 years as part of a quality improvement intervention in which some practices had implemented EHRs before initial data collection and continued to use that system throughout the observation period, whereas others used paper records throughout. As these practices were not offered assistance with improving their use of either record system, the study allows us to compare the outcomes of chronic illness care associated with typical use of both EHRs and paper records.
METHODS
To examine the relationship between EHR use and the quality of chronic illness care in primary care settings, we analyzed diabetes quality of care data collected at baseline and at 1- and 2-year follow-up from primary care practices participating in Using Learning Teams for Reflective Adaptation (ULTRA). The ULTRA study was designed to test the effect of a quality improvement process on adherence to multiple chronic disease guidelines issued by the US Preventive Services Task Force and the American Diabetes Association, including those for diabetes care, and followed primary care practices in New Jersey and Pennsylvania for 2 years, collecting data at baseline and at 1- and 2-year follow-up assessments.16,17 The quality improvement intervention focused on helping practices develop processes for reflection and adaptation to change.17
Inclusion Criteria
To be eligible for the current analysis, practices had to have complete medical record review data and have exclusively used either a paper or EHR system throughout a 1-year period before the study. Practices were excluded if they adopted a new EHR at any point during the study; thus, all EHR-using practices had been using their system for at least 1 year before the start of the study. By the study’s 2-year follow-up, 1 practice had closed and 11 practices had withdrawn from the study (most withdrew immediately after consenting because of an incomplete understanding of the study’s data collection requirements), and an additional 9 practices originally using paper records had adopted an EHR (Figure 1). Of the 42 remaining practices, 16 used EHRs and 26 did not.
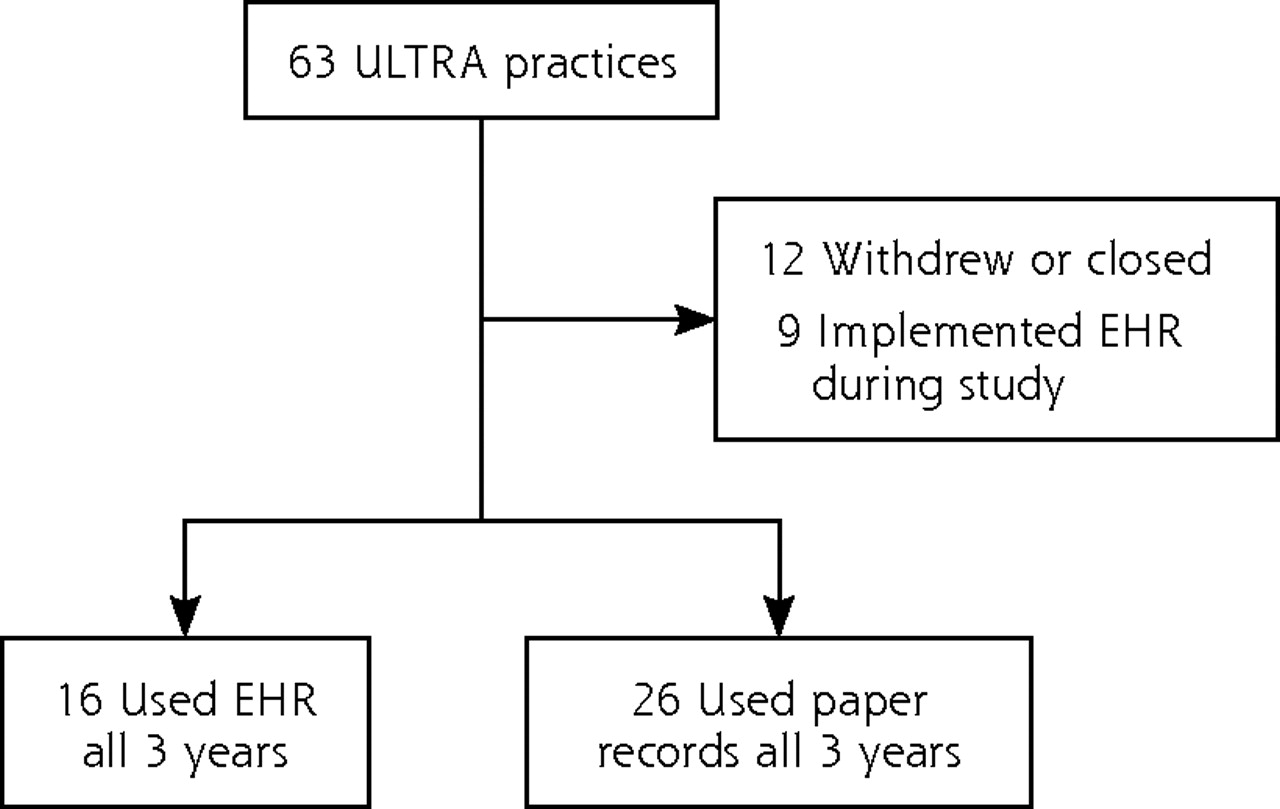
Primary care practice selection.
EHR = electronic health record; ULTRA = Using Learning Teams for Reflective Adaptation.
Data Collection
Data for this study were collected through practice observation, surveys of practice members, and medical record reviews. Our data collection methods have previously been described.17 Briefly, physician-owners or office managers at participating practices reported various organizational characteristics including practice type, ownership structure, number of clinicians and other staff, number of years in business, estimates of insurance payer mix, and whether they used an EHR. In addition, field researchers collected observational data documenting the type of medical records systems used in participating practices. Baseline assessment of patient records, including all available paper or electronic records, was completed in 2004. We then conducted follow-up assessments of patient records in 2005 and again in 2006. Each assessment of patient records focused on the previous 12 months and documented common measures of the quality of care. For the study reported here, we focused on the diabetes-related measures. At each assessment point, auditors retrospectively examined the charts of approximately 20 patients randomly selected from a list of all patients with an International Classification of Diseases, Ninth Revision (ICD-9) diagnosis code indicating that they had been treated for diabetes within the previous year (250.x). In practices with low numbers of patients with diabetes diagnosis codes, we audited the records of all eligible patients, an approach that led to variation in patient sample sizes for each assessment period.
Measurement
To assess diabetes quality of care, we measured adherence to guidelines in 3 areas—processes of care, treatment, and achievement of intermediate outcomes—and we created dichotomous composite scores for adherence in each of these areas (Table 1). Development of these measures has been previously described.14 For the process of care score, patients were assigned a value of 1 if any 3 or more of the 5 evaluation criteria were met and a value of 0 if not. For the treatment score, patients were assigned a value of 1 only if all criteria were met. For the outcomes scores, we constructed 2 scores from intermediate outcome measures: 1 for partial achievement (2 of 3 outcome targets achieved) and 1 for full achievement (all 3 targets achieved). We examined the 2 outcomes scores in separate analyses. To determine practice-level quality of care, we calculated the mean number of patients meeting each dichotomous measure.
Components of Guideline Adherence Scores
Statistical Analysis
To explore differences between the 2 groups of practices, we used the Fisher exact test for categorical variables (eg, ownership, practice type) and analysis of variance for continuous variables (eg, number of clinicians). When comparing patient-level variables, including adherence to guidelines, we used hierarchical linear models to account for clustering of patients within practices. In these models, we used a logit link for binary variables (eg, adherence to guidelines) and a standard identity link for continuous variables (eg, age). Pseudo-likelihood (using SAS PROC GLIMMIX, SAS Institute, Inc) was used for estimation. We examined within-year differences between the practice groups (EHR vs non-EHR) by stratifying analyses by year of observation. Changes in rates of adherence over time were evaluated by combining all data within a single analysis with a categorical variable for year. These models accounted for correlations between patients within a practice as well as within a particular year for each practice.
We then tested the interaction between practice group and time to examine whether the 2 groups improved their adherence to guidelines at different rates. This hierarchical modeling was also conducted adjusting for patient-level covariates (age and sex) and practice-level covariates (solo practice, physician owned, and staff–clinician ratio). Covariates were chosen to coincide with previously published analyses of baseline data.14 In addition, because these data were initially collected to examine the effectiveness of a quality improvement intervention that was implemented in approximately one-half of the participating practices immediately after baseline data collection, we also controlled for the effects of the intervention. Controlling for potential effects of the intervention did not significantly modify the results shown here. As adjustment for intervention arm or other covariates did not affect the results, we present unadjusted models for simplicity. All analyses were conducted using SAS 9.1 TS Level 1M3 XP_PRO platform (SAS Institute Inc, copyright 2002–2003).
This study was reviewed and approved by the institutional review board at the UMDNJ-Robert Wood Johnson Medical School.
RESULTS
The 42 participating practices included both solo and group practices, and slightly more than three-quarters (76%) of the practices were physician owned (Table 2). EHR use in this sample was somewhat higher than national averages for primary care, with 38% of practices reporting that they used an EHR throughout the observation period, compared with 13% nationally reporting use of at least a basic EHR system.12 Patients in practices that used EHRs were somewhat younger than patients in practices using paper records at baseline and the 1-year follow-up, but not at the 2-year follow-up. Practices did not differ significantly on any other patient-level or practice-level characteristics.
Patient and Practice Characteristics
The percentages of patients meeting guidelines for diabetes treatment and target achievement improved somewhat throughout the study, although even at the 2-year follow-up assessment, more than 40% of eligible patients were receiving care that did not meet process of care, treatment, or outcomes guidelines (Table 3). More than one-half of patients received recommended processes of care at each data collection point, and the modest improvements we observed were not statistically significant and did not differ significantly between groups of practices. Although adherence to treatment guidelines did improve significantly, from 43.8% of patients at baseline to 51.7% at the 2-year follow-up, the rates of improvement did not differ between the 2 groups of practices. The percentages of patients meeting recommended outcome targets also increased significantly between baseline and the 2-year follow-up, but again, rates of improvement did not significantly differ between the practice groups. Only 19.4% of patients across both groups met all 3 targets at that time point.
Percentages of Patients Whose Care Met Quality Standards During the 3-Year Observation Period
In cross-sectional analyses of the 2-year follow-up data using hierarchical logistic regression analyses, controlling for potential patient-level and practice-level confounders and for clustering of patients within practices, we found patterns similar to those observed at baseline (Table 4). Specifically, although patients in practices using paper records were consistently more likely to receive recommended care at the 2-year follow-up assessment, these differences were statistically significant only with regard to achievement of outcome targets. For example, the adjusted odds of a patient in a practice using paper records meeting all 3 outcome targets at the 2-year follow-up assessment were 1.67 times greater than those of a patient in an EHR-using practice.
EHR Use and the Quality of Diabetes Care at the 2-Year Follow-up
DISCUSSION
In this longitudinal observational study of primary care practices, we found that practices using an EHR for a 3-year period had a poorer quality of diabetes care at baseline, did not make more rapid quality improvements than practices using paper records, and had a poorer quality of diabetes care at the 2-year follow-up. Despite the evidence of steady improvement in diabetes quality throughout the study in both groups of practices, substantial room for improvement remained at the 2-year follow-up assessment, with fewer than 1 in 5 patients meeting recommended outcome targets. Our findings show that having an EHR as opposed to a paper-based record-keeping system does not guarantee better care and suggest that many practices that have adopted EHRs have not made the necessary changes to both work processes and ways of thinking about care that would lead to improvements in chronic illness management. Coupled with the findings from recent studies indicating that use of EHR-based clinical decision support (CDS) can lead to modest improvements in care,10,18 our findings suggest that, even among established users of EHR technology, effective use of CDS and population health management functions is likely not widespread.
Current incentive programs designed to encourage adoption of EHR technology by smaller primary care practices such as those represented here rely partly on new RECs to ensure that this adoption proceeds rapidly, effectively, and meaningfully.5,19 Because our findings suggest that many EHR-using practices are not providing better care for their patients with diabetes than paper-records practices, RECs should also focus on making more effective use of EHR technology to proactively address population health in practices that have already adopted these systems, while integrating CDS more effectively into clinical encounters.20 Although this assistance will need to focus on work process changes to support new population management activities (eg, assigning a member of the health care team to maintain disease registries), population management functions in most commercially available EHRs remain poor, and efforts to improve chronic illness care in primary care will be limited by the speed with which HIT vendors improve this key functionality.2 Policy makers should hold HIT vendors accountable for developing these capacities in ways that are usable in typical primary care practice settings while continuing to emphasize the importance of implementation of these functions as a key aspect of the meaningful use of EHRs. Currently, these functions are part of the “menu set” (optional features) of meaningful use criteria.5 Ensuring that use of these functions becomes a core element of meaningful use in the future will be essential for ensuring that EHR use translates into higher-quality care. In EHR-using practices, leaders should focus on engaging all members of the health care team in redesigning work to support efforts to improve population care—whether or not their current system supports these efforts.
In addition to the REC program, other national HIT initiatives may also lend important support to independent, unaffiliated practices as they work to ensure successful use of EHR technology to improve chronic illness care. For example, the Beacon Community Cooperative Agreement Program funded by the Office of the National Coordinator for Health Information Technology (ONC) funds 17 communities to develop health information exchange that, if successful, will greatly improve how independent practices share information about their patients with organizations with whom they work to provide health care (eg, hospitals, laboratories, diagnostic organizations, specialists). Additional ONC training and curriculum grants are focused on developing programs to train health care professionals to optimize the use of HIT in the patient care process. These efforts, along with those of the RECs, will be essential to ensuring effective use of this technology and will likely need to be expanded to ensure the realization of anticipated quality, safety, and efficiency gains from HIT use. Although key improvements to EHR technology are needed, these efforts, and the practice-based efforts to redesign the work process they will support, must focus on developing the human side of HIT implementation and use to ensure that quality gains are achieved in practice and to avoid disrupting care that is already less than optimal.
Our findings are limited in that practices in our sample were not selected to be nationally representative. In addition, the included practices are among the early adopters of EHR technology and may thus differ from those currently targeted for implementation support. It is not likely, however, that these community practices are unique in their struggles to optimize the use of an EHR. One way that EHR use is expected to improve primary care quality is through its potential use for identifying specific groups of patients, especially those with chronic illnesses such as diabetes, who may need preventive services but do not visit the office.20 We did not observe EHR use in these practices, so we do not know if the lack of improvement associated with this technology derives from the design of the particular EHR used or failure to use available features to identify gaps in care and address population health. Future studies of typical EHR use in primary care should focus on this issue.
Another study limitation is that we do not have information on how long the practices with EHRs have had them, and this group may therefore be somewhat heterogeneous; however, practices in the EHR group did not change record systems throughout the observation period and thus used a single system for at least 3 years. Because we relied on billing records to identify patient records for quality assessment, differences in the application of these codes could lead to differences in the patient samples assessed. It is unlikely that these differences are systematically related to use of an EHR, however, and our results were unchanged when controlling for differences in patient-level characteristics when comparing EHR-using and non–EHR-using practices. Finally, EHRs currently used by primary care practices may differ from those examined in this study; however, current users continue to report limitations in commercially available EHRs that lead to medication errors and work disruptions that could explain the differences in quality of care documented here.21
In conclusion, our findings show that even after the potentially disruptive phase of initial EHR implementation, quality improvements remain elusive. Achieving truly meaningful use of this technology will require more than time and experience: it will require a recognition that until population health is improved, use does not equal success.6 Practices will need assistance with implementation and achieving successful use to improve care and population health outcomes, especially with regard to redesigning work processes to make the best use of these new technologies by all members of the primary care delivery team. New payment models, such as accountable care organizations based on the patient-centered medical home principles,22,23 will also be needed to support population health management tasks associated with these improvements but currently not compensated in the fee-for-service environment.1,24 Payment reform will need to be coupled with changes in the mental models that drive primary care delivery and in the work of all members of the care team to support a new emphasis on population health. The National Demonstration Project showed that even among highly motivated practices, HIT implementation to meet these objectives remains difficult.25,26 Our findings suggest that those who are already using EHR technology in primary care will need support in redesigning their work processes and improvements in existing technology to achieve the truly meaningful and successful use of EHRs needed to improve individual patient care and population health outcomes.
Acknowledgments
We acknowledge support from the New Jersey Primary Care Research Network and the Eastern Pennsylvania Inquiry Collaborative Network.
Footnotes
-
Conflicts of interest: authors report none.
-
Funding support: Data collection for this study was supported by a research grant from the National Heart, Lung, and Blood Institute (R01-HL 70800-01, B.F. Crabtree, Principal Investigator).
- Received for publication April 11, 2011.
- Revision received September 13, 2011.
- Accepted for publication October 11, 2011.
- © 2012 Annals of Family Medicine, Inc.
References




{kind=link}
Jump to section
Related Articles
Cited By...
- Designing health information technology tools for behavioural health clinicians integrated within US-based primary care teams
- Implementation of data management and effect on chronic disease coding in a primary care organisation: A parallel cohort observational study
- Retroaction de la Sentinelle: une voie vers une utilisation significative des DME
- Sentinel feedback: path to meaningful use of EMRs
- In This Issue: From Communities of Solution to Joy