
Article Figures & Data
Figures
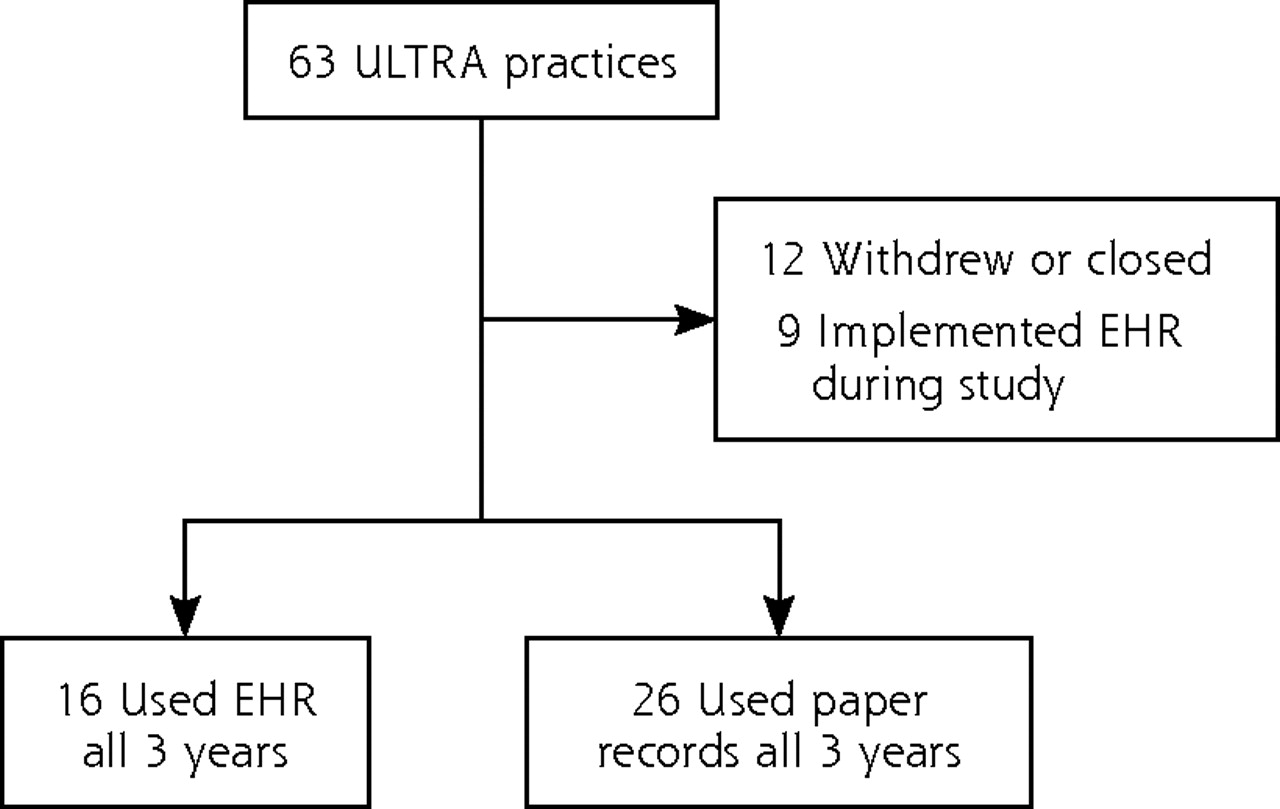
- Figure 1
Primary care practice selection.
EHR = electronic health record; ULTRA = Using Learning Teams for Reflective Adaptation.
Tables
Processes of Care Scorea Treatment Scoreb Outcomes Scorec HbA1c assessed within last 6 months HbA1c ≤8%, or >8% and on hypoglycemic agent HbA1c <7% Urine microalbumin assessed within last 12 months – – Smoking status assessed within last 6 months – – LDL-C assessed within last 12 months LDL-C ≤100 mg/dL, or >100 mg/dL and on lipid-lowering agent LDL-C ≤100 mg/dL BP recorded at each of 3 previous visits BP ≤130/85 mm Hg (systolic and diastolic), or >130/85 mm Hg (systolic or diastolic) and on antihypertensive BP ≤130/85 mm Hg (systolic and diastolic) Group Comparison Characteristic All Practices (n=42) EHR Practices (n=16) Non-EHR Practices (n=26) P Value Patients Baseline, No. 763 312 451 – Age, mean (SD), y 60.2 (14.6) 57.7 (14.9) 61.9 (14.1) .005a Women, % 53.0 55.4 51.3 .37a 1-Year follow-up, No. 792 298 494 – Age, mean (SD), y 60.1 (14.0) 57.0 (13.1) 62.0 (14.2) <.001a Women, % 48.3 53.9 44.9 .06a 2-Year follow-up, No. 798 306 492 – Age, mean (SD), y 60.5 (14.5) 59.2 (14.0) 61.3 (14.8) .23a Women, % 51.6 52.9 50.8 .69a Practices Number of clinicians, mean (SD) 5.0 (4.2) 5.8 (5.8) 4.4 (2.9) .48b Number of staff, mean (SD) 14.3 (10.4) 12.9 (8.8) 15.2 (11.4) .31b Staff–clinician ratio (SD) 3.1 (1.8) 2.7 (1.6) 3.4 (1.8) .26b Practice type, % (No.) .19c Solo 21 (9) 6 (1) 31 (8) Group 79 (33) 94 (15) 69 (18) Physician owned, % (No.) 76 (32) 63 (10) 85 (22) .14c Intervention, % (No.) 47 (20) 50 (8) 46 (12) 1.00c - Table 3
Percentages of Patients Whose Care Met Quality Standards During the 3-Year Observation Period
EHR Practices (n=16) Non-EHR Practices (n=26) EHR vs Non-EHR Practices All Practices (N=42) Quality Measure and Time Point % of Patients, Mean (SD) F2,45 (P Value) % of Patients, Mean (SD) F2,75 (P Value) F1,2222 (P Value) % of Patients, Mean (SD) F2,123 (P Value) Processes of care (3 of 5 criteria met) Baseline 45.1 (16.8) 0.44 (.65) 55.5 (24.9) 0.40 (.67) 0.02 (.98) 51.5 (22.5) 0.86 (.43) 1-Year follow-up 45.0 (27.7) 57.2 (22.3) 52.5 (24.9) 2-Year follow-up 51.1 (19.8) 60.7 (20.9) 57.0 (20.8) Treatment (all criteria met) Baseline 38.2 (14.3) 2.81 (.07) 47.2 (24.9) 1.28 (.28) 0.59 (.55) 43.8 (16.5) 3.26 (.04) 1-Year follow-up 42.2 (18.4) 47.3 (20.1) 45.4 (19.4) 2-Year follow-up 48.6 (13.5) 53.5 (19.8) 51.7 (17.6) Outcomes (2 of 3 targets met) Baseline 44.8 (15.3) 0.71 (.50) 52.5 (15.0) 4.32 (.02) 0.30 (.74) 49.6 (15.4) 4.68 (.01) 1-Year follow-up 44.8 (15.3) 52.8 (16.3) 49.8 (16.2) 2-Year follow-up 49.9 (16.0) 61.9 (15.2) 57.4 (16.4) Outcomes (all targets met) Baseline 10.3 (6.4) 2.21 (.12) 15.1 (9.7) 3.53 (.03) 0.08 (.93) 13.3 (8.8) 9.49 (.003) 1-Year follow-up 11.1 (7.8) 15.3 (11.2) 13.7 (10.1) 2-Year follow-up 15.9 (9.4) 21.5 (12.7) 19.4 (11.8) -
EHR=electronic health record.
-
Notes: F statistics and P values were calculated using hierarchical models with pseudo-likelihood estimation to determine whether changes in rates were significant for either EHR or non-EHR practices over time or whether rates of changes differed between the 2 groups over time. Results are unadjusted for covariates.
-
Quality Measure Adjusted Odds Ratio (95% CI) P Value Processes of care 1.60 (0.93–2.74) .09 Treatment 1.42 (0.81–2.49) .22 Outcomes (2 of 3 targets met) 1.54 (1.06–2.25) .02 Outcomes (all targets met) 1.67 (1.12–2.51) .01 -
EHR=electronic health record.
-
Comparison is for non-EHR practices vs EHR practices.
-
The Article in Brief
Jesse C. Crosson , and colleagues
Background It is widely expected that use of electronic health records (EHRs) will lead to improvements in health care safety, quality, and efficiency. This study analyzes diabetes care outcomes in practices that use an EHR compared with those using paper records.
What This Study Found Over a 3-year period, practices using an EHR did not make more rapid quality improvements than practices using paper records and, after 2 years, had poorer diabetes care quality.
Implications
- Having an EHR as opposed to a paper-based record keeping system does not guarantee better care.
- Adopting an EHR requires corresponding changes in work processes and ways of thinking about care that lead to improvements in chronic illness management.




{kind=link}
Jump to section
Related Articles
Cited By...
- Designing health information technology tools for behavioural health clinicians integrated within US-based primary care teams
- Implementation of data management and effect on chronic disease coding in a primary care organisation: A parallel cohort observational study
- Retroaction de la Sentinelle: une voie vers une utilisation significative des DME
- Sentinel feedback: path to meaningful use of EMRs
- In This Issue: From Communities of Solution to Joy