
Abstract
PURPOSE Disparities in the use of shared decision making (SDM) affect minoritized patients. We sought to identify the barriers and facilitators to SDM among diverse patients.
METHODS We conducted a scoping review in adherence to the Joanna Briggs Institute’s methodologic framework. Our search of 4 databases—PubMed, Scopus, CINAHL Plus with Full Text, and PsycINFO—used controlled vocabulary and key word terms related to SDM in the care of racially and/or ethnically diverse adults in the primary care setting. We included peer-reviewed studies conducted in the United States or Canada that evaluated the process of decision making and that had populations in which more than 50% of patients were from racial and/or ethnic minorities. Unique records were uploaded to a screening platform for independent review by 2 team members. We used grounded theory to guide our inductive approach and completed a thematic analysis.
RESULTS A total of 39 studies met all inclusion criteria. We identified 5 overarching themes: (1) factors regarding the decision-making process during the clinical encounter, (2) clinician practice characteristics, (3) trust in the clinician/health care system, (4) cultural congruence between clinician and patient, and (5) extrinsic factors affecting the decision-making process. Barriers of SDM included cultural and language discordance; prejudice, bias, and stereotypes; mistrust; and clinician time constraints. Facilitators of SDM included cultural concordance between clinician and patient; clinician language competence; and clear, honest, and humanistic communication with patients having the ability to ask questions.
CONCLUSIONS We identified a set of potentially modifiable factors that facilitate or impede SDM. Our findings can help inform strategies and interventions to improve SDM among racially and/or ethnically diverse patient populations.
- decision making, shared
- patient-centered care
- primary health care
- healthcare disparities
- scoping review
- communication
- medical decision making
- physician-patient relations
- communication
- race
- ethnicity
- minority groups
- vulnerable populations
- practice-based research
INTRODUCTION
Shared decision making (SDM) is a dynamic process whereby patients and clinicians collaborate to exchange information, explore treatment options, and consider patient values and preferences to arrive at medical decisions that are not only clinically effective but also acceptable to patients, fostering personalized health care strategies.1-3 Although SDM holds great potential for centering clinical decision making around patient values, especially in underserved populations, existing literature exposes concerning disparities in the prevalence and quality of its use, particularly in the context of minoritized patients.4-6 Ethnic minority populations consistently report receiving insufficient information about their health conditions and a lack of respect for their treatment preferences.1,7-9 African American patients have reported fewer participatory health care visits compared with their White counterparts.4 The consequences of these disparities in the implementation of SDM principles are profound: patients who perceive a lack of respect or involvement in the decision-making process are prone to lose trust in their clinicians and therefore experience increased risk for poorer health outcomes.5,8,10
We used a scoping review methodology to examine the body of literature assessing how minoritized patients experience SDM within primary care visits.11 Our review examined literature evaluating the process of SDM in the primary care setting, specifically focusing on the dynamics between racially and/or ethnically diverse patients and their clinicians. Our objectives were to examine how clinical decisions are made and what factors affect the decision-making process, all within a primary care encounter. We included studies focusing on varied medical conditions and looked in depth at how patients and clinicians made decisions and communicated about making those decisions. The majority of the studies had a qualitative design,5,12-43 yielding rich insight into cognitive and behavioral influences.
Our aim was to shed light on the barriers and facilitators that shape the quality and extent of SDM experiences among diverse patients in order to improve care within outpatient primary care visits. Understanding the factors affecting the SDM process in this context is crucial to developing targeted interventions to improve the overall quality of health care delivery in a more inclusive manner. Insights gained from this study can inform strategies to enhance SDM and reduce racial and ethnic health care disparities in patient-clinician relationships and communication.
METHODS
We undertook a scoping review following the Joanna Briggs Institute’s methodologic framework44 and, herein, we report on the review in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for Scoping Reviews checklist (PRISMA-ScR).45 This framework provides a systematic approach to mapping evidence on a particular topic, including identifying research gaps, synthesizing evidence, and ensuring comprehensive reporting through the PRISMA-ScR guidelines.
Search Strategy
Our team’s research librarian (L.C.) developed and executed a comprehensive search of the literature, combining controlled vocabulary and key word terms related to SDM in the care of racially, ethnically, and/or culturally diverse patients in the primary care setting. We searched 4 databases from their inception to present on May 8, 2023: PubMed, Scopus (Elsevier), CINAHL Plus with Full Text (EBSCO), and PsycINFO (EBSCO). (Full search strategies in Supplemental Appendix.) No language, publication type, or other filters were used, and no restrictions on publication dates were applied. Results were downloaded to EndNote citation management software (Clarivate) and underwent manual de-duplication by the research librarian. Unique records were uploaded to a screening platform (Covidence) for review by team members. Records were also identified by searching the references of studies identified for inclusion in the review. No study registries or other online resources were searched, and no additional studies or data were sought by contacting authors. Given that one of our inclusion criteria (described below) required that studies be peer-reviewed studies, we did not search or include gray literature sources (such as conference abstracts, conference proceedings, dissertations, and research reports).
Study Selection
Our inclusion and exclusion criteria were iteratively enhanced during the process of reviewing studies to increase specificity to the target topic of SDM with a focus on the process of decision making (Supplemental Table 1). We included peer-reviewed studies with original data on SDM specific to a medical decision among adults, but excluded those limited to decision aid testing and decision interventions.
We also excluded studies from countries other than the United States and Canada because of potential differences in approaches to clinician-patient communication and decision making. To focus on the process of SDM in a primary care setting, we excluded studies that took place in specialty clinics or hospitals. To focus on racial and ethnic diversity, we excluded studies whose populations were diverse solely on gender. Moreover, in keeping with this goal, we included only studies that had populations in which more than 50% of participants were from racial and/or ethnic minorities.
Two of the 3 authors (D.D., S.S., Y.A.) screened each title and abstract for eligibility. The same authors then reviewed each full-text article for relevance to the topic of the decision-making process using the inclusion and exclusion criteria. We resolved conflicts through direct discussion among the 3 clinical members of the study team (D.D., S.S., Y.A.).
Data Extraction
Two of the 3 authors (D.D., S.S., Y.A.) conducted data extraction for each included study using a custom data collection form created in Covidence by the study team. We collected study characteristics (country, study aim, topic of medical decision, study design, number and race and ethnicity of participants) and text from study results and discussion that captured study findings. Data were imported into an Excel spreadsheet (Microsoft Corp), where we summarized the study designs, populations, decision topic, and broad findings.
Data Synthesis and Analysis
This scoping review used a grounded theory framework to derive ideas from the data and thematic analysis as a method to identify themes within studies looking at the process of decision making in primary care encounters.46,47 Grounded theory was used as an inductive approach to exploring themes within the studies included and generating a theoretical framework grounded in the data rather than testing an existing theory.
We coded the results of each study, searched for themes, and then reviewed the themes, looking for internal homogeneity of the data and external heterogeneity of the themes. Two researchers (S.S., Y.A.) agreed on the theme designations. The data were organized by themes and subthemes and also by barriers and facilitators for SDM. Further analysis grouped themes based on their temporal relationship to the visit (before, during, or after).
RESULTS
Study Selection and Characteristics
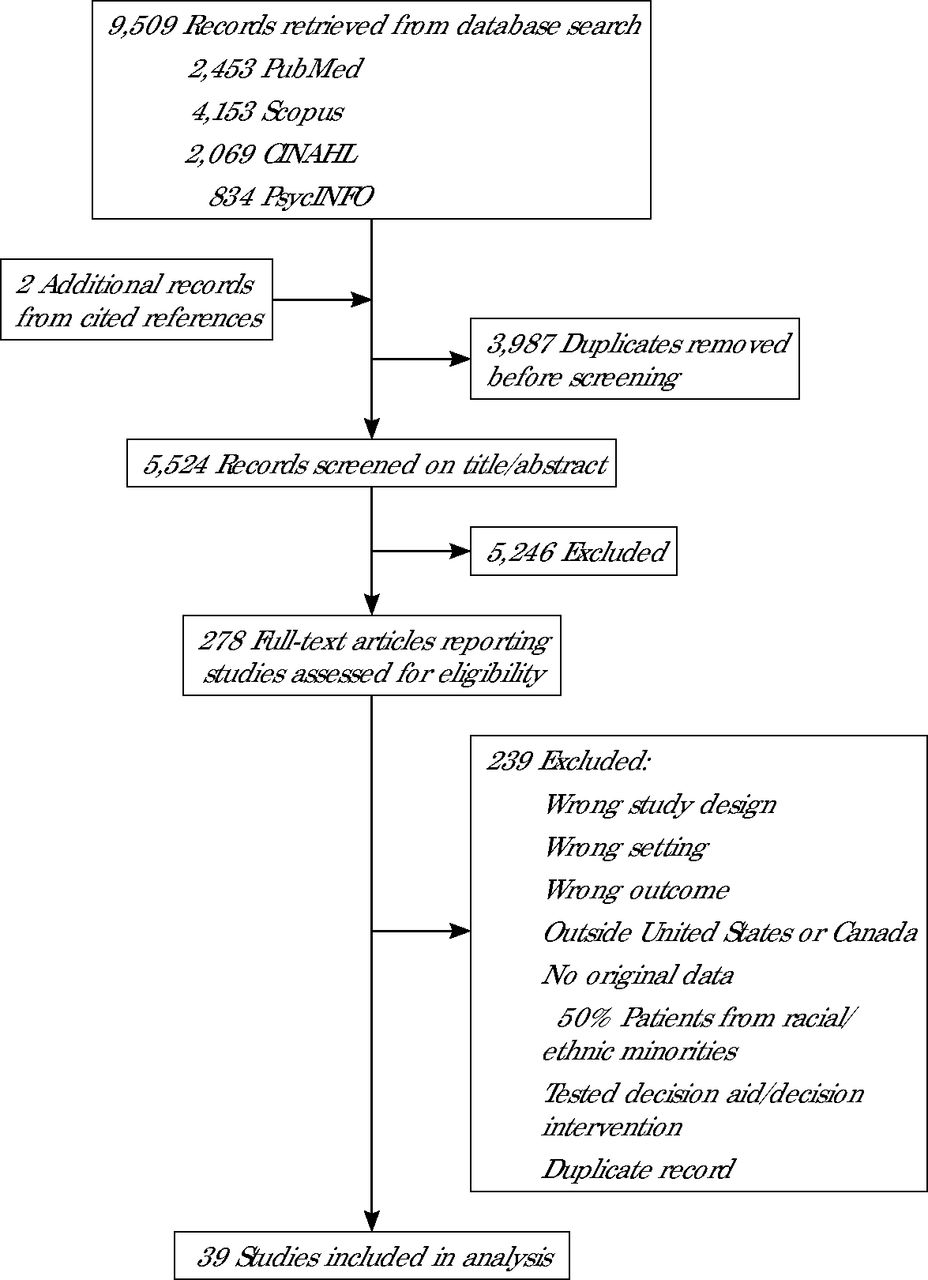
Our literature search retrieved 9,509 records (Figure 1). After removing duplicates, we screened the titles and abstracts of 5,522 records for eligibility. Two additional records were identified through searching the references of studies identified for inclusion in the review and underwent screening. We thus screened 5,524 records.

PRISMA Flow Diagram
PRISMA = Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
Ultimately, 39 studies met all of the inclusion criteria.5,12-43,48-53 Their characteristics are summarized in Table 1 and detailed in Supplemental Table 2. Thirty-eight of the studies were conducted in the United States; 1 was conducted in Canada.28 Most had a qualitative study design.5,12-43 Fully 35 studies focused on decision making among African American/Black and Latino/x/e patients.5,12,13,15-27,29-43,48-50,53 Ten pertained to decision making on the management of chronic illnesses,20,26,32,34-37,39,40,49 8 to decision making about cancer screening,12-14,21-24,33,41,43,53 6 to contraceptive decision making,15,16,18,19,30,48 and 3 to mental health treatment.17,23,38
Summary Characteristics of the 39 Studies
Main Themes
We identified 5 overarching themes of SDM in diverse populations during our review: factors regarding the decision-making process during the clinical encounter, clinician practice characteristics, trust in the clinician and health care system, cultural congruence, and extrinsic factors affecting the decision-making process. These themes and related subthemes are detailed in Table 2 and discussed further below.
Overarching Themes and Subthemes, and Examples From Studies
Factors Regarding the Decision-Making Process Encounter
Many of the studies described factors that affected the use of SDM during a clinical encounter (Table 2). Patients discussed their ability to participate in the decision-making process with the clinician.18,30,31,38,40,41,49,50,52-54 Specific factors that affected ability to participate included the way in which the clinician shared information,16,25,30,31,34,35,37,49,50 whether the clinician made a recommendation,18 and how the clinician encouraged the patient to share information.32,34,37 Patients also prioritized the ability to ask questions that enhanced their self-efficacy within the clinical visit.30,31,35
Clinician Practice Characteristics
Several studies discussed the role that various aspects of clinician-patient communication play in SDM (Table 2).5,20,30,34,35,37,50-52 The importance of humanistic communication was frequently described, as was clear and honest communication.5,20,51,52 In one study, effective communication, described as a relationship in which the clinician seeks to know and understand the patient and family, was foundational to tailored communication and decision making.53 Clinician time constraints were a barrier to SDM.17,18,20,51,52 Studies additionally highlighted how clinicians disliked being questioned, how they became impatient or dismissive when the patient attempted to ask questions, and how patients reported making accommodations for the clinician, prioritizing harmony with the clinician over their own care.17,28,36,52
Trust in the Clinician and Health Care System
Trust and factors impacting trust were often mentioned in the studies reviewed (Table 2). Facilitators of patient trust in SDM included clinician interpersonal skills; honesty and information sharing; promoting of patient sharing; medical skills and technical competence; and a balance of power.35,37,50,51 Barriers to patient trust included physician racial bias, cultural discordance between the clinician and patient, experiencing prejudice from the clinician, past experiences of health care discrimination, and invalidation of illness experiences and concerns.31,37,38,50 Mistrust (of the medical profession generally and of clinicians specifically) was an additional factor that affected SDM, as was suspicion of the effect of recommended medications on health, of clinician motives and intent, and of clinicians overall.20,32,50,51
Cultural Congruence
Studies described how not sharing racial, ethnic, cultural, and/or social background with one’s clinician was a barrier to developing patient-clinician SDM relationships, whereas having a clinician with similar lived experiences or sharing the same racial and/or ethnic identity promoted relationship building (Table 2).17,31,36,37 In addition, patients valued having culturally sensitive clinicians and interactions.39 Language barriers between patients and clinicians were identified as a barrier to engaging meaningfully in SDM.39,51,52 Patients noted the need for improved language competence by their clinicians and lamented the lack of high-quality interpreter services.39 Language barriers impeded in-depth treatment discussions, and patients indicated that translators did not always fully or accurately translate.28,39,52
Extrinsic Factors Affecting the Decision-Making Process
Factors outside of the encounter and clinician-patient relationship, including family members’ or peers’ past experiences with similar conditions or treatments, also affected SDM (Table 2). Several studies described the importance of family members in the decision-making process during or outside the visit.5,27,52 Some patients valued input of their family on health care–related decisions, and others added that incorporating family could facilitate adherence and engagement.5,27,52 Studies described how decisions about care occur subsequent to the encounter, whereby a patient responded to a clinician’s recommended treatment plan behaviorally, by adhering or not adhering to the recommendations.31,34 For patients, what could be viewed as nonadherence by clinicians was appropriate decision making about care occurring outside of the clinical encounter based on incorporating information gained through discussions with family and friends.34
Thematic Framework
In total, our analysis identified 8 barriers and 15 facilitators for SDM (Table 3). All have implications for clinical practice, and most can be modified with strategies and interventions at the clinician and/or health system level, seen in the table.
Barriers and Facilitators for Shared Decision Making and Their Practice Implications
The overall thematic framework for our findings is shown in Figure 2. This framework outlines the 3 phases of the decision-making process (previsit, visit, and postvisit) at which barriers and facilitators can impact the SDM process and relationship for better or worse.

Thematic Framework for Shared Decision Making
DISCUSSION
Summary of the Evidence
This scoping review on factors influencing SDM with racially and/or ethnically diverse populations in primary care settings analyzed 39 studies. We categorized themes as barriers or facilitators for SDM and organized them based on the phase at which they come into play. Before and during the visit, SDM is affected by the clinician-patient relationship, presence of trust in the dyad, and cultural concordance. Clinician characteristics that facilitate SDM include clear communication, availability, respect, and focus on joint information sharing and decision making. Factors that impact SDM after the visit include consultation with family members and friends throughout the decision-making process. Our study illustrates that although there is diversity in preferences across diverse individuals, using commonsense communication strategies will facilitate SDM, whereas experiences of prejudice, bias, clinician impatience, and insufficient time for questions and discussion will impede SDM.
Recommendations to Improve SDM With Diverse Populations
Clinician-Patient Communication
Patients desire clear, understandable, humanistic communication that conveys empathy, concern, and compassion from their clinician.5,34 They also desire the ability to “tell their story,” to be heard, and to be validated, however.34,50 Patients value information sharing, supported agency in decision making, and having the ability and the time to ask questions.25,34,49,50,52 Clinicians can prioritize patients’ desire to feel heard by asking them what is important to them about the specific decision being made during the visit.
Trust
Trust in the health care system and in one’s primary care clinician can substantially impact the relationship. Our review highlights that trust is a facilitator in SDM and that various factors can promote or inhibit trust and trusting relationships between clinicians and patients. For example, in one study on mental health, a trusting relationship was critical to being open to treatment discussions and willingness to try different treatment modalities, including those outside patients’ originally stated treatment preferences.38 Patients who had experienced health care discrimination, however, faced greater challenges to forming trusting relationships with clinicians to engage in SDM.38 To promote trust, clinicians can communicate honestly, give more information, encourage patient sharing and question asking, validate individual experiences, and promote a balance of power through consideration of patient preferences.20,34,35,37,50,52 Patient and engaging communication, whereby clinicians talk with patients rather than at patients, will promote trusting SDM relationships with diverse patient populations.5
Cultural Congruence
Cultural and language congruence between clinicians and patients was a theme that also arose frequently, whereby concordance was a facilitator and discordance was a barrier to SDM. Health care systems can focus on hiring and retaining a workforce that is diverse in race, ethnicity, and cultural identity as well as social background, so that patients can have access to clinicians with similar lived experiences with whom they can develop the trusting clinician-patient relationships essential for SDM. Ensuring a language-capable workforce is similarly needed in light of negative patient experiences with interpreters that impeded SDM in the studies reviewed.51,52 Clinicians who do not share cultural (and language) congruence with patients can still promote therapeutic relationships with patients by ensuring in-depth treatment discussions, providing time to ask questions, and avoiding invalidation, race- and ethnicity-based judgements, and discrimination.38,48,50,52
Inclusion of Family Members in the Decision-Making Process
Clinicians should elicit patients’ preferences regarding family member participation and ensure their inclusion if the patient requests their input. Respecting the importance of family involvement may enhance the trust that the patient has in the clinician and the health care system and may help improve adherence to agreed-on interventions. Clinicians and health systems can welcome family involvement in decision-making visits. Clinicians can also recognize that patients may talk to people outside of the visit about their decision and should ask patients who helps them with decision making.
Limitations
This study was limited by the inclusion and exclusion parameters that we chose. We excluded studies from countries outside of the United States and Canada, which may have limited the information collected. We also focused on the patient-clinician interaction within a primary care office visit, potentially missing out on informative data from studies conducted in specialty clinics or in hospitals. Our study is also limited by the original study populations, which were predominantly African American and Hispanic/Latino/x/e, and therefore by underrepresentation of other racial and ethnic groups.
Conclusions
Our analysis shows that focusing on clear, honest, and compassionate clinician communication that enables and encourages patient information sharing and question asking will facilitate SDM in racially and/or ethnically diverse populations. Health systems can promote SDM by ensuring a language-capable and culturally diverse clinician workforce that is accessible and enables visits in which patients have sufficient time and opportunity to ask questions and tell their illness story. Above all, when caring for patients, as individually based preferences are likely, avoiding assumptions and eliciting personal preferences is paramount.
Acknowledgments
We are grateful to the UW-Madison Department of Family Medicine Original Research Writing Group for their review and helpful reflections that helped strengthen the quality of our manuscript.
Footnotes
Conflicts of interest: authors report none.
Funding support: Funding for this study was provided by the UW-Madison Department of Family Medicine Summer Student Research and Clinical Assistantship program, which supported D.D.
Disclaimer: The views expressed are solely those of the authors and do not necessarily represent official views of the authors’ affiliated institutions or funders.
Previous presentations: Preliminary results from this project were presented in a poster at the NAPCRG annual meeting; Oct 30-Nov 3, 2023; San Francisco, California and Nov 2024; Quebec City, Canada.
- Received for publication February 19, 2024.
- Revision received October 19, 2024.
- Accepted for publication November 4, 2024.
- © 2025 Annals of Family Medicine, Inc.
References
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.