
Abstract
BACKGROUND We wanted to determine the frequency of self-reported receipt of screening mammography and Papanicolaou (Pap) tests in older women and investigate important predictors of utilization, based on 2 national longitudinal surveys.
METHODS This cohort study includes participants from 4 waves (1994–2000) of the Health and Retirement Study (HRS)—5,942 women aged 50 to 61 years, and 4 waves (1993–2000) of the Asset and Health Dynamics Among the Oldest Old (AHEAD) survey—4,543 women aged 70 years and older. The self-reported receipt of screening mammograms and Pap smears in the most recent 2 years were reported in 1996 and 2000 for HRS, with predictors of receipt measured in 1994 and 1998. In AHEAD, the self-reported receipt of screening mammograms and Pap smears in the most recent 2 years were reported in 1995 and 2000, with predictors of receipt measured in 1993 and 1998.
RESULTS Receipt of mammography is stable at 70% to 80% among women aged 50 to 64 years, then declines to around 40% among those aged 85 to 90 years. For Pap tests there is a decline from 75% among women aged 50 to 54 years to 25% in those aged 85 to 90 years. For both mammography and Pap tests, the rates increased in all groups from 1995/1996 to 2000. Higher education, being married, higher income, not smoking, and vigorous exercise were consistently associated with higher rates of receipt.
CONCLUSIONS Although the use of mammography and Pap tests for screening declines into old age, use has been increasing recently. The large and increasing number of tests performed might not be justified given the lack of evidence of effect in older age-groups.
- Aged
- cohort studies
- health services for the aged
- mammography
- Papanicolaou test
- preventive health services
INTRODUCTION
Health maintenance care for young adults is focused on identification and reduction of long-term health risks, whereas care for elderly patients is generally focused on case finding. Early discovery of treatable, asymptomatic cancers is an important motive for patients and clinicians, but an important question persists: Is it reasonable to screen for common cancers in the elderly?
The exponential age-related increase in incidence of some cancer types argues in favor of increased screening. Furthermore, case fatality rates also increase with age.1 There is also evidence that increasing age is associated with an increasing “sojourn time,” which begins when cancer might first be detected by screening and ends when cancer is detected through the appearance of symptoms. Given a certain screening interval, increased sojourn time allows a larger proportion of cancers to be detected in a preclinical stage.
Life expectancy obviously decreases with age, however, and the competing risk of dying from other diseases increases rapidly, reducing the number of years that can be saved through screening. There is also a selection problem: the healthiest elderly, with lower risk of disease, are more likely to be screened. For example, in a Dutch breast cancer-screening study,2 those who were screened lived 2 years longer than those who were not, even when the effects of screening on breast cancer mortality were statistically excluded. Thus, the apparent benefit of screening is falsely increased by patient self-selection.
Furthermore, there are no rigorous studies showing that screening of the very old provides clear benefits. Most studies have excluded the very old. In the Swedish Two County Trial of mammography,3 screening that began in the oldest age-group (ages 70 to 74 years) was abandoned because of poor attendance.
Clinical Guidelines
Reflecting these opposing considerations and the lack of evidence, it is not surprising that cancer-screening practice guidelines are ambiguous and inconsistent for elderly women.
Breast Cancer
For women aged 50 to 69 years, guidelines are consistent with regard to annual or biannual mammograms.4–,8 After the age of 70 years, most recommendations cite inconclusive evidence for the need for mammograms but support them so long as the woman is healthy enough to endure the treatment regimen for any detected cancer. The American Cancer Society differs slightly,6 providing no specific age for cessation and stating that comorbidity is the only qualifying factor for exclusion from screening. The Health Plan Employer Data and Information Set (HEDIS) parameters are report cards for clinical practice that affect clinical reimbursement and group practice certification; the HEDIS breast cancer-screening rate includes women aged 52 to 69 years.9 Finally, Healthy People 201010 has set as a target that 70% of all women aged 40 years or older should have received a mammogram within the preceding 2 years.
Cervical Cancer
Most recommendations relating to Papanicolaou (Pap) smears suggest that they should be done after a woman has sexual intercourse or by age 18 years if her sexual activity status is unknown.5–,8 Most recommend screening at a minimum of 3-year intervals even after a series of 3 Pap test results have been normal. The American Cancer Society6 suggests that women aged 70 years of age or older who have had 3 or more normal Pap test results in a row and no abnormal test results in the last 10 years may choose to stop having cervical cancer screening.
The HEDIS cervical cancer screening measure is based on women aged 21 to 64 years,9 but Healthy People 201010 has set as targets that by 2010, 97% of all women aged 18 years or older should have ever received a Pap test, and 90% of these women should have received it within the preceding 3 years.
Given the uncertain benefits, combined with the substantial economic and psychological costs associated with large-scale screening, it is of interest to document whether screening for common cancers among women persists into old age and to investigate factors associated with such screening practices.
The objective of these analyses was to document the provision and receipt of mammography and Pap tests with respect to age using 2 large national studies of middle-aged and older Americans. We investigated how self-reported utilization frequencies vary by age, and whether there have been any recent (from 1996 to 2000) changes in these frequencies. The importance of plausible (demographic, socioeconomic, health, and health care) predictors of utilization are investigated in multivariate analyses.
METHODS
Data
The Health and Retirement Study (HRS),11 a national panel study, contains information about health behaviors, disease and disability, and medical care usage. The baseline survey was conducted in 1992 for the 1931–1941 birth cohort of women (and their spouses, regardless of age) (n = 12,652). Questions relating to receipt of clinical preventive services, including certain cancer-screening tests, were included for all participants in wave 3 (1996) and wave 5 (2000). In our analyses, women who responded to these questions in at least 1 wave were included (n = 5,942).
The Asset and Health Dynamics Among the Oldest Old (AHEAD) is a companion study including an older age-group.12 The initial sample (wave 1 in 1993) included respondents aged 70 years and older (and their spouses, regardless of age) (n = 7,447). Persons older than 80 years were oversampled to allow for more precise estimates in this group. Follow-up interviews were conducted in 1995, 1998, and 2000. The questions pertaining to mammography screening and Pap tests were asked of all respondents in wave 2 (1995) and in wave 4 (2000), and women who answered these questions at least once are included in our analyses (n = 4,543). African Americans (blacks) were oversampled (100%) in both surveys.
Dependent Variables
The questions (both from the preventive procedures section of the questionnaires) were as follows: (for mammogram) “Did you have a mammogram or x-ray of the breast, to search for cancer in the last two years?” and (for Papanicolaou test) “In the last two years, have you had any of the following medical tests or procedures: a Pap smear?”
Explanatory Variables
Cancer screening was reported in 1996 and 2000, with the corresponding explanatory variables measured in 1994 and 1998, respectively, for HRS. In AHEAD, reports on cancer screening were collected in 1995 and 2000, with the corresponding explanatory variables measured in 1993 and 1998, respectively. Age was grouped in 5-year intervals. Other explanatory variables included racial group (black, white), education (at least some college education, completed high school or less), place of birth (United States, abroad), marital status (married, unmarried), smoking (current smokers, nonsmokers), exercise (vigorous, lower levels of physical activity) and self-reported health (fair or poor, excellent, very good or good). Subjective life expectation was coded as high, medium, and low (footnote, Table 1⇓). Household income was categorized into 4 groups (footnote, Table 1⇓). In HRS respondents who had no health insurance were compared with those who had any type of health insurance; in AHEAD, where nearly all participants were insured by Medicare, those who had additional, private insurance were compared with those who had none. Participants who had been hospitalized in the last year were compared with those who had not. Number of outpatient physician visits was categorized as 0 to 2, 3 to 5, 6 or more.
Receipt of Preventive Services by Survey Wave in Selected Subgroups (Weighted Percentages)
Analyses
The weighted proportions (taking into consideration oversampling of blacks and residents in certain states) of respondents who reported having received the screening test since the previous wave were calculated by year (wave: 1995 [AHEAD] and 1996 [HRS], and 2000) and age-group. For consistency with the multivariate analyses, the sampling weights were from the previous wave (see below).
The weighted relationships between the explanatory and screening variables were tabulated for respondents who completed the screening question in 1995/1996 or 2000, or both. Because the outcome question referred to receipt of the screening test in the interval between the current and the previous wave (“In the last two years ...” or “... since we spoke to you last.”), the values of the explanatory variables from the wave preceding the value of the outcome variable were selected (ie, explanatory variables 1994 → outcome 1995/1996; explanatory variables 1998 → outcome 2000.) Using multivariate logistic regression, models were first developed separately for outcomes reported in the 1995/1996 wave and for the outcomes reported in the 2000 wave (not shown). Subsequently, observations for each respondent were stacked (each respondent provided 2 outcome values and 2 sets of explanatory values). In the latter models, because the observations for the same person in different waves are not independent of each other, clustering of observations at the individual level was adjusted by using Huber-White corrected standard errors.13,14 Although similar explanatory variables were used, models were estimated separately for AHEAD and HRS. In addition to simple models including only wave and demographic variables (age and racial group) (not shown), more extensive models were also developed including explanatory variables from the socioeconomic, health, and health care domains.
STATA (version 6.0) was used for the statistical analyses.
This study proposal was approved by the Duke University Medical Center Institutional Review Board.
RESULTS
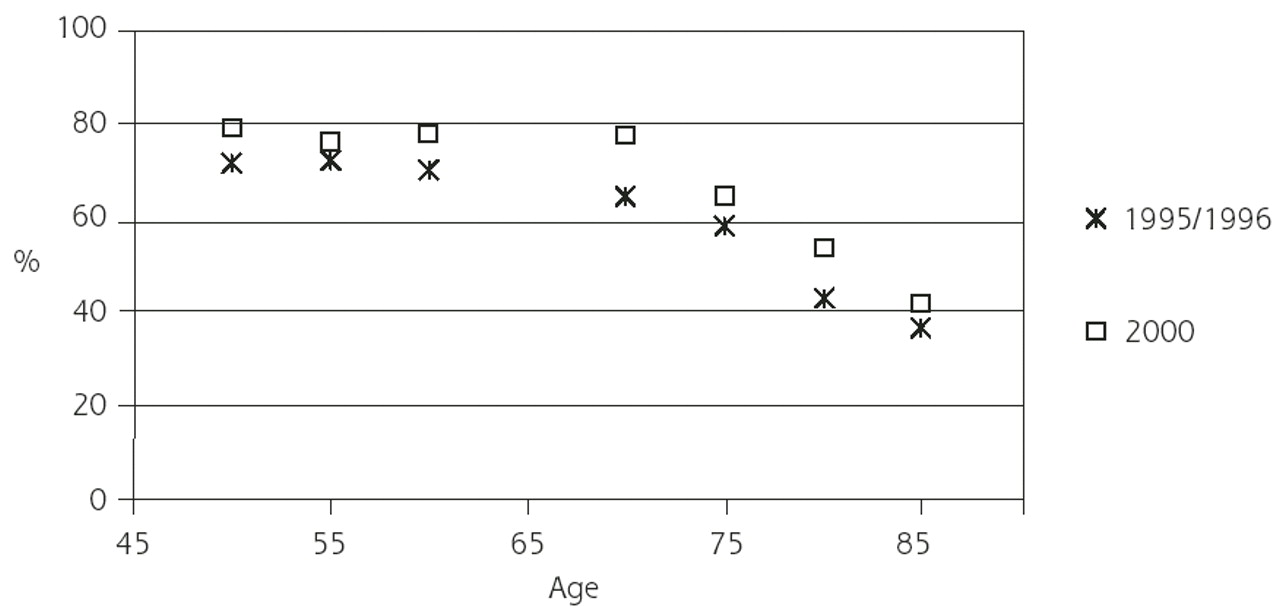
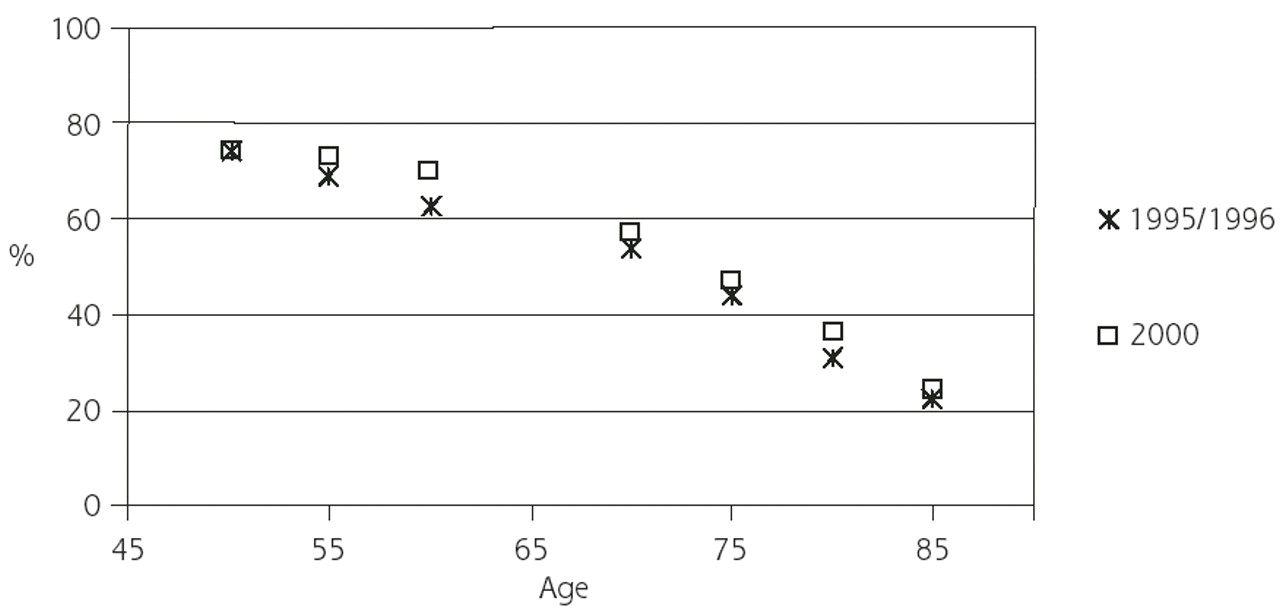
For both mammography and Pap tests, the rates increased among all age-groups from 1995/1996 to 2000. Receipt of mammography (Figure 1⇓) by age was relatively stable at 70% to 80% until approximately age 70 years, at which time it declined to about 40% among those aged 85 to 90 years. For Pap tests (Figure 2⇓), there was a decline by age from 75% at age 50 to 54 years to 25% at age 85 to 90 years.

Mammography: proportion (weighted) reported screening in the last 2 years, by age-group and year.

Cervical cancer: proportion (weighted) reported screening in the last 2 years, by age-group and year.
Table 1⇑ shows that, in bivariate analyses of HRS data, there were few differences by racial group or country of birth for receipt of either of the screening tests. Higher education levels, being married, and higher income were all positively related to receipt of both screening tests. Nonsmokers were more likely to have undergone screening, as were those who perceived their health as excellent, very good, or good. Those who thought there was a better chance that they would live beyond the age of 75 years were more likely to be screened than those who did not. Lacking supplemental health insurance was related to lower rates of screening. Hospitalization in the last year had little effect, whereas those with more outpatient visits in the last year were more likely to be screened.
In bivariate analyses of AHEAD (Table 1⇑) data, differences between blacks and whites were also small. Consistent with the findings from HRS, higher education, being married, higher income, not smoking, no cognitive impairment, perception of health to be excellent, very good, or good, and higher subjective life expectation were positively related to both screening behaviors. Elderly persons with additional health insurance were more likely to be screened than their counterparts without additional health insurance. Hospitalization in the last year did not affect outcomes, but those who had more physician visits were more likely to be screened.
The multivariate results (HRS, Table 2⇓; AHEAD, Table 3⇓) are broadly consistent with the bivariate results. In HRS, there were significant increases in mammography screening from 1995/1996 to 2000. Because of the large number of independent variables tested in the models, which therefore increased the probability of type I error, the significance of 95% confidence intervals around the odds ratios with upper or lower bounds close to 1 must be interpreted with caution.
Adjusted Relative Odds of Receipt of Cancer Screening Services: Health and Retirement Study (HRS) Multivariate Models
Adjusted Relative Odds of Receipt of Cancer Screening Services: Asset and Health Dynamics Among the Oldest Old (AHDEAD) Multivariate Models
For mammography screening, there was no decline by age in HRS, but a decline by age was observed in AHEAD. There was a decline in Pap tests by age-group in both surveys. Higher education, being married, higher income, not smoking and vigorous exercise were significantly associated with higher screening rates in all models. Black women were more likely to report having been screened in the last 2 years than white women. In HRS those with health insurance and in AHEAD those with additional health insurance were more likely to have received screening. More physician visits also remained significantly associated with screening in all models.
In HRS those with the highest subjective life expectation were more likely to have received either screening test. In AHEAD those with subjective life expectation in the middle range (34% to 66%) were more likely to have received a mammogram than those with lower or higher subjective survival expectations; screening rates for those most optimistic regarding their future survival did not differ significantly from the most pessimistic group.
DISCUSSION
Period Effects
In bivariate analyses screening rates increased from the 1995/1996 wave to the 2000 wave in all age-groups and for both screening tests. These increases might be attributable to better access to health services in general, increases in the perception of the utility of these interventions, or increasing concern regarding the diseases in question. The increases for mammography screening remained significant in the HRS models after adjusting for covariates.
Age Effects
Our data show a consistent age-related pattern of decline for both screening tests in both surveys and for both question periods. This decline might be explained by weak recommendations and little evidence of effect of screening in old women. Possible, but not mutually exclusive, explanations for lack of effect include increasing mortality from competing illnesses, diminishing importance of finding asymptomatic disease in participants with established illness, and reduced probability of living long enough to benefit from the discovery of asymptomatic cancer.
Effect of Objective and Subjective Risk of Mortality on Screening
The decision to obtain cancer screening is an individual one, made with varying amounts of information regarding risk of death by different persons. Our results suggest that both subjective and objective perceptions of mortality risk could play a role. In multivariate models older women with subjective views of their survival likelihood in the middle of the distribution (probability 0.34 to 0.66) were more likely to obtain screening compared with women with lower survival expectations. Reasons for avoiding screening by those in the distribution tails (very pessimistic, very optimistic) might be explained by opposite attitudes: in the first case the women might view such screening as hopeless, in the latter they might view it as unnecessary. The most interesting aspect of our findings with respect to risk perceptions is that survival expectations remain significant predictors even after controlling for many other plausible predictors of screening, suggesting that the women have inside information that is not readily obvious from commonly observed variables. The role of individual perceptions and beliefs about risk warrants more investigation in the study of the use of preventive services generally. It is not clear whether interventions that attempt to change such perceptions are feasible.
Continued Screening in Old Age
Physician actions contributing to screening could reflect a case-by-case basis for screening in these age-groups. Although there is a decline in rates with age, the continuing (and, from 1996 to 2000, apparently increasing) utilization of these screening tests in older age-groups might be excessive.
Based on population data from 1996 and 2000,15,16 the proportion in each age-group reporting having received a screening test in the last 2 years in AHEAD (Table 1⇑) and a cost per mammogram of $100 and a cost of a Pap test of $14.60,17 we estimate that approximately 3.7 million screening mammograms at a total cost of $370 million and 2.8 million Pap tests at a total cost of $41 million were performed in 1996 among women 70 years of age and older. In 2000 the numbers had increased to 4.6 million screening mammograms at a total cost of $460 million and 3.7 million Pap tests at a total annual cost of $47 million among women 70 years of age and older. These costs do not include subsequent follow-up costs for further evaluation and clinical management.
Although both mammography and Pap tests are covered by Medicare and are thus not paid for by the seniors themselves, the societal costs of continuing to perform these tests among the oldest old are substantial. This argument can be made even more strongly for Pap tests than for mammography. Although utilization rates do drop in the oldest age-groups, the low relative rates of mortality from cervical cancer in old age18 should argue for limited cervical screening among the elderly. The continued use might be because some authors still consider the tests useful for women in the oldest age-groups19–,21 despite the lack of evidence from randomized controlled trials.
Walter and Covinsky22 have proposed a framework for when it might be reasonable to screen among the elderly. They suggest basing the screening decision on quantitative estimates of life expectancy, risk of cancer death, and screening outcomes based on published data. According to their framework, patients with a life expectancy of less than 5 years are not likely to have reduced mortality and therefore would not benefit from cancer screening. The potential for harm from a screening (which becomes greater as life expectancy decreases) is also taken into account. Walter and Covinsky recognize that many cancer-screening decisions for the elderly cannot be based on quantitative estimates of benefit and harm that might result from the screening. They therefore also recommend considering the predicted outcomes in accordance with the patient’s own values and preferences for making informed screening decisions.
They estimate that as many as 240 very healthy 80-year-old women need to be screened with mammography to prevent 1 death from breast cancer, and that this number goes up drastically as general life expectancy decreases. They also conclude that elderly women who have had repeated normal Pap smear findings during their reproductive years do not benefit from continued Pap testing. This estimate is consistent with work based on decision modeling.23
Other Factors Predicting Use of Screening
In a study based on the Medicare Current Beneficiary Survey, 26.7% of women older than 75 years were found to have had a mammogram in the last 2 years.24 Mammography was related to functional status and inversely related to age. A smaller study from Connecticut25 concluded that screening mammography might be overused among elderly women, especially among those least likely to benefit, namely, those with a relatively poor general mortality prognosis.
It has been shown that those at higher risk for cancer are less likely to have access to screening than those who are at lower risk,26 and that persons with higher socioeconomic status are more likely to be screened than those with fewer resources.27–,29 Access to health care, insurance, and engaging in other healthy behaviors appear to influence a woman’s likelihood of obtaining a screening mammogram.30 Roberts and Birch31 found that factors affecting screening include insurance type, provider type, long waiting times, and poor communication among the physician, the staff, and the patient. In another mammography study, significant correlates of utilization included age, household income, and the type of managed care organization in which the member was enrolled.32 A study of preventive services and the elderly found that those who had no additional insurance coverage were approximately 10 percentage points less likely to receive influenza vaccination, cholesterol testing, mammography, or Pap smears than those who had such coverage.33
These earlier studies were mostly done among those who were young and middle-aged under the assumption that lower use of screening tests is detrimental. Although this assumption is not as valid in older women, our findings are consistent with these earlier studies. Women who smoke, who are less physically active, who deem their health to be poor or fair, or who have a low subjective life expectation are less likely to be screened. Women who have completed high school, are married, have a higher income, visit their physician more often, and have more health insurance are more likely to be screened. All these findings persist from middle (HRS) to old age (AHEAD). It is particularly noteworthy that the discrepancy for more screening among those with better resources outlasts the equalizing effect of Medicare coverage for these services after the age of 65 years. Generally, these findings are consistent in bivariate analyses and multivariate analyses and for both screening tests.
Strengths and Limitations
Strengths of the study include its large, prospective, representative, national sample of middle-aged and elderly American women, and its inclusion of information on both cancer-screening utilization and predictors for utilization from more than one point in time for each individual.
A limitation is that the screening behavior is based on self-report. Although certain studies conclude that self-report of mammography is generally valid in population studies,34 other authors conclude that self-report might overestimate the receipt of mammography and Pap smears.35–,37 Additionally, although the screening questions were part of the preventive services section of the questionnaires, some women might have reported receipt of a diagnostic (rather than a screening) mammogram. The wording of the questions might also be interpreted somewhat differently by different respondents. Because the wording in the questionnaires refers to the period “within the last two years,” the proportions reporting having received the screening test, as reported in Table 1⇑, are higher than annual rates. Because it is possible that women might have had 1 or more of each test in the last 2 years, we cannot simply halve the reported rates to calculate the annual rates; ie, the corresponding annual rates lie somewhere between our reported rates and one-half of these rates. Given the lack of detail provided from the surveys regarding women’s history and treatment of breast cancer, we were unable to consider women with a history of breast cancer in a separate category for our analysis. Finally, many of the women in these age-groups might have had hysterectomies for benign indications; for elderly women without a uterus, the utility for getting regular Pap tests is likely even smaller than for those with a uterus. Unfortunately, data on whether the survey participants had had a hysterectomy were not collected.
CONCLUSION
Although the use of mammography and Pap tests for screening is lower among older than middle-aged women, elderly women are receiving a large and recently increasing number of screening mammograms and Pap tests. This continued widespread general screening, at substantial societal cost, takes place despite limited scientific evidence of advantage. We believe that information about these screening rates in older women, combined with education about the limited evidence of effect, should be provided to providers. Furthermore, screening among the elderly should be better and more specifically addressed in national clinical guidelines.
Acknowledgments
The authors would like to thank Lynn van Scoyoc for managing and analyzing the data. Thanks to Katrina Krause and Tara Hackney for editing the manuscript.
Footnotes
-
Conflicts of interest: none reported
-
Funding support: This work was supported by a grant from the National Institute on Aging (1RO1-AG-15868).
- Received for publication September 18, 2002.
- Revision received January 6, 2003.
- Accepted for publication January 27, 2003.
- © 2003 Annals of Family Medicine, Inc.
REFERENCES




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Increasing Efforts to Reduce Cervical Cancer through State-Level Comprehensive Cancer Control Planning
- Reversals of Association for Pap, Colorectal, and Prostate Cancer Testing among Hispanic and Non-Hispanic Black Women and Men
- The Break-Even Point: When Medical Advances Are Less Important Than Improving the Fidelity With Which They Are Delivered
- Provocative Questions
- In This Issue: Cervical Cancer Screening