
Article Figures & Data
Figures
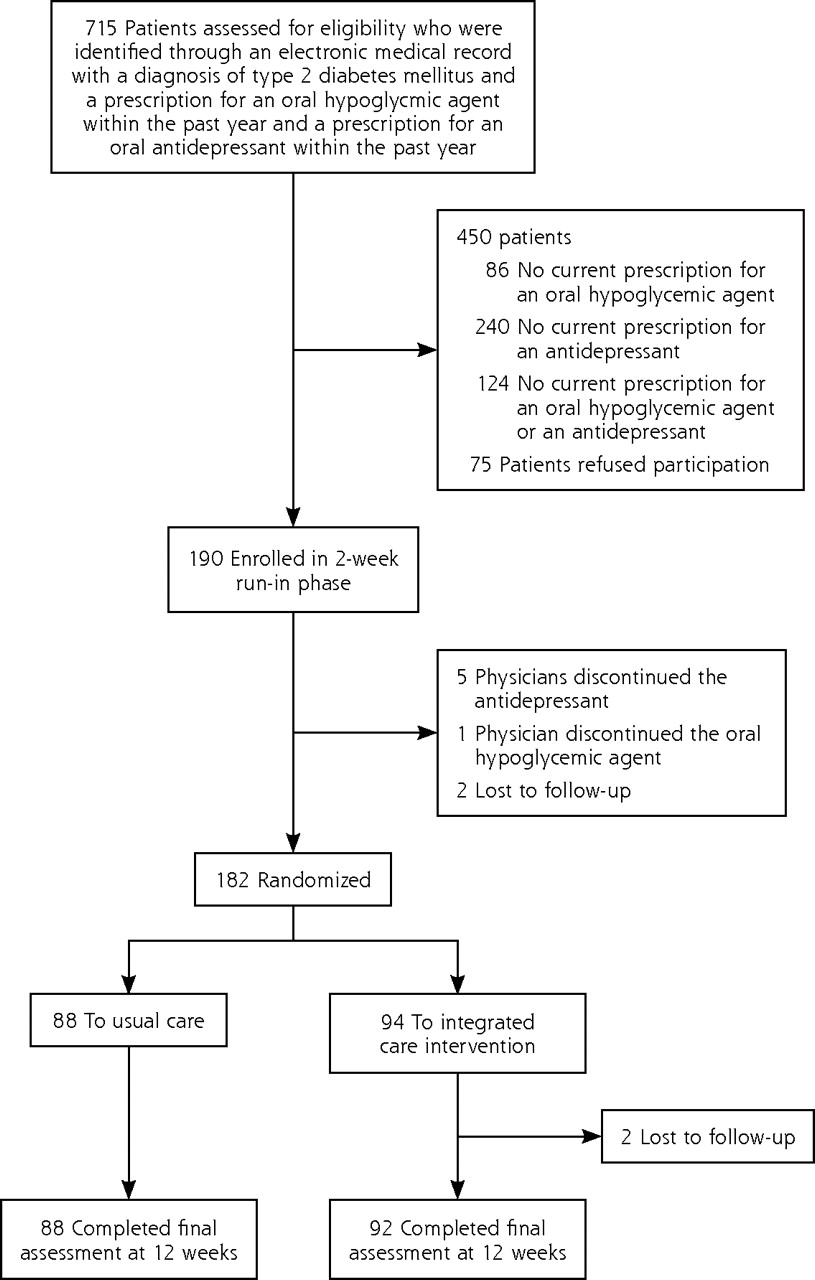
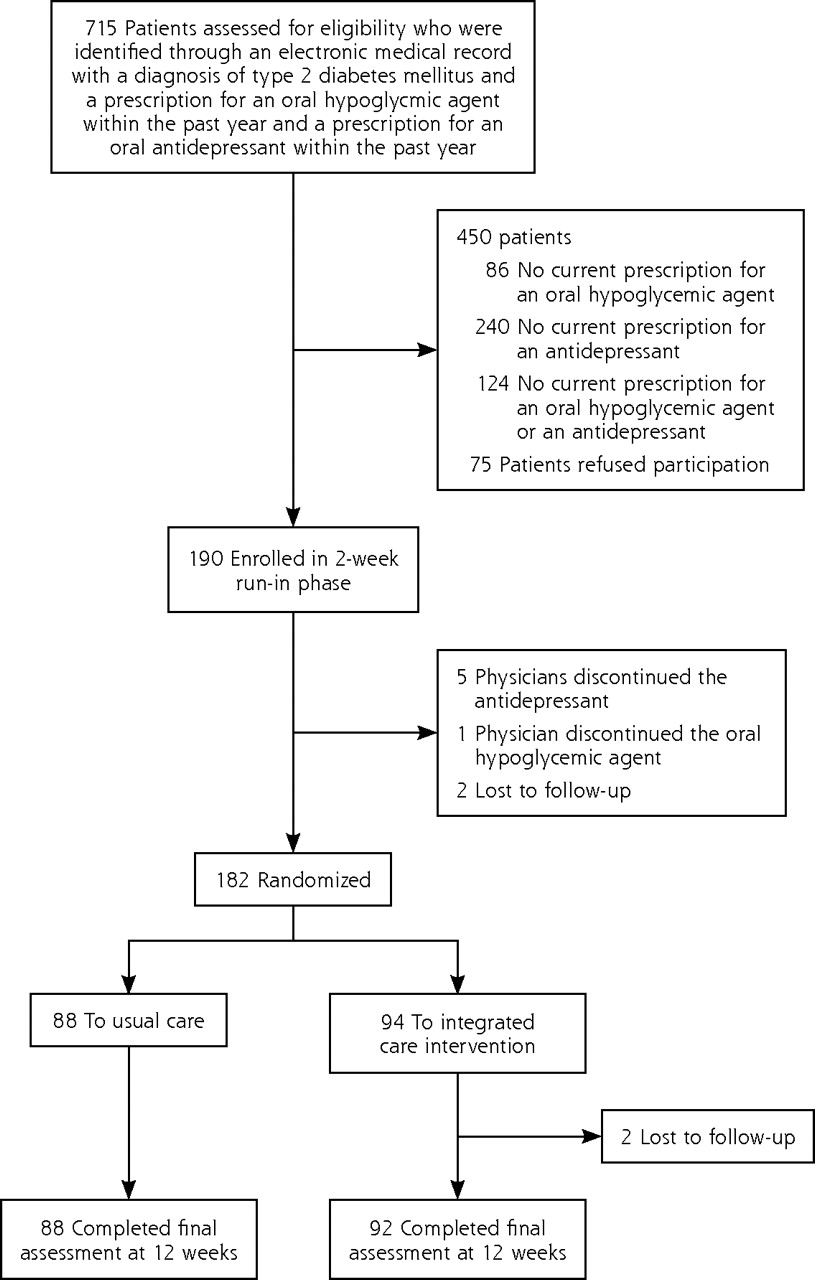
- Figure 1
Study flow diagram.
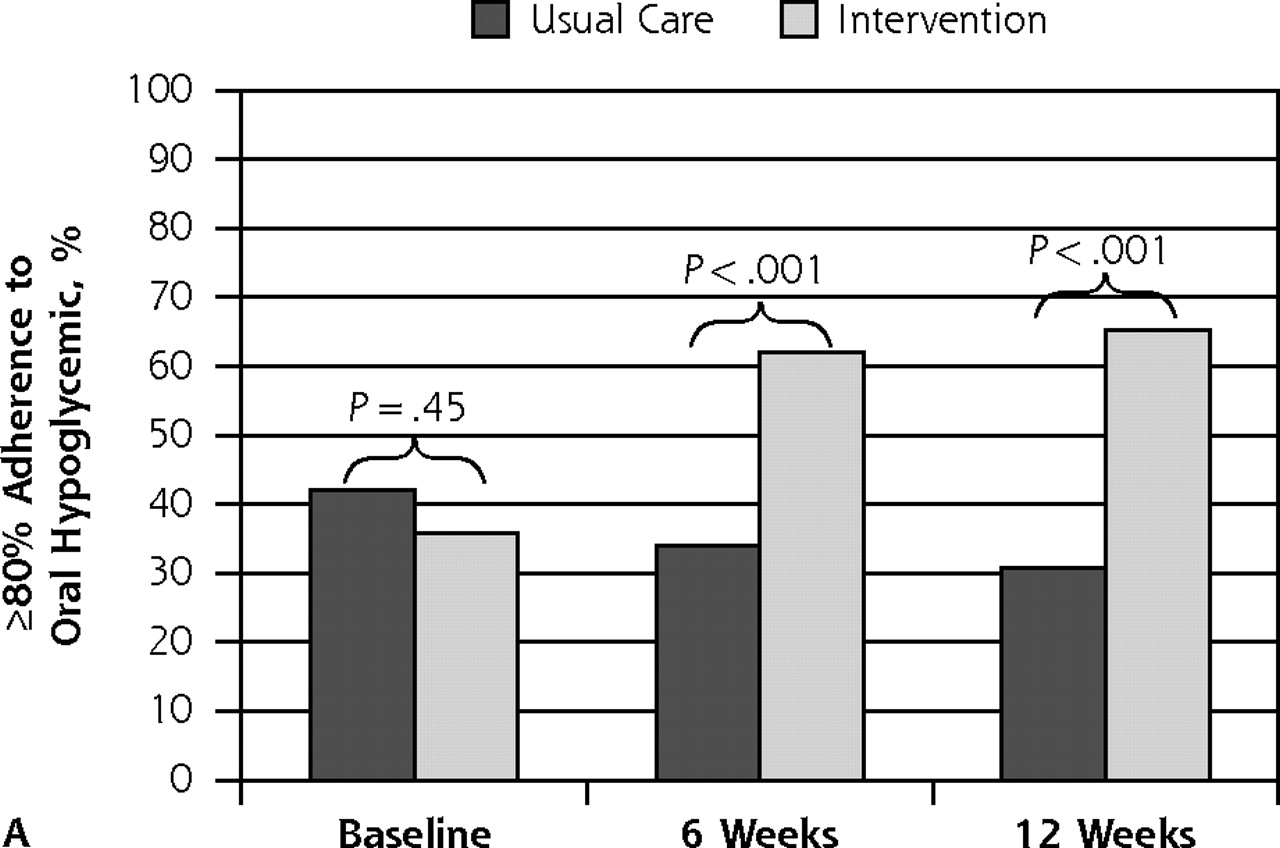
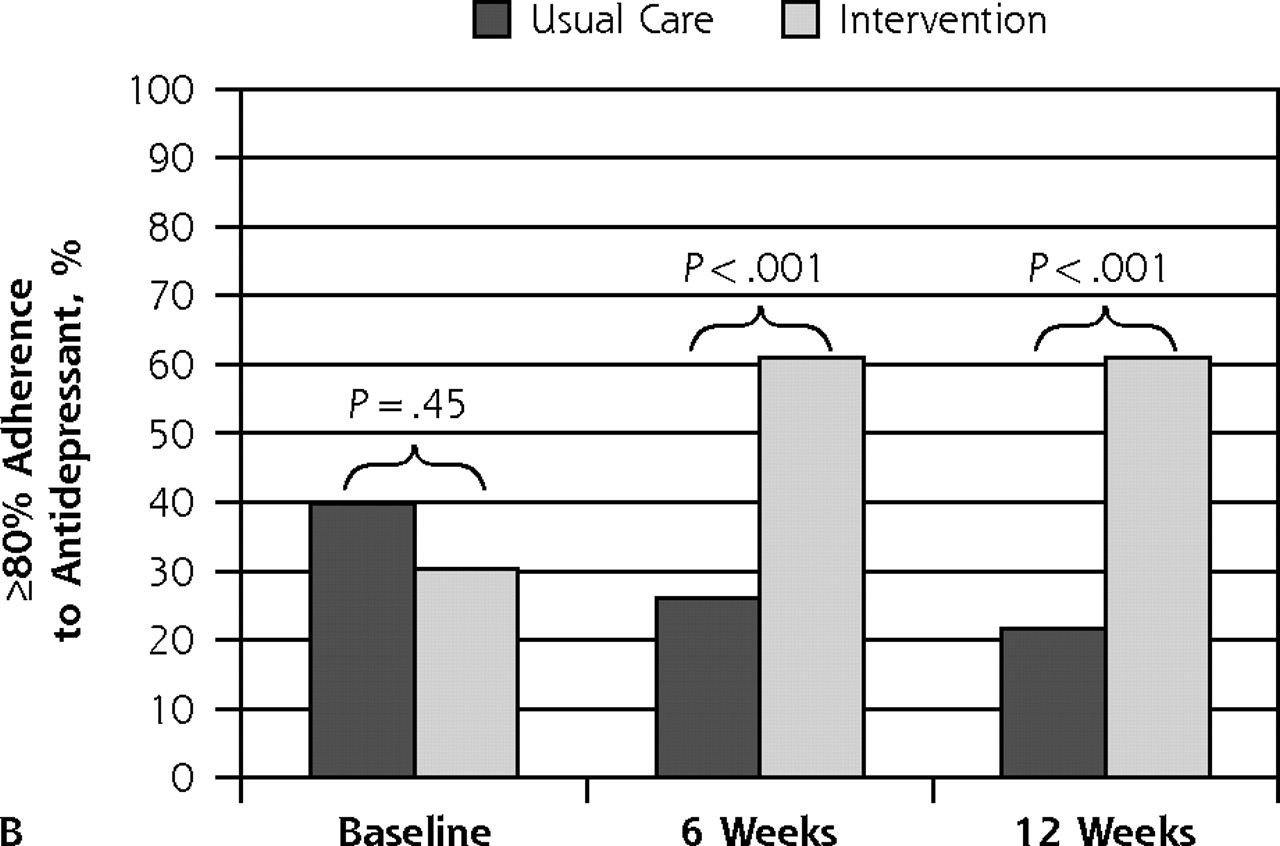
- Figure 2
Patient outcome of ≥80% adherence to oral hypoglycemic agent and to antidepressant medication.
Note: Assessed with the Medication Event Monitoring System at baseline (preintervention) and at 6 and 12 weeks postintervention, according to treatment assignment.


Tables
Characteristic Usual Care (n = 88) Intervention (n = 92) P Value Sociodemographic Age, mean (SD) y 57.1 (9.6) 57.8 (9.4) .63 African American, n (%) 48 (54.5) 54 (58.7) .30 White, n (%) 36 (40.9) 29 (31.5) Hispanic, n (%) 3 (3.4) 4 (4.3) Other, n (%) 1 (1.1) 5 (5.4) Sex, women n (%) 58 (65.9) 64 (69.6) .64 Less than high school education, n (%) 15 (17.0) 14 (15.2) .84 Type 2 diabetes mellitus Years of diabetes, mean (SD) 12.0 (11.8) 10.5 (10.2) .35 HbA1c, mean (SD), % 7.0 (1.9) 7.2 (1.8) .51 Depression PHQ-9 score, mean (SD)a 9.9 (7.2) 10.6 (7.9) .54 Medications Number of medications, mean (SD) 10.1 (5.1) 9.8 (4.5) .66 ≥ 80% adherent to oral hypoglycemic agent, n (%) 37 (42.0) 33 (35.9) .45 ≥ 80% adherent to antidepressant, n (%) 34 (39.0) 28 (30.4) .27 Functional status (SF-36) scoreb Physical function, mean (SD) 53.6 (31.7) 50.8 (32.6) .56 Social function, mean (SD) 67.7 (39.9) 76.6 (36.9) .12 Role physical, mean (SD) 49.4 (46.7) 59.5 (46.6) .15 Role emotional, mean (SD) 65.9 (46.0) 67.8 (44.6) .79 Bodily pain, mean (SD) 42.3 (31.4) 50.9 (31.7) .07 Cognitive status MMSE score, mean (SD)c 28.2 (2.3) 28.2 (2.3) .99 Cardiovascular disease risk factors Systolic blood pressure, mean (SD), mm Hg 132.3 (21.4) 133.9 (20.4) .62 Diastolic blood pressure, mean (SD), mm Hg 77.0 (11.4) 76.6 (11.1) .85 Body mass index, mean (SD) 33.8 (8.3) 34.5 (10.8) .62 LDL cholesterol,d mean (SD), mg/dL 96.9 (27.4) 95.6 (33.4) .77 -
HbA1c = glycated hemoglobin; LDL = low-density lipoprotein; MMSE = Mini-Mental State Examination; PHQ-9 = 9-item Patient Health Questionnaire; SF-36 = Medical Outcomes Study Short Form.
-
Note: P Values represent comparisons according to the Fisher exact test and t tests for categorical or continuous data, respectively.
-
↵a Scored on a range from 0 to 27, where lower scores represent fewer depressive symptoms.
-
↵b Scored on a range from 0 to 100, where lower scores represent functional impairment.
-
↵c Scored on a range from 0 to 30, where lower scores represent cognitive impairment.
-
↵d n = 175 because of missing values.
-
- Table 2
Clinical Outcomes of Glycemic Control and Depression Symptoms in Usual Care and in the Integrated Intervention at 12 Weeks
Outcomes for Type 2 Diabetes Mellitus Unadjusted Estimate Estimated Between-Group Odds Ratio or Difference (95% CI) P Value Usual Care (n = 88) Intervention (n = 92) Glucose control Achieved HbA1c <7%, n (%) 25 (35.7) 67 (60.9) 8.48 (3.24 to 22.2)a <.001 HbA1c, change from baseline, mean (SD) 0.50 (1.11) −0.70 (1.32) −1.20 (−1.56 to 0.84)b <.001 Depression Achieved remission (PHQ-9 <5c), n (%) 27 (30.7) 54 (58.7) 6.15 (2.93 to 12.92)d <.001 PHQ-9 scorec change from baseline, mean (SD) −0.29 (5.74) −2.42 (4.75) −2.13 (−3.68 to −0.59) .007 -
HbA1c = glycated hemoglobin; PHQ-9 = 9-item Patient Health Questionnaire; SD = standard deviation.
-
Estimates, 95% confidence intervals, and P values from the statistical models.
-
↵a Odds ratio (95% CI) from a logistic regression model.
-
↵b Mean group difference (95% CI) from a repeated measures linear regression model.
-
↵c PHQ-9 scored on a range from 0 to 27, where lower scores represent fewer depressive symptoms.
-
↵d Odds ratio (95% CI) from a repeated measures logistic regression model.
-
Supplemental Appendix
Supplemental Appendix. Summary of an Integrated Management of Type 2 Diabetes Mellitus and Depression to Improve Medication Adherence: A Randomized Controlled Trial
Files in this Data Supplement:
- Supplemental data: Appendix - PDF file, 3 pages, 225 KB
The Article in Brief
Hillary R. Bogner , and colleagues
Background Depression is common in patients with diabetes and contributes to poor adherence to medication and dietary regimens, physical inactivity, poor glycemic control, reduced quality of life, disability, and increased health care costs. This study tests the effectiveness of integrated care management of type 2 diabetes and depression compared with usual care services in primary care.
What This Study Found A simple, brief treatment intervention using integration care managers is successful in improving medication adherence and disease outcomes for patients with both depression and type 2 diabetes, a group known to have poor treatment adherence. The intervention integrated depression treatment with type 2 diabetes management and provided an individualized program that recognized the patients� social and cultural context to improve adherence to antidepressants and oral hypoglycemic agents. Patients receiving the integrated care intervention had higher rates of adherence to oral hypoglycemic and antidepressant agents, greater glucose control, and fewer depressive symptoms compared with usual care patients. Specifically, patients receiving the integrated care intervention were more likely to achieve glycated hemoglobin levels of less than 7% and remission of depression when compared with patients in the usual care group.
Implications
- The authors call for an integrated approach to depression and type 2 diabetes treatment.
- This intervention, which has a total contact time of 2 hours, may offer a sustainable solution that can be implemented in primary care for patients managing multiple medical comorbidities with varying degrees of complexity in pharmacotherapy regimens.
Annals Journal Club
Jan/Feb 2012: Beginning to Integrate Care for Diabetes and Depression
The Annals of Family Medicine encourages readers to develop a learning community of those seeking to improve health care and health through enhanced primary care. You can participate by conducting a RADICAL journal club and sharing the results of your discussions in the Annals online discussion for the featured articles. RADICAL is an acronym for Read, Ask, Discuss, Inquire, Collaborate, Act, and Learn. The word radical also indicates the need to engage diverse participants in thinking critically about important issues affecting primary care and then acting on those discussions.1
HOW IT WORKS
In each issue, the Annals selects an article or articles and provides discussion tips and questions. We encourage you to take a RADICAL approach to these materials and to post a summary of your conversation in our online discussion. (Open the article online and click on "TRACK Comments: Submit a response.") You can find discussion questions and more information online at: http://www.AnnFamMed.org/site/AJC/.
CURRENT SELECTION
Article for Discussion
- Bogner HR, Morales KH, de Vries HF, Cappola AR. Integrated management of type 2 diabetes mellitus and depression to improve medication adherence: a randomized controlled trial.Ann Fam Med. 2012;10(1):15-22.
Discussion Tips
Care of people with multiple medical conditions is the norm in family practice.2 Yet, how to integrate, personalize, and prioritize care of multimorbid conditions often is relegated to the art of medicine.3 This study moves beyond a one-disease-at-a-time approach to support the higher order integrative function of primary care.4
Discussion Questions
- What questions are asked by this study, and why do they matter?
- How does this study advance beyond previous research and clinical practice on this topic?
- How strong is the study design for answering the questions?
- Does the registration of the study at http://clinicaltrials.gov increase your confidence in the findings?
- To what degree can the findings be accounted for by:
- How patients were selected, excluded, or lost to follow-up?
- How the main variables were measured?
- Confounding (false attribution of causality because 2 variables discovered to be associated actually are associated with a 3rd factor)?
- Chance? (Optional statistical nerd question: How, other than dichotomizing, might the highly skewed adherence data have been handled?)
- How the findings were interpreted?
- What are the main study findings?
- How comparable is the study sample to similar patients in your practice? What is your judgment about the transportability of the findings?
- What contextual factors are important for interpreting the findings?
- What else do you need to know to optimize care for people with both diabetes and depression?
- How might this study change your practice? Policy? Education? Research?
- Who is affected by the findings, and how might they be engaged in interpreting or using the findings?
- What are the next steps in interpreting or applying the findings?
- What researchable questions remain?
References
- Stange KC, Miller WL, McLellan LA, et al. Annals Journal Club: It's time to get RADICAL. Ann Fam Med. 2006;4(3):196-197.
- Fortin M, Bravo G, Hudon C, Vanasse A, Lapointe L. Prevalence of multimorbidity among adults seen in family practice. Ann Fam Med. 2005;3(3):223-228.
- Stange KC. The generalist approach. Ann Fam Med. 2009;7(3):198-203.
- Stange KC. A science of connectedness. Ann Fam Med. 2009;7(5):387-395.




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Interventions to improve medication adherence in adults with mental-physical multimorbidity in primary care: a systematic review
- A Cluster Randomized Trial of Primary Care Practice Redesign to Integrate Behavioral Health for Those Who Need It Most: Patients With Multiple Chronic Conditions
- A patient-centered comparative effectiveness research study of culturally appropriate options for diabetes self-management
- Randomized Trial of a Tailored Cognitive Behavioral Intervention in Type 2 Diabetes With Comorbid Depressive and/or Regimen-Related Distress Symptoms: 12-Month Outcomes From COMRADE
- Effect of telemedicine on glycated hemoglobin in diabetes: a systematic review and meta-analysis of randomized trials
- Outcomes of Integrated Behavioral Health with Primary Care
- Consequences of Comorbidity of Elevated Stress and/or Depressive Symptoms and Incident Cardiovascular Outcomes in Diabetes: Results From the REasons for Geographic And Racial Differences in Stroke (REGARDS) Study
- Major Depressive Disorder and Bipolar Disorder Predispose Youth to Accelerated Atherosclerosis and Early Cardiovascular Disease: A Scientific Statement From the American Heart Association
- Cognitive Behavioral Therapy Versus Sertraline in Patients With Depression and Poorly Controlled Diabetes: The Diabetes and Depression (DAD) Study: A Randomized Controlled Multicenter Trial
- Personal Accounts of the Negative and Adaptive Psychosocial Experiences of People With Diabetes in the Second Diabetes Attitudes, Wishes and Needs (DAWN2) Study
- Depression in Adults in the T1D Exchange Clinic Registry
- Collaborative care for comorbid depression and diabetes: a systematic review and meta-analysis
- A Randomized Controlled Trial of Cognitive Behavioral Therapy for Adherence and Depression (CBT-AD) in Patients With Uncontrolled Type 2 Diabetes
- Simplifying Care for Complex Patients
- In This Issue: Challenges of Managing Multimorbidity
- Beginning to Integrate Care for Diabetes and Depression