
Abstract
PURPOSE Routine assessment of women's pregnancy intentions and contraceptive use—a so-called contraceptive vital sign—may help primary care physicians identify patients who need preconception or contraceptive counseling and be of particular benefit when teratogenic medications are prescribed.
METHODS We conducted a cluster-randomized controlled trial to evaluate the effect of a contraceptive vital sign on primary care documentation of contraceptive use and change in primary care physicians' provision of family planning services. Academic internists in the intervention group (n = 26) were provided with information on their female patients' pregnancy intentions and contraceptive use immediately before visits; internists in the control group (n = 27) received only standard intake information. Data were abstracted from the electronic health record for 5,371 visits by 2,304 women aged 18 to 50 years.
RESULTS Documentation of contraception increased from baseline, from 23% to 57% in the intervention group, but remained 28% in the control group, a change of +77.4 (95% confidence interval [CI], 70.7 to 84.1) adjusted percentage points in the former vs +3.1 (95% CI, 1.2 to 5.0) in the latter (P <.001). For visits involving a teratogenic prescription, documentation increased from 14% to 48% in the intervention group and decreased from 29% to 26% in the control group, a change of +61.5 (95% CI, 35.8 to 87.1) adjusted percentage points in the former vs −0.3 (95% CI, −4.3 to 3.6) in the latter (P <.001). Provision of new family planning services increased only minimally with this intervention, however. When women with documented nonuse of contraception were prescribed potential teratogens, only 7% were provided family planning services.
CONCLUSIONS A contraceptive vital sign improves documentation of contraceptive use; however, ongoing efforts are needed to improve provision of preconception and contraceptive services.
INTRODUCTION
Women whose medical condition or medication use may increase the risk of adverse pregnancy outcomes need preconception guidance and contraceptive counseling to reduce the risk of unintended pregnancy and optimize pregnancy timing. One-half of US pregnancies remain unintended,1 however, and family planning services are provided during only 5% to 20% of visits made by women prescribed potentially teratogenic medications.2 As a result, approximately 6% of US pregnancies are exposed to potentially teratogenic class D or X medications.3
As the majority of potentially teratogenic medications are prescribed by primary care physicians,2,4 there is a particular need for these physicians to provide preconception and contraceptive counseling. Primary care physicians have reported that one barrier to safe prescribing to women of reproductive age is difficulty ascertaining their pregnancy intentions, and they have expressed interest in strategies for routinely assessing chance of pregnancy.5,6 Obtaining a so-called contraceptive vital sign, similar to efforts to assess pain as a vital sign,7, 8 could help prompt preconception counseling.
In this study, we evaluated the feasibility and efficacy of this type of routine intake assessment of women's pregnancy intentions and contraceptive use on the documentation of contraception and primary care physicians' provision of family planning services. We hypothesized that a contraceptive vital sign would increase documentation of contraception and increase provision of family planning services, especially for women prescribed potentially teratogenic medications.
METHODS
Setting and Participants
We conducted a cluster-randomized trial between October 2008 and April 2010 to evaluate the introduction of a contraceptive vital sign in a large, academic general internal medicine practice that has collected patient-entered intake information (eg, alcohol use, physical activity, last menstrual period) using wirelessly networked tablet computers since 2004. These computers use branched logic to select appropriate intake questions for each patient. The computer synthesizes and formats the information into a paper report for physicians.9,10 All primary care physicians at this practice were invited to participate. As this practice is a residency training site, participating physicians were both residents and supervising physicians. This study was approved by the University of Pittsburgh Institutional Review Board.
Intervention Design
Physicians were randomized to an intervention group or control group. When female patients aged 18 to 50 years were scheduled to see intervention physicians, a pair of questions asking about pregnancy intentions and recent contraceptive use—the contraceptive vital sign—were added to their intake questionnaire. Specifically, they were asked “Are you currently pregnant or trying to become pregnant?” and provided with 6 response options: “no,” “not trying to get pregnant but wouldn't mind being pregnant,” “trying to get pregnant,” “currently pregnant,” “been through menopause,” and “prefer not to answer.” Women who responded either “no” or “not trying to get pregnant…” were then asked: “There are many ways that people try to avoid becoming pregnant. Which are you using?” and were provided with a list of contraceptive methods. Response options included “no method of birth control,” “not sexually active with men in the past 3 months,” and “prefer not to answer.” If a patient reported that she was pregnant, trying to become pregnant, wouldn't mind becoming pregnant, or trying to avoid pregnancy but not using any contraception, the intake report provided to physicians included the warning statement “Consider chance of pregnancy when prescribing” in bold text, unless the woman responded that she had not had sex within the past 3 months. The decision to consider women abstinent for 3 months as at low risk of pregnancy reflected the majority opinion of this practice's clinicians. Patients previously indicating that they were menopausal or had undergone hysterectomy or tubal ligation were not asked the questions. Also, because of a programming error, women making annual preventive visits were not asked the questions.
Patients seeing control physicians were asked only the standard intake questions. This study was conducted in conjunction with the introduction of clinical decision support integrated into the clinic's electronic health record (EHR), which alerted physicians when they initiated a prescription for a potentially teratogenic medication.
Data Collection
We reviewed deidentified EHR data from all visits by women aged 18 to 50 years who started to complete a computerized intake questionnaire during a baseline period (May 2007-September 2008) and the intervention period (October 2008-April 2010). Abstracted data included evidence of new contraceptive prescriptions; referrals for placement of an intrauterine contraceptive, contraceptive implant, or diaphragm; contraceptive counseling received within the past 3 months; prior contraceptive prescriptions or devices that were still active; pregnancy tests; potentially teratogenic medications prescribed at the visit; type of clinical encounter (new vs return, usual physician vs other); and patients' age, race, and marital status. Responses to the contraceptive vital sign questions were extracted from the tablet computers and linked to EHR data by an honest broker. We eliminated all visits with evidence of sterilization, menopause, or infertility, as well as all annual preventive visits, which did not receive the intervention as planned. Additionally, because the intake system provides physicians with information patients have given at previous visits, in a small number of cases, control physicians inadvertently received contraceptive vital sign information from previous visits with intervention physicians; we also eliminated these “crossover” visits.
Statistical Analysis
Intervention and control physicians were compared using χ2 tests and Wilcoxon rank sum tests, and the characteristics of visits made to the 2 groups during the baseline period were compared using mixed-effects models with random effects to address clustering by physician and patient. We calculated the response rate and range of responses to each of the contraceptive vital sign questions. We calculated the proportion of visits in each study group with documentation of contraception, overall and for the subgroup of visits involving the prescription of a potential teratogen, at baseline and during the intervention.
To test whether there was significantly different change in documentation in the intervention group, we constructed visit-level generalized linear mixed-effects models with a repeated time measure adjusting for visit characteristics including patient characteristics (aged ≥30 years, married, white), and physician characteristics (sex, resident, receipt of clinical decision support when prescribing a potential teratogen). The models contained an interaction term to test whether changes over time differed significantly between groups.11 Using nearly identical models, we also investigated whether the contraceptive vital sign affected the rate of prescription of potentially teratogenic medications and provision of new family planning services (ie, new contraception prescriptions, contraceptive counseling, pregnancy testing, or referral to a family planning specialist). Models predicting documentation of contraception included a random effect for patients only, as this information was collected before seeing the physician. Models predicting physician prescribing and counseling behavior included a random effect for physician only, as models containing crossed random effects for physicians and patients would not converge. We also tested models adjusting only for patient clustering, but the difference between the models was not appreciable.
From each model, we estimated the adjusted absolute change in the outcome over time and the 95% confidence interval (CI) (holding covariates at their grand means). Finally, we calculated the residual intraclass correlation coefficient (ICC) for provision of teratogenic prescriptions and family planning services.12
Community-Based Extension
As an extension of this trial, we pilot tested the use of a similar intake system in a community-based family practice. Given the smaller number of primary care physicians in this practice (N = 13), implementation was not randomized by physician; rather, the front desk staff randomly requested that 10% of women use the new intake system. We therefore compared rates of potentially terato-genic prescriptions among women who were and were not asked to provide the contraceptive vital sign and investigated whether provision of new family planning services when potential teratogens were prescribed was higher among visits involving the contraceptive vital sign.
All analyses were conducted using Stata version 11 IC (StataCorp LP); P values less than .05 were considered significant.
RESULTS
Figure 1 shows the flow of participating primary care physicians and visits. We abstracted data from 11,621 visits. We eliminated 1,834 visits with women who had evidence of sterilization, menopause, or infertility (16% of all visits; 22% of visits with a potentially teratogenic prescription). We also eliminated 158 visits in which a control physician inadvertently received contraceptive vital sign information entered on a previous visit and 4,258 annual preventive visits, leaving 5,371 visits made by 2,304 unique women. There were no significant differences in physician characteristics between groups (Table 1).
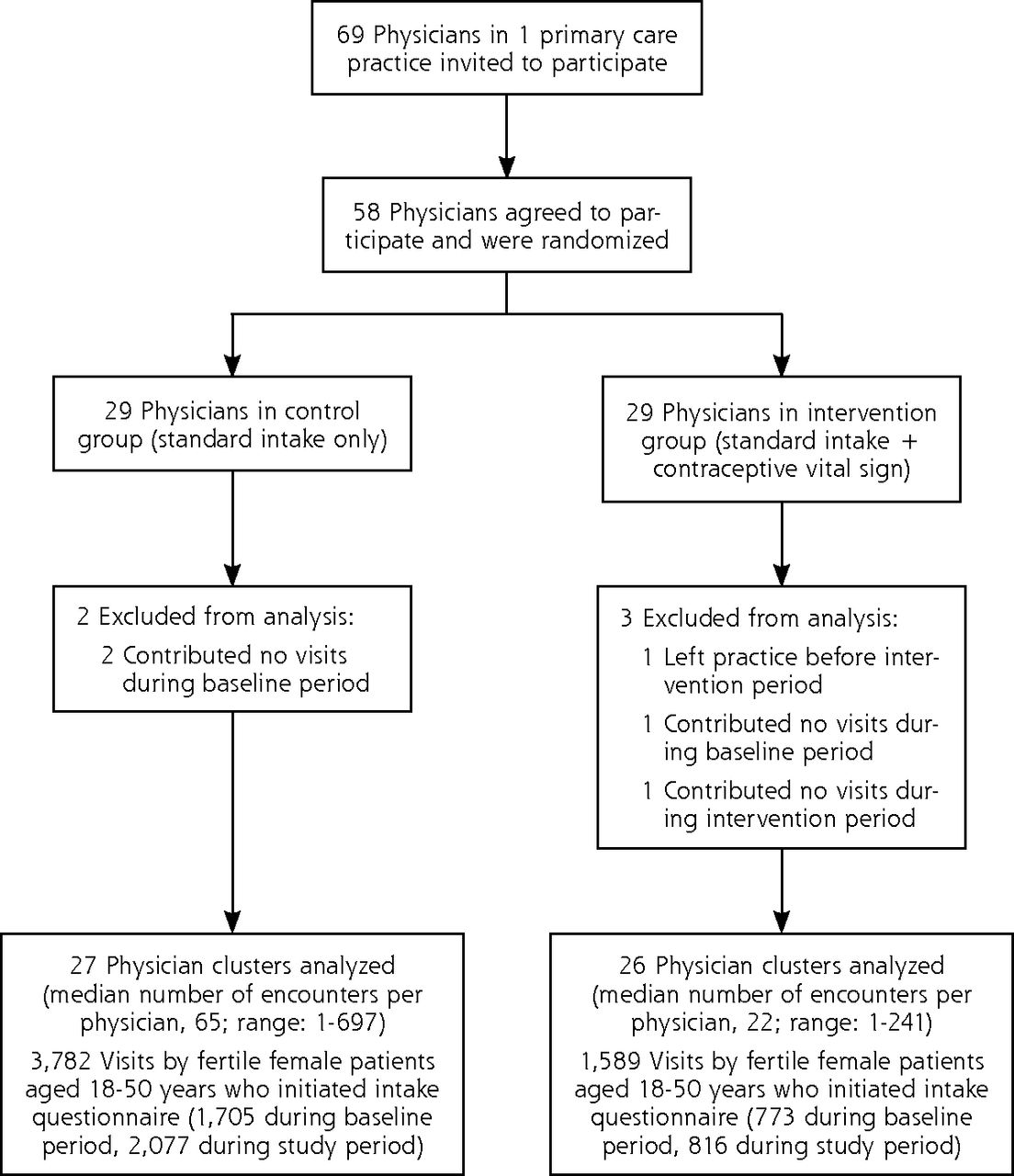
Flow diagram describing physician clusters and patient encounters from the time of recruitment to analysis.
Feasibility and Acceptability of the Intervention
During the 816 visits in which women were asked the contraceptive vital sign questions, 93% provided answers. The remaining 7% either skipped the question or did not finish the questionnaire. In total, intervention physicians were notified to “consider chance of pregnancy when prescribing” in 13.5% of visits (110 of 816) in which contraceptive vital sign data were collected. Responses to the contraceptive vital sign questions are given in Table 2.
Efficacy of the Intervention
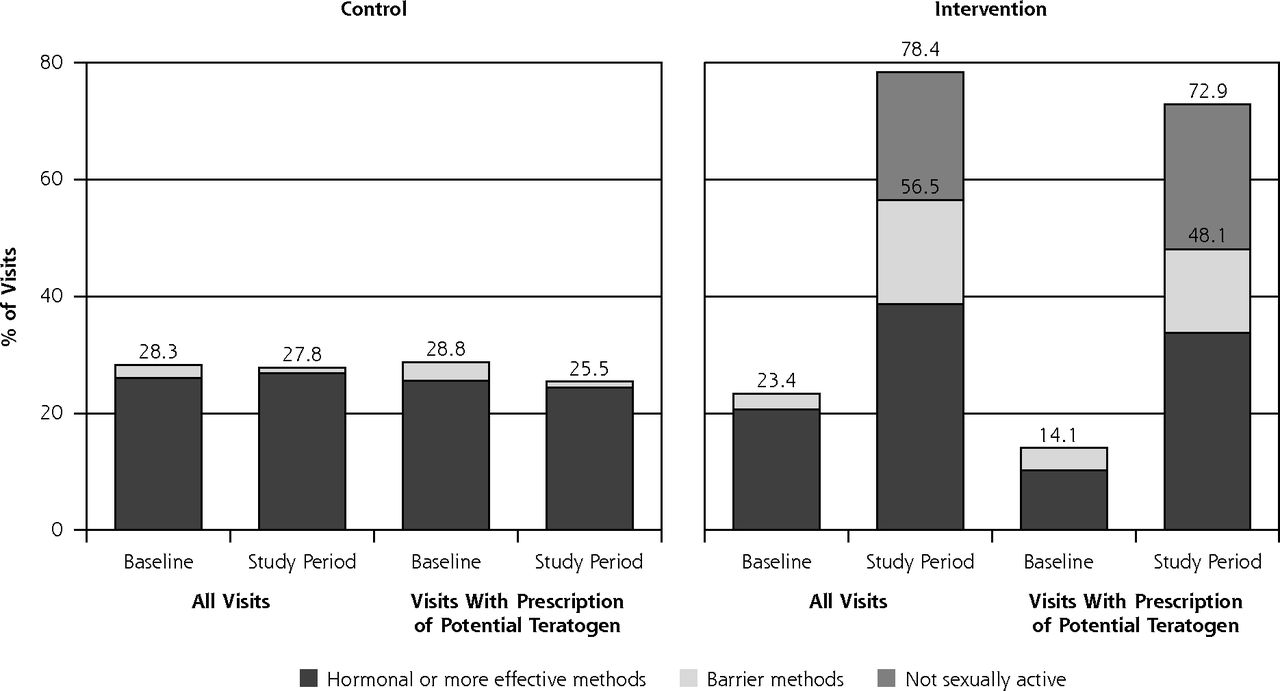
Figure 2 displays the proportion of visits with documented use of contraception before and during the intervention period, for all visits as well as the subgroup of visits with a potentially teratogenic prescription. There was significantly greater improvement in documentation in the intervention group compared with the control group: +77.4 (95% CI, 70.7 to 84.1) adjusted percentage points in the former vs +3.1 (95% CI, 1.2 to 5.0) in the latter (P <.001). A similar increase was seen among visits with a teratogenic prescription: +61.5 (95% CI, 35.8 to 87.1) adjusted percentage points vs −0.3 (95% CI, −4.3 to 3.6; P <.001). The contraceptive vital sign increased documentation of use of hormonal or more effective methods (ie, intrauterine devices, implants, and vasectomies), as well as barrier methods. It also provided additional information about which women had not been sexually active in the past 3 months.
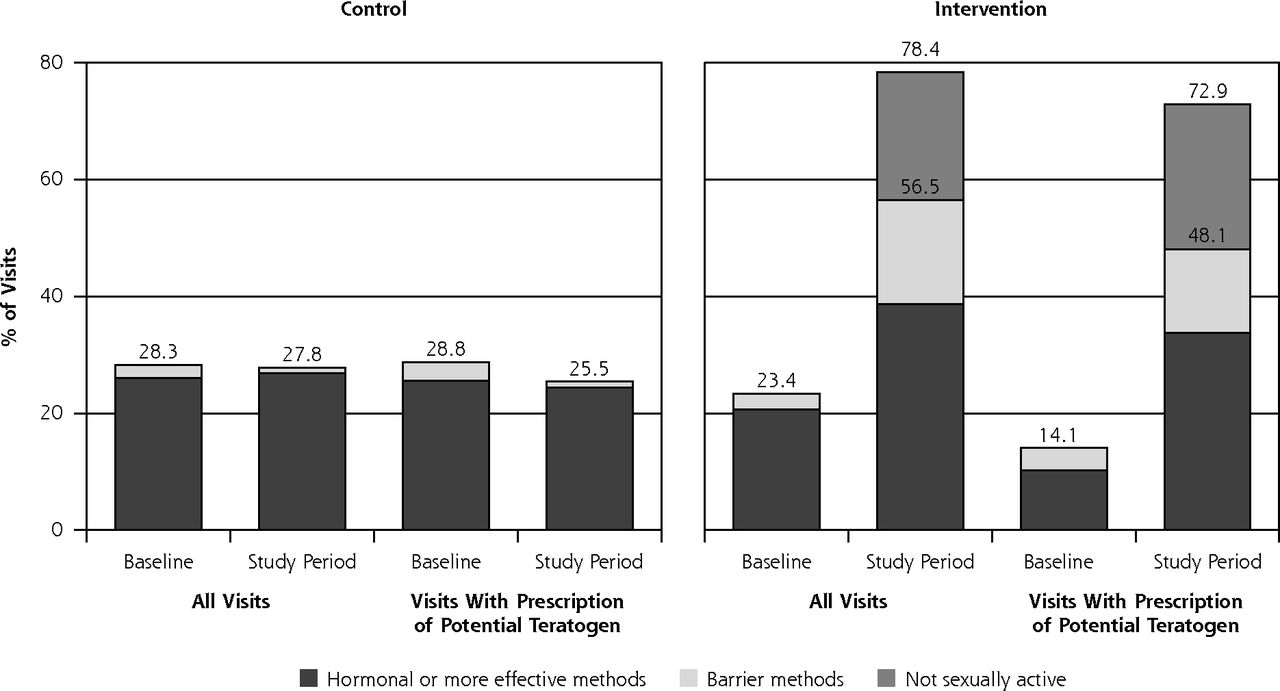
Change in proportion of visits with medical record documentation of contraception before and after introduction of the contraceptive vital sign.
Notes: Contraceptive vital sign data and electronic health record data were collected between October 1, 2008, and April 14, 2010. Baseline electronic health record data from the 17 months before introduction of the contraceptive vital sign were used for comparison. In generalized linear mixed-effects models, there was a greater increase in documentation of contraception in the intervention group compared with the control group, both for all visits (P <.001) and visits that involved prescription of potentially teratogenic medications (P <.001). Hormonal or more effective methods = pill, patch, ring, injection, intrauterine devices, subdermal contraceptiveimplants, and vasectomies. Women who had been sterilized were excluded. Not sexually active = women who reported no sex with a man in past 3 months.
At baseline, 14% of intervention visits and 18% of control visits included prescriptions for potentially teratogenic medications (P <.01). After introduction of the contraceptive vital sign, there was little change in the rate of teratogenic prescriptions for either group: +2.6 (95% CI, –0.8 to +6.0) adjusted percentage points in the intervention group vs −0.4 (95% CI, −3.0 to +2.0) in the control group (P = .1). At baseline, family planning services were provided at 9% of intervention visits and 11% of control visits (P = 1.0). After introduction of the contraceptive vital sign, intervention physicians were not significantly more likely to provide new family planning services than control physicians: +0.3 (95% CI, −2.8 to 3.3) vs −1.4 (95% CI, −3.3 to 0.4) adjusted percentage points (P = .3). The ICC was 0.01 (95% CI, –0.01 to 0.03) for potentially teratogenic prescriptions and 0.03 (95% CI, 0.002 to 0.048) for family planning services.
Among the visits with potentially teratogenic prescriptions, at baseline, family planning services were provided at 7% of intervention visits and 12% of control visits (P = .7). Again, however, there was only minimal increase in provision of new family planning services by intervention physicians: +3.3 (95% CI, −5.4 to 12.0) adjusted percentage points in the intervention group vs −1.7 (95% CI, −6.6 to 3.3) in the control group (P = .3). The ICC for family planning services was less than 0.001 (95% CI, –0.02 to 0.02) in this subgroup of visits with prescription of potential teratogens.
Of the 133 visits to intervention physicians during the study period that involved prescription of a potential teratogen, 17% still had no documentation of the patient's contraceptive status (either because they did not complete the contraceptive vital sign questions [9%] or responded “prefer not to answer” [8%]), and 11% had documentation of nonuse of contraception. Of the 14 visits with documentation of contraceptive nonuse, only 1 (7%) received a referral for family planning services; none received pregnancy testing or a new contraceptive prescription.
At the community-based family practice, new family planning services were provided during 9% of visits, whether or not contraceptive vital sign data were collected. Visits with contraceptive vital sign data were significantly less likely to include prescriptions for teratogenic medications: –3.8 (95% CI, –7.1 to –0.3) adjusted percentage points (P = .03). But visits with potential teratogens were not more likely to include provision of new family planning services when contraceptive vital sign data were collected: –3.2 (95% CI, –6.3 to –0.1) adjusted percentage points (P = .04).
DISCUSSION
This study found that routine collection of contraceptive vital sign data was acceptable to the large majority of women served by 2 primary care practices and significantly improved documentation of contraception. The intervention had minimal impact on documented provision of family planning services, however, and a substantial number of patients prescribed potentially teratogenic medications were found to remain at risk for unintended pregnancy. Although the intervention was designed to limit primary care physicians' liability when a potential teratogen was prescribed, it may have inadvertently increased liability when contraceptive nonuse was explicitly documented alongside a potentially teratogenic prescription.
This randomized intervention took place in an academic general internal medicine practice that trains residents and has established an efficient electronic intake system. These findings thus may not be generalizable to all primary care settings; however, results from our pilot study in a community-based family practice were similar. Compared with general internists, family physicians see a larger proportion of female patients of reproductive age,2,13 receive more training in reproductive health, and report being more comfortable providing routine gynecologic care and initiating contraception.14 Nationally, family physicians tend to provide contraceptive counseling more frequently than general internists (10.2% of visits to former vs 6.4% of visits to latter).2 Family physicians are somewhat less likely to prescribe potentially teratogenic medications (6.4% vs 8.0% of visits).2 Nonetheless, provision of appropriate counseling when teratogenic medications are prescribed remains a considerable challenge for both family physicians and general internists, as primary care physicians generally have lower levels of contraceptive knowledge than gynecologists.15-17
Recently an extensive educational intervention was shown to increase family practice residents' documentation of contraceptive counseling when prescribing teratogenic medications from 20% to 37%.18 In a similar study, documentation of contraceptive counseling rose from 46% to 80% of family practice visits involving a teratogenic medication,19 although the authors were unable to be certain that this was the result of their intervention as documentation of contraception had been rising before the intervention and there was no control group. A major strength of our study is its randomized controlled design. Also, although it took place in a practice that uses an electronic intake system, contraceptive vital sign data could easily be assessed by nursing staff or using a paper intake system.
As primary care physicians frequently discuss contraception during annual preventive visits, it is unfortunate that a programming error excluded these visits from our study, and the final sample size was smaller than intended. With only 110 visits that included a warning message, we had limited power to detect significant improvement in physician behaviors. Although the majority of clinicians in the study clinic felt that women who had not been sexually active in the last 3 months were at low risk for pregnancy, some of these women may have resumed sexual activity after filling a teratogenic prescription and might have benefited from contraceptive counseling. As more than one-third of women see both a primary care physician and gynecologist,20 we would have liked to ask women if they wanted to discuss birth control with their primary care physician; however, concerns about the length of the intake questionnaire precluded the addition of more than the 2 questions we studied at this time. Additionally, as primary care physicians have little incentive to code for provision of counseling services and we did not review physician notes from these visits, physicians likely provided preconception and contraceptive counseling more often than is reflected in the EHR data. A study by Gilchrist et al21 suggests that 71% of visits wherein contraceptive counseling occurs lack documentation of this counseling. As some physicians who felt pressured for time may have planned to provide such counseling at a follow-up visit, the fact that we examined data from only 1 visit may underestimate the intervention's true effect. Additionally, we have no way of verifying that physicians in either the general medicine or family practice reviewed the contraceptive vital sign data that was provided, as they were not instructed to look for it or to document counseling in the EHR.
In conclusion, a contraceptive vital sign improves primary care documentation of pregnancy intentions and contraception in a manner that is acceptable to patients. Prior research indicates that women prescribed teratogenic medications prefer to hear about the risks of these medications directly from their prescribing physician,22 and provision of contraceptive counseling in primary care has been associated with increased likelihood of contraceptive use.23 Ongoing efforts are needed, however, to ensure that primary care patients receive preconception counseling and family planning services, and that the provision of these services is documented in the EHR, particularly when potentially teratogenic medications are prescribed.
Acknowledgments
Funding support: This study was funded by AHRQ R18HS017093 and NICHD K23HD051585. Ms Williams was supported by a grant from the Doris Duke Charitable Foundation to the University of Pittsburgh.
Footnotes
-
Conflicts of interest: authors report none.
-
To read or post commentaries in response to this article, see it online at http://www.annfammed.org/content/10/6/516.
-
Previous presentation: A poster describing a preliminary analysis of this data was presented at the Reproductive Health Conference in Atlanta, GA, on September 22-25, 2010.
-
Trial Registration: ClinicalTrials.gov Identifier: NCT00766207
- Received for publication August 24, 2011.
- Revision received December 21, 2011.
- Accepted for publication February 22, 2012.
- © 2012 Annals of Family Medicine, Inc.




{kind=link}
{kind=link}