
Article Figures & Data
Figures
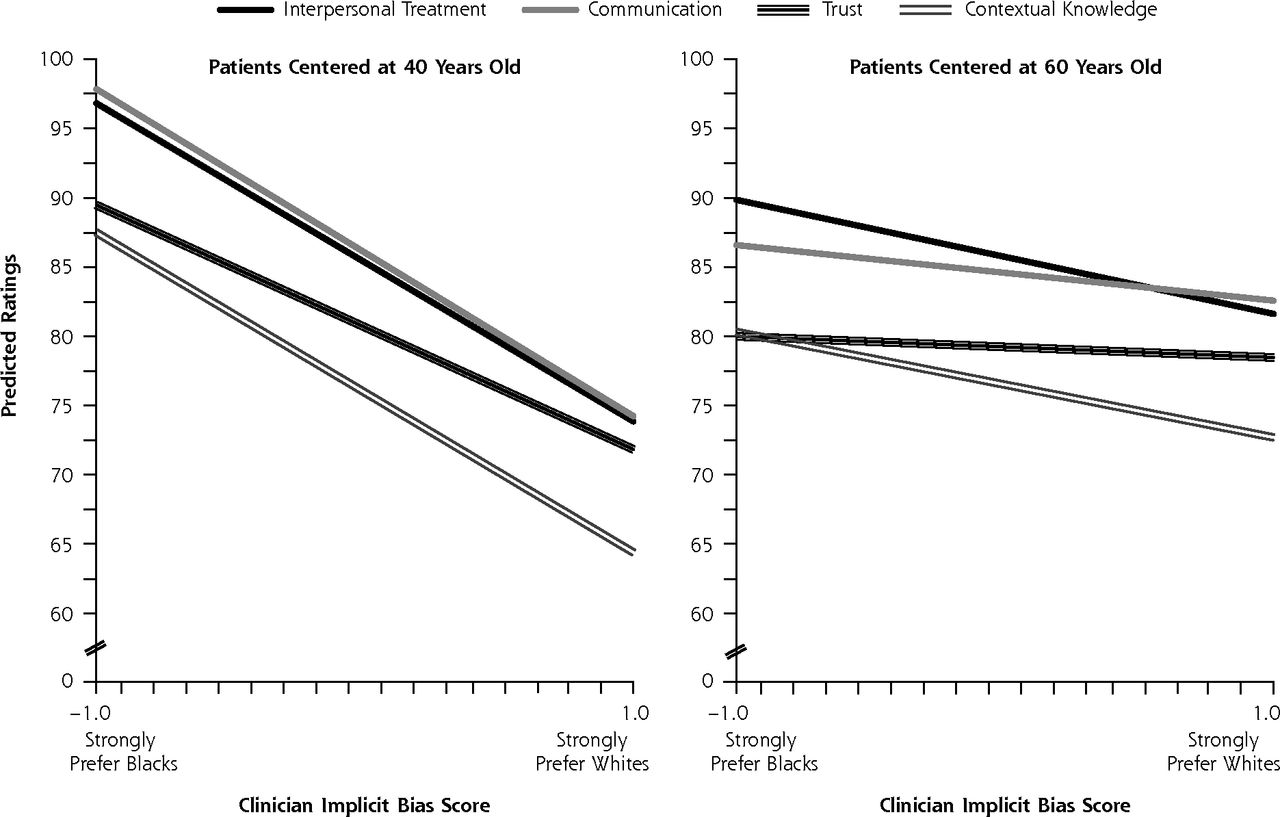
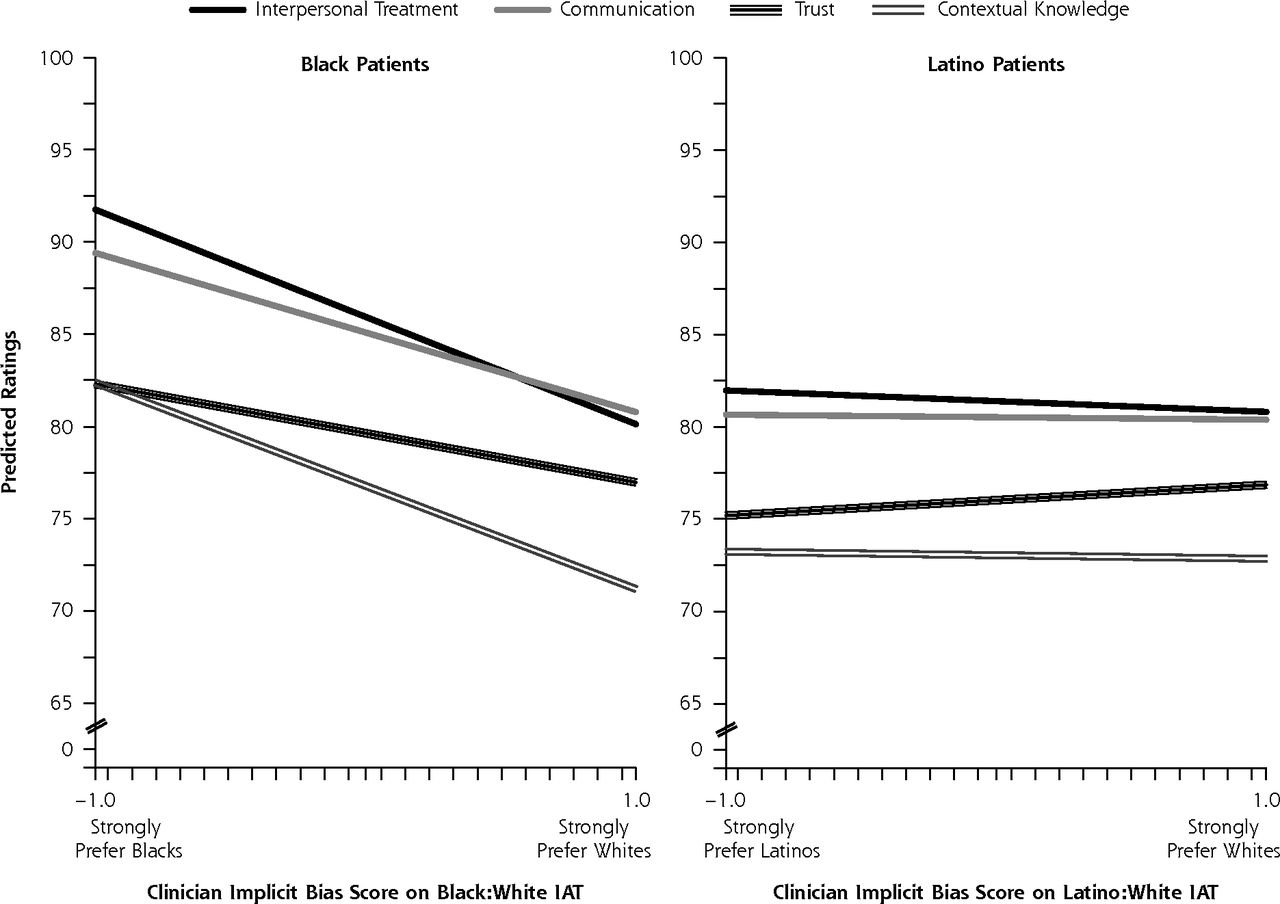
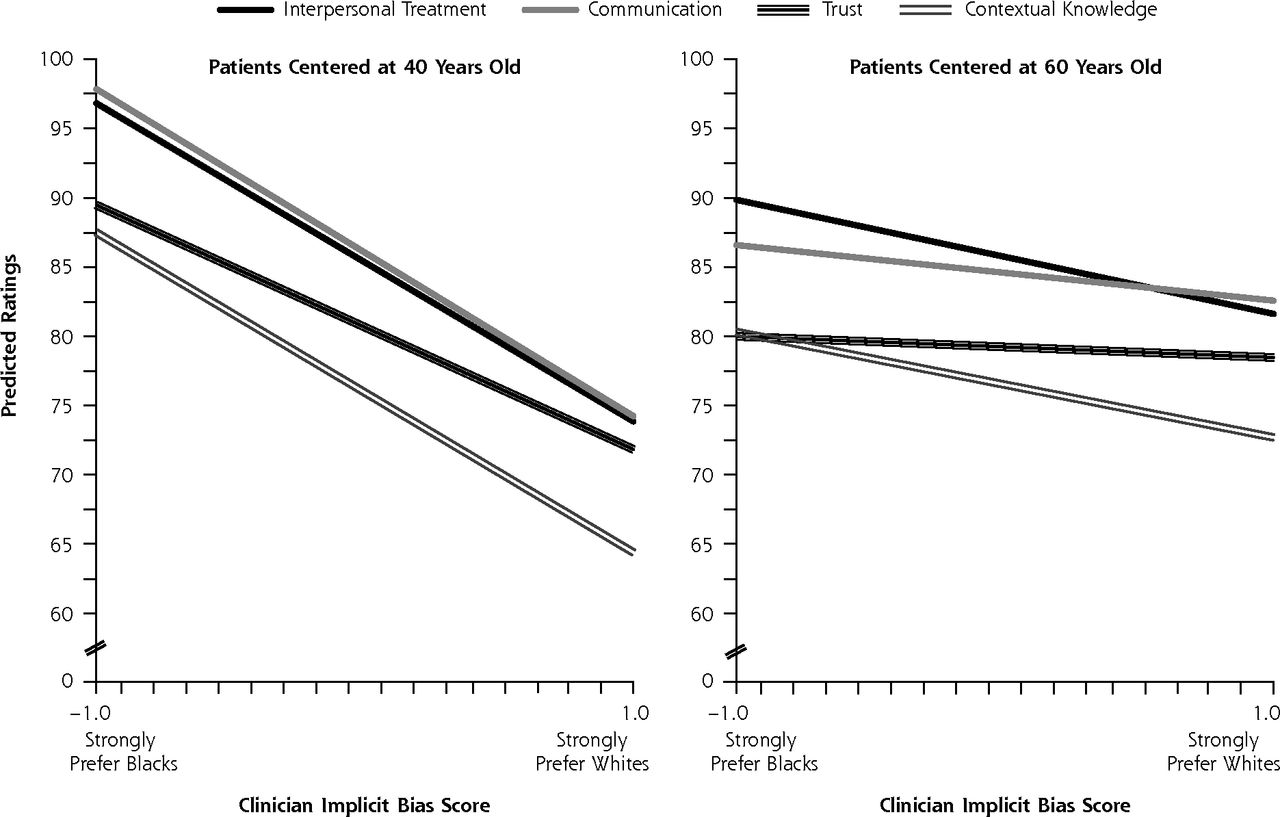
- Figure 1
Predicted ratings of clinicians as a function of their implicit bias (IAT) score and their patients’ ethnicity/race. White patients always served as the reference group (data not shown).
IAT = Implicit Association Test.
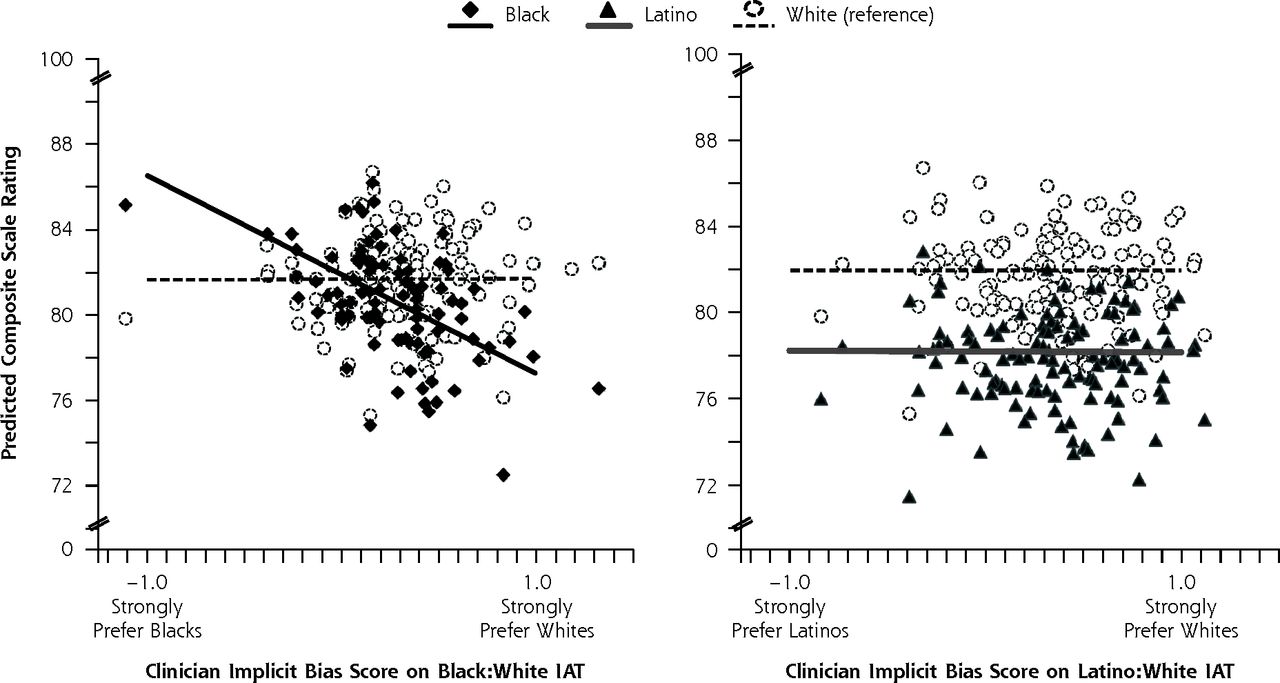
- Figure 2
Predicted composite scale ratings by black, Latino, and white (reference) patients for individual clinicians with specific IAT scores.
IAT = Implicit Association Test.
Note: The lines show the overall (unconditional) estimate of the relation between clinician implicit bias scores and predicted patient ratings. The symbols show the individual (conditional) estimates for each clinician with a specific IAT score by each ethnic/racial patient group.
- Figure 3
Predicted ratings of clinicians by younger and older black patients, as a function of clinicians’ implicit bias score on the Black:White IAT.
IAT = Implicit Association Test.


Tables
Recruitment Sample Final Patient Sample by Ethnicity/Race (N = 2,908) Characteristic Nonparticipants (n = 3,221) Participants (n = 2,908) Black (n = 612) Latino (n = 859) White (n = 1,437) Female, No. (%)a,b 1,690 (52) 1,694 (58) 369 (60) 539 (63) 786 (55) Age, No. (%)a,b 18–35 y 108 (3) 67 (2) 25 (4) 29 (3) 13 (1) 36–55 y 1,115 (36) 973 (33) 234 (38) 314 (37) 425 (30) ≥56 y 1,958 (61) 1,868 (64) 353 (58) 516 (60) 999 (70) Ethnicity/race, No. (%)a Black 560 (17) 612 (21) – – – Latino 1,146 (36) 859 (30) – – – White 1,515 (47) 1,437 (49) – – – Education, No. (%)b High school not completed – 529 (18) 91 (15) 355 (42) 83 (5) High school diploma or GED – 773 (27) 185 (30) 237 (28) 351 (24) 1–3 y college – 866 (30) 215 (35) 167 (19) 484 (34) ≥4 y college – 714 (24) 118 (20) 88 (11) 508 (35) Unknown – 26 (1) 3 (<1) 12 (1) 11 (1) Household income, No. (%)b ≤$15,000 – 1,026 (35) 274 (45) 396 (46) 356 (25) $16,000–$35,000 – 555 (19) 133 (22) 184 (21) 238 (17) $36,000–$55,000 – 408 (14) 68 (11) 88 (10) 252 (18) ≥$56,000 – 717 (25) 100 (16) 124 (14) 493 (34) Unknown – 202 (7) 37 (6) 67 (8) 98 (7) Language proficiency,c No. (%)b Spanish > English – 268 (9) 5 (1) 260 (30) 3 (<1) Alternate category – 2,640 (91) 607 (99) 599 (70) 1,434 (>99) Proportion of primary care visits with clinician, No. (%)b .50–.59 520 (16) 446 (15) 85 (14) 137 (16) 224 (16) .60–.69 530 (16) 471 (16) 84 (14) 133 (15) 254 (18) .70–.79 552 (17) 519 (18) 99 (16) 161 (19) 259 (18) .80–.89 644 (20) 594 (20) 144 (24) 182 (21) 268 (19) .90–1.0 975 (30) 878 (30) 200 (33) 246 (29) 432 (30) Visits with clinician in 3 y, mean No. (SD)a,b 7.38 (5.35) 7.81 (5.70) 8.16 (6.05) 8.51 (5.91) 7.23 (5.36) Years with clinician, mean No. (SD) – 3.40 (1.07) 3.35 (1.09) 3.37 (1.16) 3.45 (1.00) GED = general equivalency degree. -
↵a Participants and nonparticipants differ, P < .05.
-
↵b Ethnic/racial groups differ, P < .05.
-
↵c Greater proficiency in Spanish than English was assigned if (1) patients completed the questionnaire in Spanish instead of English, or (2) patients reported on the questionnaire that they were fluent in Spanish and less than fluent in English.
-
Score, Mean (SD) Scale (α) and Description Black Latino White Subscalea Interpersonal treatment (α = .94); 5 items on the clinician’s patience, friendliness, caring, respect, and time spent with the patient 84 (19) 81b (19) 86 (18) Communication (α = .93); 6 items on the thoroughness of the clinician’s questions, attention to the patient, clarity of explanations and instructions, and help in making decisions about care 84 (18) 80b (19) 84 (17) Trust (α = .85); 8 items on the clinician’s integrity and role as the patient’s agent in the system 79b (16) 76b (15) 82 (15) Contextual knowledge (α = .90); 5 items on the clinician’s knowledge of the patient’s medical history, life responsibilities, principal health concerns, and values and beliefs 75 (19) 73 (20) 74 (20) Composite (α = .93); average of all 4 subscales weighted equally 80 (16) 78b (17) 82 (16) - Table 3
Effects of Ethnic/Racial Group and Interactions Between Group and Clinicians’ Implicit Bias on Patients’ PCAS Ratings of the Clinicians
PCAS Score by Scale, Estimate (SE) Predictor Interpersonal Treatment Communication Trust Contextual Knowledge Composite Intercept (average rating by white patients) 85.69 (0.57) 84.45 (0.56) 81.88 (0.47) 74.36 (0.62) 81.62 (0.52) Black patients Group (black vs white) 0.24 (1.11) 0.64 (1.10) –2.25 (0.93)a 2.42 (1.22)a 0.20 (1.00) Group × clinicians’ implicit bias –5.81 (2.52)a –4.31 (2.47)b –2.65 (2.09) –5.58 (2.73)a –4.61 (2.25)a Latino patients Group (Latino vs white) –4.30 (0.97)c –3.93 (0.96)c –5.85 (0.81)c –1.31 (1.06) –3.86 (0.87)c Group × clinicians’ implicit bias –0.58 (1.71) –0.13 (1.68) 0.85 (1.42) –0.19 (1.86) –0.04 (1.53)
The Article in Brief
Clinicians' Implicit Ethnic/Racial Bias and Perceptions of Care Among Black and Latino Patients
Irene V. Blair , and colleagues
Background Bias can be explicit or implicit. Explicit bias is overt and freely expressed; implicit bias may not be consciously acknowledged and operates in more subtle ways. Clinicians are unlikely to directly express ethnic/racial bias yet may still deliver care that is influenced by unrecognized bias. In this study, patients evaluate the degree to which their clinicians are patient-centered during their interactions. Researchers then examine those evaluations in terms of patients' ethnicity/race and the clinicians' implicit and explicit ethnic or racial bias.
What This Study Found Clinicians with higher levels of implicit ethnic or racial bias are rated less favorably by black patients than are clinicians with lower levels of implicit bias. Surveys of nearly 3,000 patients found black patients rated clinicians who had greater implicit bias against blacks lower in patient-centered care than they did clinicians with little or no such implicit bias. Latino patients' ratings were not correlated to clinicians' implicit bias, though they tended to give clinicians lower ratings overall than did other groups.
Implications
- Clinicians' implicit bias may jeopardize their clinical relationships with black patients, which could have negative effects on other care processes, including adherence to medical advice.
- The authors conclude these findings support the Institute of Medicine's suggestion that clinician bias may contribute to health disparities. They note that implicit bias is malleable, and they encourage interventions that may help render bias less implicit and unconscious, thereby fostering real reflection, analysis, and change.




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Trends and Disparities in Newer GLP1 Receptor Agonist Initiation among Real-World Adult Patients Eligible for Obesity Treatment
- County-level racial bias is associated with worse care for white and especially black older US adults: a cross-sectional observational study
- Investigating Unconscious Race Bias and Bias Awareness Among Vascular Surgeons
- Storylines of family medicine X: standing up for diversity, equity and inclusion
- Le racisme comme determinant de la sante et des soins de sante: Sommaires narratifs des donnees probantes produits par le projet SAFE pour les etablissements de sante
- Racism as a determinant of health and health care: Rapid evidence narrative from the SAFE for Health Institutions project
- Diversity, equity and inclusion in acute care surgery: a multifaceted approach
- Discrimination and Medical Mistrust in a Racially and Ethnically Diverse Sample of California Adults
- Color-Blind Racial Attitudes in Dental Hygiene Students: A pilot study
- Nonverbal synchrony as a behavioural marker of patient and physician race-related attitudes and a predictor of outcomes in oncology interactions: protocol for a secondary analysis of video-recorded cancer treatment discussions
- Placebo effects and racial and ethnic health disparities: an unjust and underexplored connection
- Study protocol for investigating physician communication behaviours that link physician implicit racial bias and patient outcomes in Black patients with type 2 diabetes using an exploratory sequential mixed methods design
- Color-Blind Racial Beliefs Among Dental Students and Faculty
- Talking With Patients Is Better Than Talking to Patients
- Texas Medicaid Payment Reform: Fewer Early Elective Deliveries And Increased Gestational Age And Birthweight
- Shared Goal Setting in Team-Based Geriatric Oncology
- The Effects of Oncologist Implicit Racial Bias in Racially Discordant Oncology Interactions
- Social Determinants of Risk and Outcomes for Cardiovascular Disease: A Scientific Statement From the American Heart Association
- Unconscious Biases: Racial Microaggressions in American Indian Health Care
- In This Issue: How We Think and Feel Influences Patient Care