
Article Figures & Data
Figures
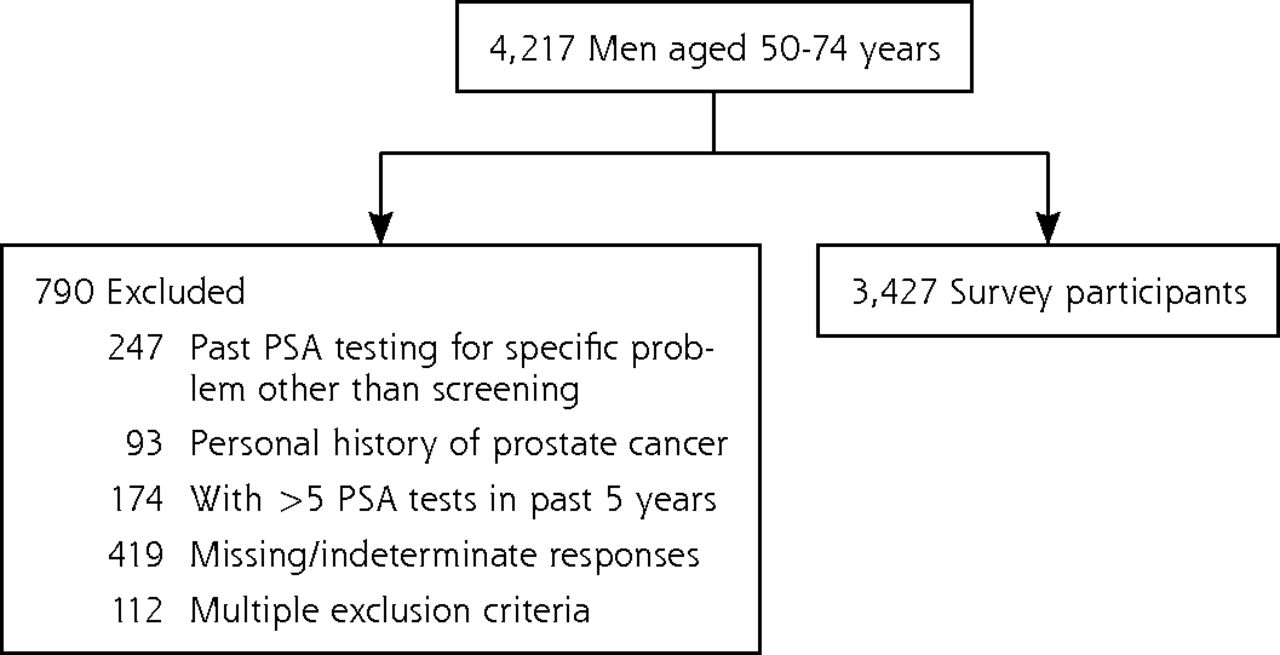
- Figure 1
Study population of men aged 50–74 years, National Health Interview Survey, 2010.
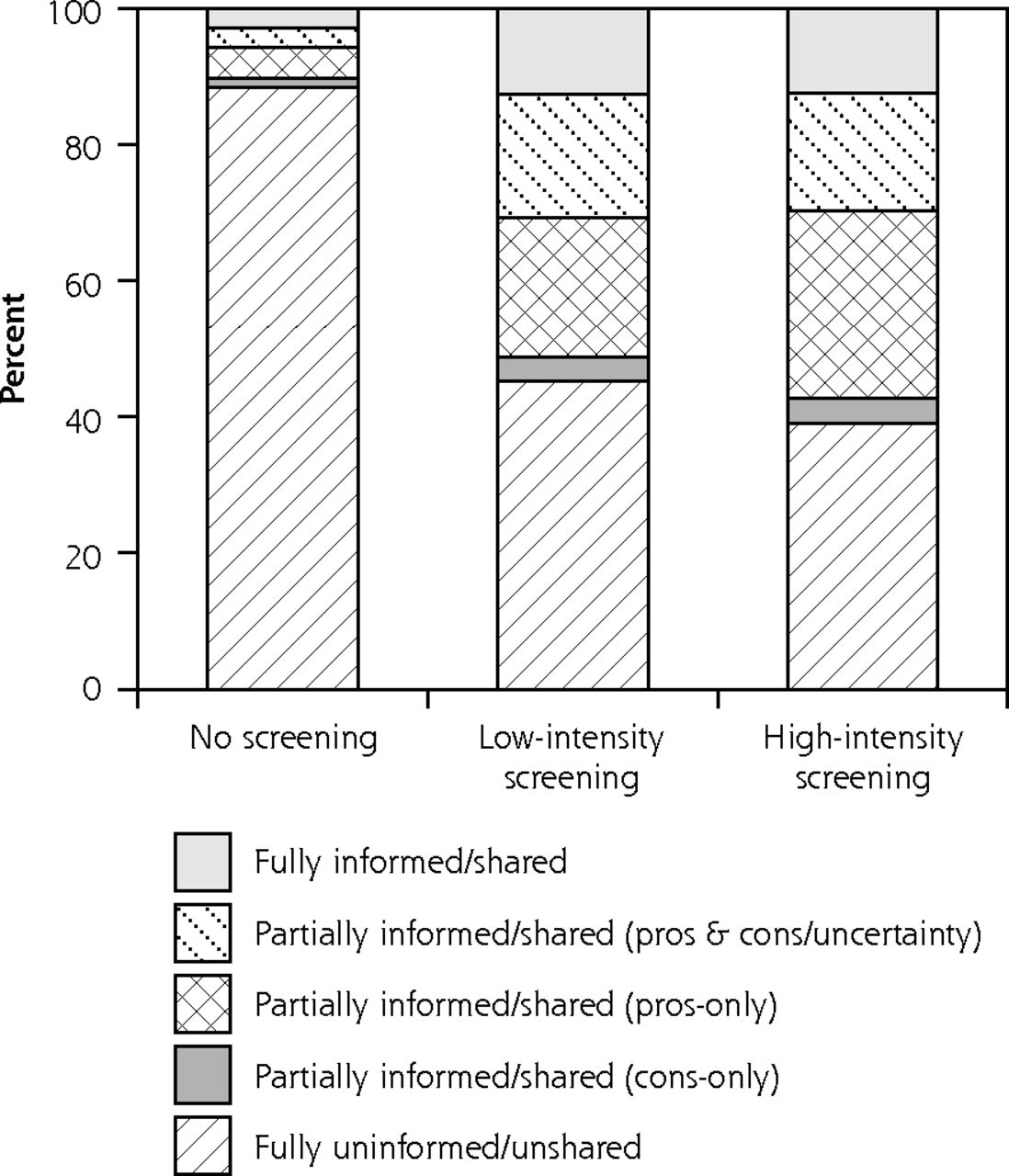
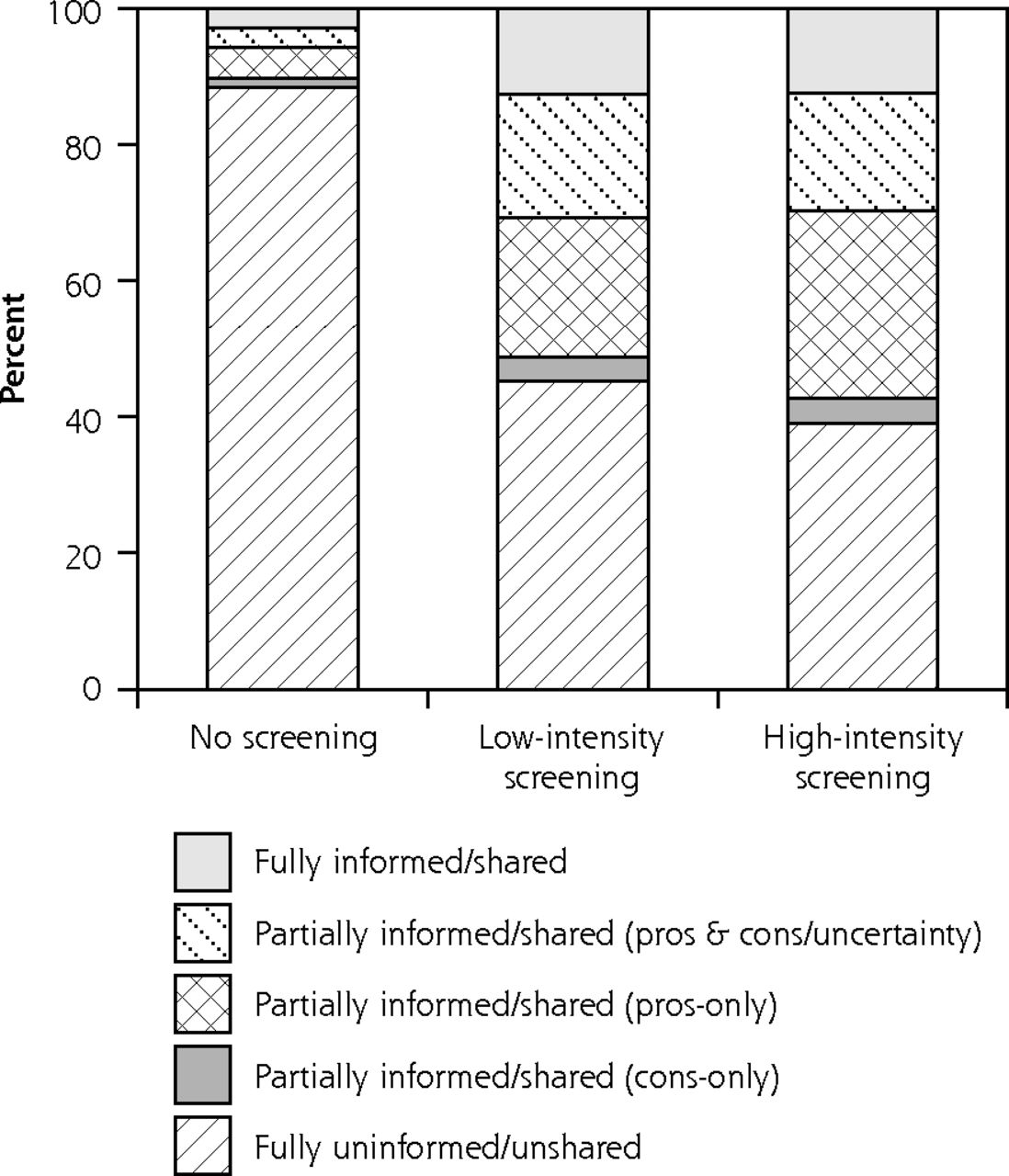
- Figure 2
Extent of shared decision making by intensity level of PSA screening, 2010 National Health Interview Survey
PSA=prostate-specific antigen.
Notes: Extent of shared decision making (unadjusted percentages) according to the physician’s discussion of the following elements: advantages, disadvantages, and uncertainty. Fully informed is discussion of all elements. Partially informed/shared (pros+cons/uncertainty) is discussion of advantages and disadvantages or advantages and uncertainty. Partially informed/shared (pros-only) is discussion of advantages only. Partially informed/shared (cons-only) is discussion of disadvantages only, disadvantages and uncertainty, or uncertainty only. Fully uninformed/unshared is no discussion of decision-making elements. PSA screening intensity levels are as follows: no screening = no past history; low-intensity = 1–3 tests in past 5 years; high-intensity = 4–5 tests in past 5 years.

Tables
- Table 1
Characteristics of Study Population (N = 3,427), 2010 National Health Interview Survey
Characteristic, No. Responding Percenta Age, years, N=3,427 50–59 54.0 60–69 36.1 70–74 9.9 Race, N=3,427 White 85.0 Black 9.9 Other 5.1 Ethnicity, N=3,427 Hispanic 9.8 Non-Hispanic 90.2 Education, n=3,415 <High school graduate 15.0 High school graduate 26.2 Some college/technical school 25.5 College grad 33.3 Poverty ratio, N=3,427 <200% 20.7 200%–299% 11.9 300%–399% 10.2 400%–499% 10.1 ≥500% 30.0 Unknown 17.1 Health insurance, n=3,422 None 11.3 Public only 16.7 Private/military 71.9 Usual source of medical care, n=3,425 Yes 88.1 No 11.9 Reported health status, N=3,427 Excellent 22.8 Very good 29.8 Good 29.5 Fair or poor 17.9 Family history of prostate cancer, N=3,427 Yes 6.8 No/unknown 93.2 Chronic diseases, n=3,412 None 39.4 1 33.4 2 18.2 ≥3 9.0 Cancer, n=3,421b Yes 5.9 No 94.1 Doctor recommended PSA screening, n=3,417 Yes 52.5 No 47.5 Ever had a PSA test, N=3,427 Yes 55.8 No 44.2 Date of last PSA test, n=1,826 ≤1 Year ago 65.5 >1 But less than 5 years ago 29.0 >5 Years ago 5.6 Screening intensity (PSA tests in 5 y), n = 3,355 None 47.1 1–3 (low intensity) 27.8 4–5 (high intensity 25.1 -
PSA=prostate-specific antigen.
-
Note: Respondents were men aged 40 to 75 years with no prior PSA testing or who had PSA testing as part of routine examination; not all categories sum to 3,427 because of missing data.
-
↵a Percentages weighted to the US civilian noninstitutionalized population.
-
↵b Excluding prostate and nonmelanoma skin cancer.
-
- Table 2
Prevalence of Elements of Shared Decision Making in PSA Screening Study Population (N=3,427), 2010 National Health Interview Survey
Element, No. Responding Percenta Discussion of advantages/disadvantages, n = 3,344 None 65.1 Advantages only 16.9 Disadvantages only 0.9 Both 17.0 Discussion of uncertainty, n = 3,344 Yes 12.1 No 87.9 Extent of shared decision making,b n=3,304 No elements 64.3 Partial, disadvantages only, disadvantages and uncertainty, or uncertainty only 2.5 Partial, advantages only 14.6 Partial, advantages and disadvantages or advantages and uncertainty 10.7 All elements 8.0 -
PSA=prostate-specific antigen.
-
Note: Respondents were men aged 40–75 years with no prior PSA testing or who had PSA testing as part of routine examination (N = 3,427); not all categories sum to 3,427 because of missing data.
-
↵a Percentages weighted to the US civilian noninstitutionalized population.
-
↵b Physician discussion of the following elements: advantages, disadvantages, and uncertainty.
-
- Table 3
Factors Associated with PSA Screening Intensity,a 2010 National Health Interview Survey
Factor Low Intensity vs No Screeninga
OR (95% CI)bHigh Intensity vs No Screening
OR (95% CI)bP Valuec Age, year <.001 50–59 1.0 1.0 60–69 1.41 (1.07–1.86) 2.95 (2.12–4.11) 70–74 1.54 (0.90–2.65) 4.59 (2.68–7.87) Education .002 <High school graduate 1.0 1.0 High school graduate 1.37 (0.90–2.08) 1.56 (0.84–2.89) Some college/technical institute 1.00 (0.64–1.56) 1.68 (0.95–2.96) College graduate 1.58 (0.97–2.57) 2.92 (1.55–5.49) Usual source of medical care <.001 Yes 1.0 1.0 No 0.46 (0.29–0.74) 0.15 (0.06–0.38) Doctor recommendation <.001 Yes 44.10 (31.68–61.41) 107.37 (71.42–161.41) No 1.0 1.0 Extent of shared decision makingd <.001 No elements 1.0 1.0 Partial, disadvantages only, disadvantages and uncertainty, or uncertainty only 3.84 (1.24–11.91) 4.87 (1.48–16.02) Partial, advantages only 2.38 (1.53–3.71) 3.22 (1.94–5.35) Partial, advantages and disadvantages or advantages and uncertainty 3.97 (1.82–8.68) 3.82 (1.67–8.69) All elements 1.98 (0.97–4.04) 1.96 (0.93–4.11) -
↵a PSA Screening intensity: “no screening” = no prior testing; “low intensity” = 1–3 tests/past 5 years; “high intensity” = 4–5 tests/past 5 years
-
↵b Confidence interval from multivariable polytomous logistic regression model with PSA screening as the dependent variable (n = 3,209); analyses adjusted for race, ethnicity, poverty ratio, self-reported health status, number of chronic diseases, personal history of cancer, family history of prostate cancer, health insurance.
-
↵c P value for Wald χ2 test for association.
-
↵d Physician discussion of the following elements: advantages, disadvantages, and uncertainty.
-
- Table 4
Factors Associated with Physician-Patient Discussion of Advantages and Disadvantages of PSA Screening and Uncertainty About PSA Screening, 2010 National Health Interview Survey
Discussion of Advantages and Disadvantagesa Discussion of Uncertaintyb Factor Advantages or Disadvantages vs No Discussion
OR (95% CI)Advantages and Disadvantages vs No Discussion
OR (95% CI)P Valuec Uncertainty vs No Discussion
OR (95% CI)P Valuec Race <.001 White 1.0 1.0 – Black 1.09 (0.76–1.56) 2.47 (1.73–3.53) – Other 0.99 (0.60–1.64) 1.34 (0.79–2.28) – Ethnicity .005 – Hispanic 1.16 (0.75–1.79) 2.03 (1.32–3.13) – Non-Hispanic 1.0 1.0 – Education <.001 <High school graduate – – – 1.0 High school graduate – – – 1.44 (0.81–2.57) Some college/technical school – – – 1.27 (0.70–2.30) College graduate – – – 2.61 (1.49–4.58) Health insurance .002 None – – – 0.24 (0.10–0.58) Public only – – – 0.66 (0.44–0.99) Private/military – – – 1.0 Doctor recommendation <.001 Yes 9.24 (6.63–12.88) 10.56 (7.47–14.92) – No 1.0 1.0 – Discussion of uncertainty <.001 Yes 5.42 (3.28–8.98) 38.79 (23.57–63.83) – No 1.0 1.0 – Discussion of advantages/disadvantages <.001 None – – – 1.0 Advantages or disadvantages – – – 5.30 (3.26–8.60) Both – – – 38.23 (23.49–62.22) -
OR=odds ratio.
-
↵a Multivariable polytomous logistic regression model with discussion of advantages and disadvantages of PSA screening as the dependent variable (n = 3,260); analyses adjusted for age, education, poverty ratio, self-reported health status, number of chronic diseases, personal history of cancer, family history of prostate cancer, health insurance, usual source of medical care.
-
↵b Multivariable logistic regression model with discussion of uncertainty about PSA screening as the dependent variable (n = 3,260); analyses adjusted for age, poverty ratio, self-reported health status, number of chronic diseases, personal history of cancer, family history of prostate cancer, usual source of medical care.
-
↵c Wald χ2 test for association.
-
The Article in Brief
National Evidence on the Use of Shared Decision Making in Prostate-Specific Antigen Screening
Paul K. J Han , and colleagues
Background The prostate-specific antigen (PSA) test, which screens for prostate cancer, has limited accuracy, and there is conflicting evidence for its effectiveness in reducing mortality. Because of the nature of prostate cancer, PSA screening can lead to overdiagnosis and unnecessary evaluation and treatment. Professional organizations therefore recommend that clinicians inform patients about the pros, cons, and uncertainties of PSA screening, and that screening decisions be based on patient preferences. This study examines the prevalence of shared decision making in both PSA screening and nonscreening, as well as patient characteristics associated with shared decision making.
What This Study Found Most US men report little shared decision making in PSA screening, and the absence of shared decision making is more prevalent in men who are not screened. Nearly two-thirds of men report no past physician-patient discussion of advantages, disadvantages, or scientific uncertainty of PSA screening (no shared decision making); 28 percent report discussion of 1 to 2 elements (partial shared decision making); and 8 percent report discussion of 3 elements (full shared decision making). Forty-four percent of participants report no PSA screening, 28 percent report less than annual screening, and 25 percent report nearly annual screening. The extent of shared decision making is associated with black race, Hispanic ethnicity, higher education, health insurance, and physician recommendation. Screening intensity is associated with older age, higher education, usual source of medical care, and physician recommendation, as well as with partial shared decision making.
Implications
- These findings, the authors assert, justify a broader policy debate about PSA screening. Much of the debate has focused on the absence of shared decision making in PSA screening and the potential harm of undesired and unnecessary treatment. This study suggests the more prevalent problem is the absence of shared decision making in nonscreening--the harm of which is the failure to allow individuals to decide for themselves whether screening is beneficial.
Supplemental Table
Supplemental Table 1. Factors Associated With PSA Screening Intensity (Unadjusted Analyses), 2010 National Health Interview Survey
Files in this Data Supplement:
- Supplemental data: Table - PDF file, 1 page, 184 KB




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Transcriptome-Wide Association Analysis Identifies Novel Candidate Susceptibility Genes for Prostate-Specific Antigen Levels in Men Without Prostate Cancer
- Diagnosing prostate cancer in asymptomatic patients
- Effect of a Prostate Cancer Screening Decision Aid for African-American Men in Primary Care Settings
- Prostate cancer screening with prostate-specific antigen (PSA) test: a systematic review and meta-analysis
- Prostate-Specific Antigen Testing Initiation and Shared Decision-Making: Findings from the 2000 and 2015 National Health Interview Surveys
- Recent Patterns in Shared Decision Making for Prostate-Specific Antigen Testing in the United States
- Updated Review of Prevalence of Major Risk Factors and Use of Screening Tests for Cancer in the United States
- In This Issue: A Diversified Portfolio
- Shared Decision Making, Contextualized